Roots Prefixes And Suffixes
- 1 Roots Prefixes And Suffixes —
- 2 What you'll learn —
- 3 Blueprint mapping —
- 4 Why it matters —
- 5 Key Terms & Must-Know Facts —
- 6 Key terms —
- 7 Must-know facts —
- 8 Core content —
- 9 1.1.1.1 Foundations: how to break a medical term into usable coding clues —
- 10 1.1.1.2 Foundational patterns: high-yield prefixes and suffixes that flip meaning —
- 11 1.1.1.3 Application: using roots to identify body systems and likely codebook sections —
- 12 1.1.1.4 Application: decoding procedure language from suffixes and operation clues —
- 13 1.1.1.5 Integration: translating terminology into diagnosis-vs-symptom-vs-status coding lo —
- 14 1.1.1.6 Integration: when terminology is not enough and you must not guess —
- 15 Exam Traps & Differentiators —
Why it matters
- CPC questions often hide the coding clue inside a single word part; if you miss the part, you choose the wrong section or wrong code family.
- Medical terminology is a speed tool: decoding pericarditis, arthroscopy, or hematuria quickly narrows body system, condition type, and documentation meaning.
- Terminology protects compliance: coders must not invent laterality, acuity, or diagnosis severity that the documentation does not support.
- Many exam distractors differ by one prefix or suffix; recognizing that one difference often resolves the item immediately.
Exam takeaway: Break an unfamiliar term into prefix, root, and suffix before deciding what the documentation supports.
flowchart LR
A[Unfamiliar term] --> B{Prefix present?}
B -->|Yes| C[Read timing quantity location or position]
B -->|No| D[Go to root]
C --> D[Identify body part or core concept]
D --> E[Read suffix for condition procedure or status]
E --> F[Combine only documented meanings]
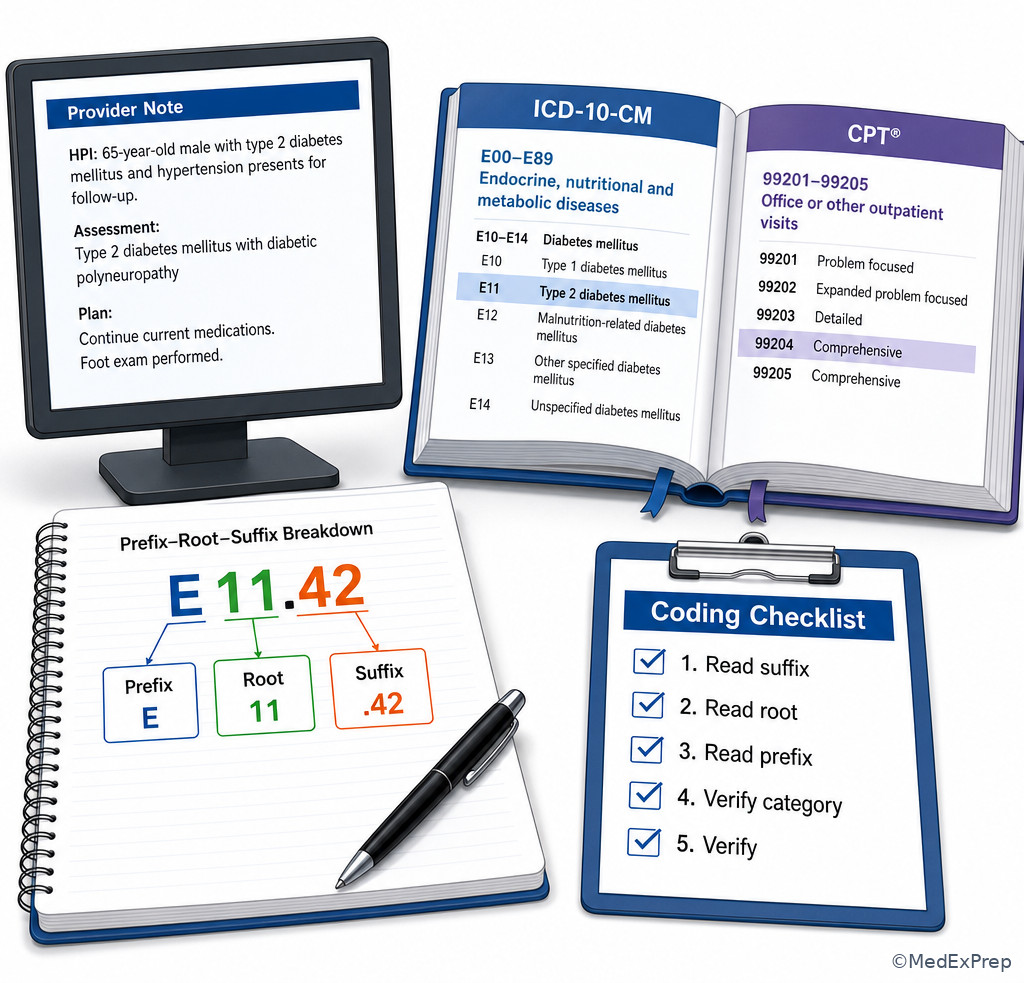
F --> G[Verify in context and codebook] See Fig 1 for the fastest CPC-friendly decoding sequence.
Key Terms & Must-Know Facts
1.1.1.1 Key terms
- Root: core meaning, often body part or base concept
- Prefix: beginning word part that changes location, quantity, time, or status
- Suffix: ending word part that signals condition, procedure, specialty, or record type
- Combining vowel: usually “o”; links parts for pronunciation, not meaning
- Inflammation suffix: -itis
- Viewing procedure suffix: -scopy
- Incision suffix: -otomy
- Removal suffix: -ectomy
- Repair suffix: -plasty
- Pain suffix: -algia
- Blood condition clue: hemat-/hemo-
- Urine clue: ur-/uria
- Around prefix: peri-
- Within prefix: intra-
- After prefix: post-
1.1.1.2 Must-know facts
- The suffix usually tells you what kind of problem or service is documented.
- The root usually tells you where the problem or service is located.
- A combining vowel does not add clinical meaning.
- -otomy, -ostomy, and -ectomy are not interchangeable.
- Hyper- and hypo- are classic exam traps because they flip the meaning.
- Arthr- means joint; oste- means bone; my- may mean muscle but context matters.
- Nephr- and ren- both relate to kidney; CPC items may use either form.
- Hepat- is liver; gastr- is stomach; enter- is intestine.
- Do not code a disease just because a suffix suggests one if the provider documents only a symptom or finding.
- Terminology helps you find the code section; code selection still requires index-to-tabular verification.
| Word part | Meaning | Common coding use | Trap to avoid |
|---|---|---|---|
| -itis | Inflammation | Condition type in ICD-10-CM | Do not assume infection unless documented |
| -scopy | Visual examination | Procedure family clue in CPT | Not the same as excision or biopsy |
| -ectomy | Removal/excision | Surgical service selection | Do not confuse with incision |
| -otomy | Cutting into/incision | Approach or access clue | Not a permanent opening |
| -ostomy | Surgically created opening | Status or procedure distinction | Not interchangeable with -otomy |
| -plasty | Repair/reconstruction | Procedure intent | Not automatically cosmetic |
| hyper- | Excessive/above normal | Severity or abnormal level clue | Opposite of hypo- |
| hypo- | Deficient/below normal | Abnormal low state | Opposite of hyper- |
Core content
1.1.1.3 Foundations: how to break a medical term into usable coding clues
A Explanation
The first CPC decision conflict is simple: Should you trust the whole unfamiliar word as a guess, or split it into parts? Always choose the split. The single rule that resolves this conflict is: suffix tells the action or condition, root tells the site, prefix refines the circumstance. For coding, that matters because a term may point you toward a diagnosis family, a procedure family, or a documentation query need. For example, arthroscopy is not “joint surgery in general”; the suffix -scopy narrows it to visual examination, and the root arthr- identifies joint. That distinction will matter later when you compare scope, biopsy, excision, and repair language in CPT. WHY THIS IS TESTED: exam stems often present an unfamiliar term and ask you to identify the body system or type of service before code selection begins.
Choose the meaning supported by all visible parts. Reject meaning based on sound-alike intuition. Nephritis and nephrectomy both involve the kidney root, but one is a diagnosis and the other is a removal procedure. A coder who notices only the root will choose the wrong code set. Similarly, the combining vowel “o” in gastroenterology makes pronunciation smoother but does not add an extra body site. For board-style logic, read from the end first, then identify the root, then add any prefix nuance. See Fig 1.
B Worked example
A 67-year-old man with hypertension, obesity, and chronic knee osteoarthritis is seen in an orthopedic clinic. The assessment lists “diagnostic arthroscopy of left knee for persistent pain; prior MRI outside facility showed degenerative changes.” The note also mentions mild anemia and a remote appendectomy. The task is to interpret the key term, not to code the full service yet. Identify task: determine what the word supports. Extract key facts: arthr- = joint, -scopy = visual examination, left knee = site/laterality context. Apply rule: the suffix resolves whether this is viewing vs removal or repair. Eliminate distractors: do not read it as arthroplasty because the ending is different; do not assume open surgery because the term itself signals scope language. Verify: the documentation supports a joint endoscopic/visual procedure family, specifically of the knee, and later CPT verification would depend on exact findings and any additional services performed.
C Exam trap
D Checkpoint
Question: A provider documents “cystoscopy performed for hematuria.” Which interpretation is most accurate before code lookup?
- A bladder inflammation procedure because cyst- implies cystitis.
- A visual examination of the urinary bladder because cyst- refers to bladder and -scopy refers to viewing.
- A surgical creation of a bladder opening because -ostomy is implied by endoscopic access.
- A bladder excision because instrumentation always means tissue removal.
Answer: B
- A: Tempting because cyst- can make learners think of cystitis; wrong because the suffix is -scopy, not -itis.
- B: Tempting and correct because it uses both root and suffix accurately.
- C: Tempting because endoscopic procedures involve entry; wrong because -ostomy is not documented.
- D: Tempting because many scopes can include interventions; wrong because the documented term alone supports viewing, not excision.
1.1.1.4 Foundational patterns: high-yield prefixes and suffixes that flip meaning
A Explanation
Many CPC items are not hard because the term is rare; they are hard because one small prefix flips the meaning. The decision conflict is: Do two similar-looking terms belong to the same concept family, or does the prefix change the coding meaning enough to reject that choice? The single rule is: prefixes often control degree, position, time, or number, and a wrong prefix can reverse the answer. Hyperglycemia and hypoglycemia share the same root and suffix pattern, but the prefix changes the clinical state. Prenatal and postnatal share the same root, but timing changes completely. Bilateral, unilateral, and contralateral are frequent documentation clues that affect codebook navigation and laterality logic.
High-yield suffixes also separate service types: -gram is the record, -graph is the instrument, and -graphy is the process of recording. A coder who sees angiography but thinks angiogram may misread what the documentation is actually naming. Likewise, -oma generally signals a mass or tumor, while -megaly indicates enlargement; those are not interchangeable documentation meanings. WHY THIS IS TESTED: exam writers like near-match answer choices that differ by one prefix or suffix because the item tests precision rather than memorization.
See Fig 2 for a comparison of commonly confused affixes.
Exam takeaway: The best answer is often separated from the trap by one prefix or suffix that flips degree, timing, or service type.
flowchart TD A[Look alike terms] --> B[hyper vs hypo] A --> C[pre vs post] A --> D[-ectomy vs -otomy vs -ostomy] A --> E[-gram vs -graphy] B --> F[High vs low] C --> G[Before vs after] D --> H[Remove vs cut into vs create opening] E --> I[Record vs process]
B Worked example
A 54-year-old woman with type 2 diabetes, stage 2 chronic kidney disease, and hyperlipidemia presents to family medicine. The note lists “episodes of symptomatic hypoglycemia after missed lunch” and also documents “history of hyperglycemia last month” in the medication review. Her blood pressure today is mildly elevated, and a healing forearm bruise is noted after a fall. Identify task: determine the correct current terminology meaning. Extract key facts: the active assessment for today is hypoglycemia; the hyperglycemia mention is historical. Apply rule: hypo- means low, hyper- means high. Eliminate distractors: do not code by the more familiar chronic diabetic pattern if the current documented problem is the opposite. Verify: terminology must match the documented state and timing, not what seems more common.
C Exam trap
D Checkpoint
Question: Which pair is interpreted correctly for coding purposes?
- Nephrotomy = kidney removal; nephrectomy = incision into the kidney.
- Prenatal = after birth; postnatal = before birth.
- Electrocardiography = process of recording heart electrical activity; electrocardiogram = the resulting record.
- Hypotension = elevated blood pressure because “tension” means force.
Answer: C
- A: Tempting because both terms involve kidney procedures; wrong because the suffix meanings are reversed.
- B: Tempting because pre/post are easy to swap under time pressure; wrong because the timing meanings are reversed.
- C: Tempting and correct because -graphy is the process and -gram is the record.
- D: Tempting because “tension” sounds forceful; wrong because hypo- means low.
- The suffix for inflammation is ____.
- True or False: -ostomy and -otomy mean the same thing.
- Name the difference between -gram and -graphy.
1.1.1.5 Application: using roots to identify body systems and likely codebook sections
A Explanation
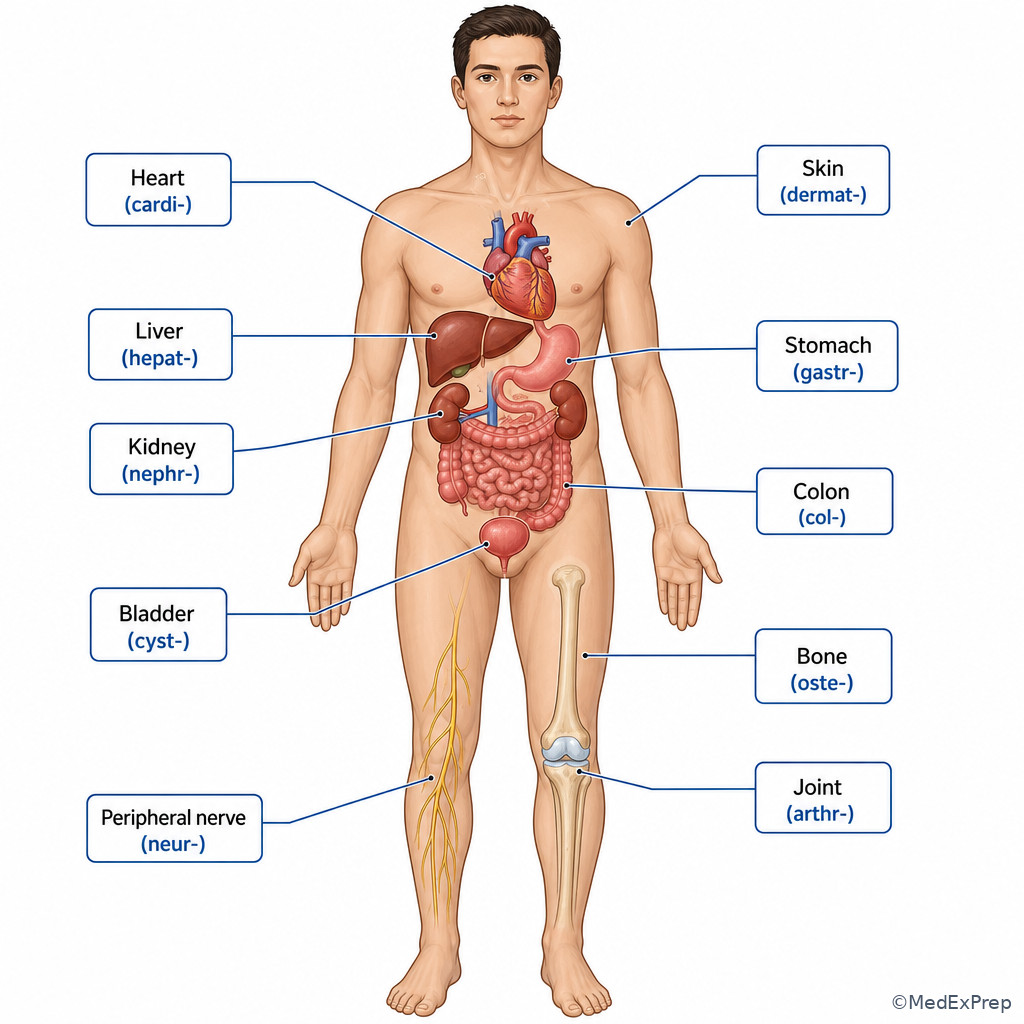
Once you can decode the parts, the next CPC decision conflict is: Which codebook section or body system should you open first? The single resolving rule is: the root usually points to the organ, tissue, or body system that anchors your search. If you see dermat-, think skin; cardi-, heart; neur-, nerve; arthr-, joint; oste-, bone; hepat-, liver; gastr-, stomach; col/o, colon; nephr-/ren-, kidney; cyst-, bladder in many contexts. For outpatient coding, this helps you pick the likely diagnosis chapter family or procedure section before detailed verification.
This does not mean root alone is enough for code assignment. Root is your map, not your final answer. For example, myalgia and myotomy may both contain my-, but one points toward a symptom and one toward a procedure. Another trap is that some roots have more than one form: kidney may appear as nephr- or ren-; uterus may appear as hyster- or metr-. WHY THIS IS TESTED: coders must connect medical language to codebook organization quickly without inventing details.
See Fig 3 for a body-system map and use it as a retrieval tool rather than a memorization list.
Exam takeaway: Use the root to choose the most likely body system first, then let the suffix decide diagnosis vs symptom vs procedure.
mindmap root((Root)) cardi heart dermat skin neur nerve arthr joint oste bone hepat liver gastr stomach nephr kidney cyst bladder col colon
Exam takeaway: Associate common roots with the correct organ system so you can open the right codebook section faster.
B Worked example
A 43-year-old woman with asthma and migraine history presents to gastroenterology for “colonoscopy with biopsy of sigmoid lesion.” The note also mentions seasonal allergies and a recent ankle sprain. Identify task: determine the likely body system and procedure family from terminology. Extract key facts: col/o points to colon; -scopy indicates visual examination; biopsy is an added procedural detail. Apply rule: root gets you to digestive system logic; suffix distinguishes visualization from open excision. Eliminate distractors: do not drift into urinary because “cysto-” is not present; do not reduce the entire service to “biopsy” without recognizing the endoscopic family. Verify: digestive endoscopy is the correct starting section, with later CPT verification based on exact scope depth and intervention.
C Exam trap
D Checkpoint
Question: Which documented term most directly points a coder to the musculoskeletal system?
- Neuritis
- Arthroplasty
- Hepatomegaly
- Cystitis
Answer: B
- A: Tempting because nerve-related services sometimes involve extremities; wrong because neur- points to nerve, not joint or bone.
- B: Tempting and correct because arthr- identifies a joint and -plasty indicates repair/reconstruction.
- C: Tempting because enlargement sounds structural; wrong because hepat- points to liver.
- D: Tempting because bladder conditions may present with pain; wrong because cyst- here points to bladder.
1.1.1.6 Application: decoding procedure language from suffixes and operation clues
A Explanation
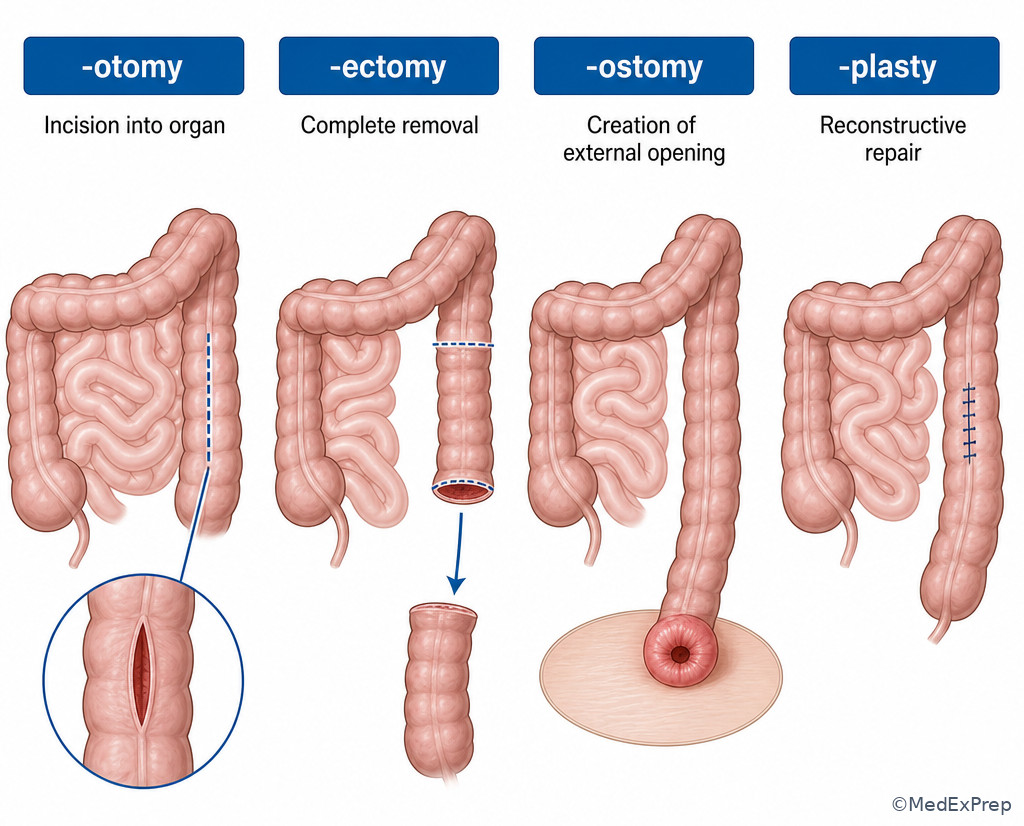
This is one of the most testable transitions from terminology into CPT logic. The decision conflict is: When several procedures involve the same organ, how do you know which procedural concept is actually documented? The single resolving rule is: the suffix and operation word tell the intent of the service. -ectomy means removal, -otomy means incision into, -ostomy means creation of an opening, -plasty means repair or reconstruction, -desis means binding/fusion, and -pexy means fixation. These are not stylistic variations. They describe different services and often different CPT families.
For example, tracheotomy is incision into the trachea; tracheostomy is creation of an opening. On a CPC item, that single suffix difference may be the entire question. Likewise, appendectomy is removal of the appendix, whereas appendotomy would mean incision into it. The practical coding rule: choose the exact operation documented; reject “close enough” procedure language. WHY THIS IS TESTED: CPT distractors commonly present same-site procedures with different operative intents.
See Fig 4 for the highest-yield procedure suffix comparisons.
Exam takeaway: Same organ does not mean same procedure—operative suffixes separate removal, incision, opening, repair, and fixation.
flowchart TB
A[Procedure term] --> B{Suffix}
B --> C[-ectomy = removal]
B --> D[-otomy = incision into]
B --> E[-ostomy = create opening]
B --> F[-plasty = repair]
B --> G[-pexy = fixation]
B --> H[-desis = fusion]
C --> I[Choose removal family]
D --> J[Choose incision family]
E --> K[Choose opening/status family] Exam takeaway: Visualize how incision, removal, repair, and opening are different operative intents even when the same organ is involved.
B Worked example
A 58-year-old man with COPD, tobacco dependence, and GERD undergoes ENT surgery. The operative note summary states “planned tracheostomy performed after difficult airway access; no tracheal mass excised.” The chart also lists chronic hoarseness and a remote wrist fracture. Identify task: determine the documented operative intent. Extract key facts: trache- = trachea; -ostomy = creation of an opening; explicit statement that no mass was excised rules out removal. Apply rule: same site does not equal same service. Eliminate distractors: reject tracheotomy if the final procedure is an opening/stoma, not merely an incision; reject excision because the note says none was done. Verify: terminology plus operative wording supports an opening procedure family.
C Exam trap
D Checkpoint
Question: Which interpretation is most accurate?
- Gastroplasty indicates removal of the stomach.
- Nephropexy indicates fixation of the kidney.
- Arthrodesis indicates visual examination of a joint.
- Colostomy indicates incision into the colon only.
Answer: B
- A: Tempting because surgery often implies removal; wrong because -plasty indicates repair/reconstruction.
- B: Tempting and correct because -pexy means fixation and nephr- means kidney.
- C: Tempting because joint procedures are often scoped; wrong because -desis means fusion/binding.
- D: Tempting because both involve entering the colon; wrong because -ostomy means creating an opening, not just incision.
- -ectomy means ______.
- True or False: -plasty always means cosmetic surgery.
- Name the key difference between -otomy and -ostomy.
1.1.1.7 Integration: translating terminology into diagnosis-vs-symptom-vs-status coding logic
A Explanation
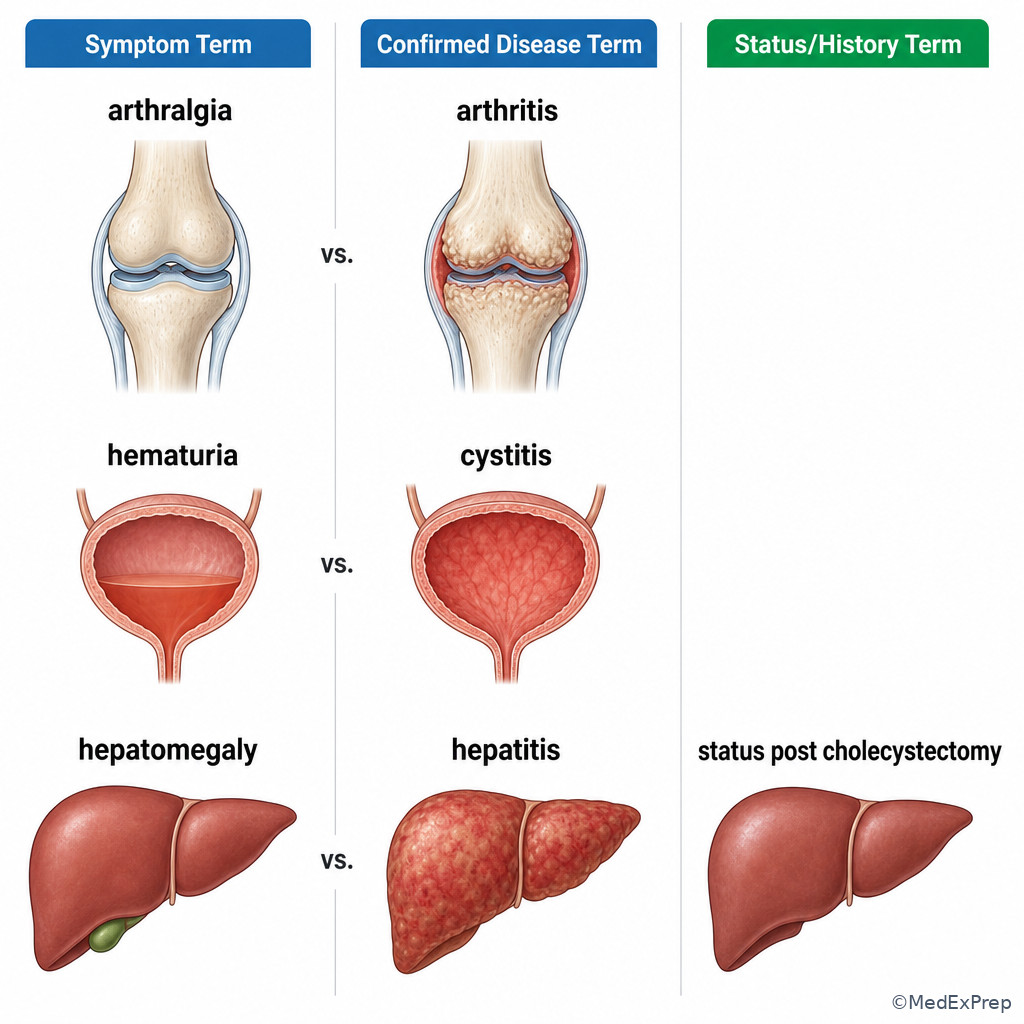
At this stage, terminology becomes a documentation support tool. The decision conflict is: Does the documented term support a disease, a symptom, a status/history concept, or not enough information at all? The single rule is: code only the category actually documented by the terminology and context. A suffix like -algia points to pain, usually a symptom concept. -emia points to a blood condition. -uria points to a urine-related finding. Terms containing history of, status post, or presence of shift you away from active disease logic and toward status/history logic when appropriate. Terminology can narrow the search, but it cannot upgrade the documentation.
Example: “hematuria” means blood in urine. It does not by itself document a kidney stone, urinary infection, or bladder cancer. “Arthralgia” means joint pain; it does not equal arthritis. “Hepatomegaly” means enlarged liver; it does not establish hepatitis or cirrhosis. WHY THIS IS TESTED: CPC questions frequently tempt learners to jump from a descriptive term to a more specific diagnosis that is clinically plausible but undocumented.
This is where coder discipline matters most. Terminology can guide your search, but outpatient coding requires documented certainty. If the provider writes “rule out appendicitis” in an outpatient setting, you do not code appendicitis based on a root and suffix pattern. You code the documented sign, symptom, or reason for encounter according to official outpatient rules. See Fig 5.
Exam takeaway: Terminology narrows meaning, but coding still depends on whether the note supports an active diagnosis, symptom, or status/history concept.
flowchart LR
A[Documented term] --> B{Suffix/context}
B --> C[-algia or symptom wording]
B --> D[-itis or active disease wording]
B --> E[history status post presence of]
B --> F[suspected rule out possible]
C --> G[Symptom logic]
D --> H[Active diagnosis logic if documented]
E --> I[Status or history logic]
F --> J[Outpatient certainty rule: do not code as confirmed disease] Exam takeaway: A term such as pain, enlargement, or blood in urine does not automatically justify coding a more specific disease.
B Worked example
A 29-year-old woman with endometriosis history and prior C-section presents to urgent care with dysuria and visible blood in the urine. The assessment states “hematuria and dysuria; possible cystitis, urine culture pending.” She also reports mild back soreness after moving furniture, and her pregnancy test is negative. Identify task: determine what terminology actually supports today. Extract key facts: active documented terms are hematuria and dysuria; cystitis is possible, not confirmed. Apply rule: blood in urine is a finding, not proof of infection. Eliminate distractors: reject a confirmed infection code if the note preserves diagnostic uncertainty in the outpatient setting. Verify: code the supported symptom/finding logic, not the suspected cause.
C Exam trap
D Checkpoint
Question: Which term most clearly represents a symptom rather than a confirmed disease?
- Arthralgia
- Arthritis
- Nephritis
- Dermatitis
Answer: A
- A: Tempting and correct because -algia means pain, which is a symptom category.
- B: Tempting because joint problems often present with pain; wrong because -itis indicates inflammation, a disease condition if documented as such.
- C: Tempting because it involves a body-system root like the others; wrong because it names kidney inflammation, not merely a symptom.
- D: Tempting because skin conditions may be mild; wrong because it is still an inflammatory diagnosis term.
1.1.1.8 Integration: when terminology is not enough and you must not guess
A Explanation
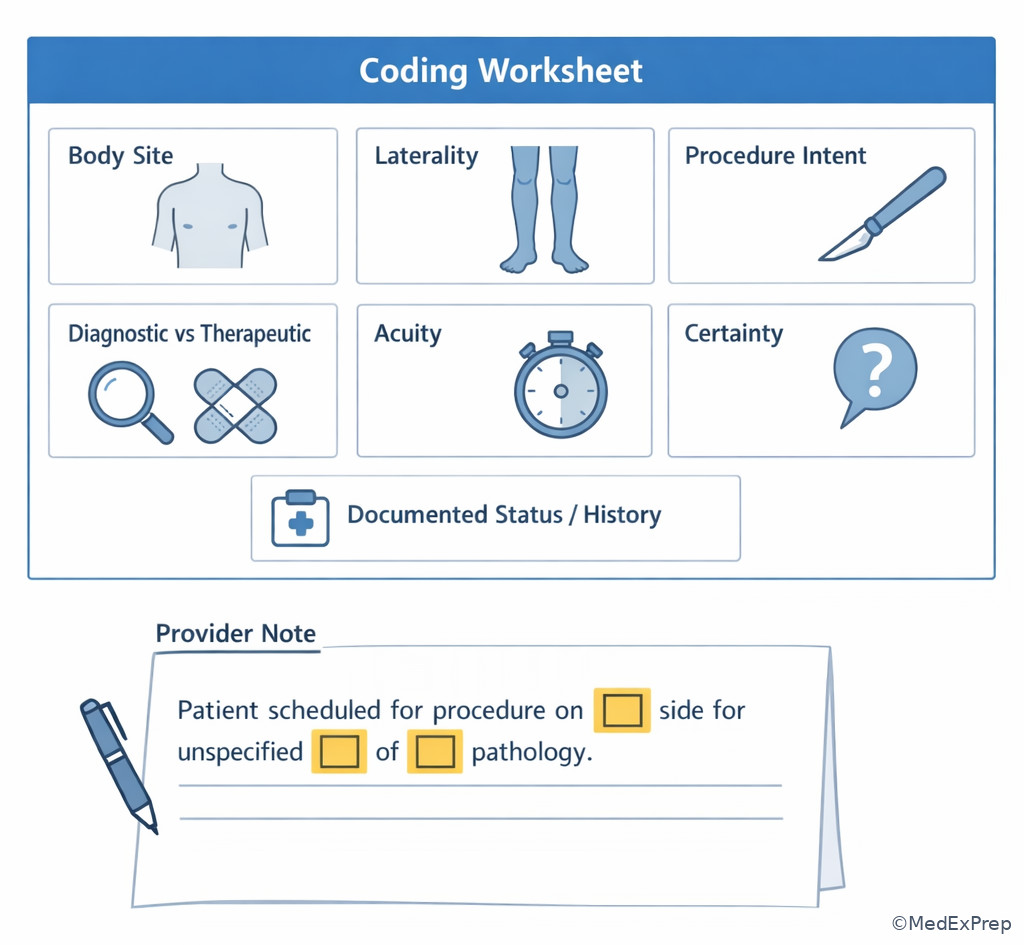
The final decision conflict is one every ethical coder faces: Does terminology give enough support to assign a specific code, or does the record stop short? The single resolving rule is: if a term is incomplete, ambiguous, contradictory, or nonfinal, do not guess beyond documentation support. A root may identify the organ and a suffix may identify general type, but you may still lack laterality, approach, acuity, episode, exact site, or whether a service was diagnostic vs therapeutic. Terminology is a guide, not permission to infer.
Examples: “knee scope” may suggest arthroscopy, but if the final procedure note does not confirm diagnostic vs surgical intervention, you cannot fill in the missing work. “Renal mass” is not the same as kidney cancer. “Lesion removed” does not tell you biopsy vs destruction vs excision without more operative detail. “Otalgia” does not equal otitis media. WHY THIS IS TESTED: CPC items often reward restraint. The best answer is sometimes “insufficient documentation” or the less specific supported interpretation.
In practice, this is where provider clarification would be needed. On the exam, the correct move is to reject options that rely on undocumented assumptions. See Fig 6 for a decision tree on when terminology is enough and when it is not.
Exam takeaway: When terminology identifies the concept but not the required specifics, choose the supported level or recognize the need for clarification.
flowchart TD
A[Decoded term] --> B{Enough documented detail?}
B -->|Yes| C[Search exact supported code family]
B -->|No| D{Can a supported less specific option be used?}
D -->|Yes| E[Use supported level only]
D -->|No| F[In practice query or escalate]
C --> G[Verify notes conventions and context] Exam takeaway: A decoded term still needs enough detail on site, intent, laterality, and certainty before final code selection.
B Worked example
A 71-year-old man with atrial fibrillation, benign prostatic hyperplasia, and chronic tobacco use is seen by urology. The note says “bladder lesion treated endoscopically,” but the operative summary does not state whether the lesion was biopsied, fulgurated, or excised; pathology is pending. A distracting note mentions prior hematuria workup and stable kidney cysts. Identify task: decide whether terminology alone supports a specific procedure choice. Extract key facts: bladder root/site is clear; endoscopic approach is suggested; exact intervention is not documented. Apply rule: do not infer biopsy or excision from the word “treated.” Eliminate distractors: reject answers that assume the final operative intent. Verify: the documentation is insufficient for a more specific procedural assignment without further detail.
C Exam trap
D Checkpoint
Question: A provider documents “possible nephrolithiasis, hematuria present, imaging pending” in an outpatient visit. What is the best coding interpretation based on terminology rules alone?
- Code confirmed nephrolithiasis because the term is clinically likely.
- Code kidney cancer because hematuria suggests a renal source.
- Use the documented supported finding/symptom logic rather than coding the possible diagnosis as confirmed.
- Assign a stone removal procedure because the workup is for nephrolithiasis.
Answer: C
- A: Tempting because the provider names a suspected cause; wrong because outpatient certainty rules do not allow coding it as confirmed.
- B: Tempting because hematuria can raise concern for malignancy; wrong because cancer is nowhere documented.
- C: Tempting and correct because the note supports symptoms/findings, not a final stone diagnosis.
- D: Tempting because a urologic workup may lead to intervention; wrong because no procedure was documented.
Exam Traps & Differentiators
Most common wrong answer and why: choosing a term that shares the same root but has a different suffix. This is tempting because the body site feels familiar, but the suffix is what changes diagnosis to symptom, symptom to procedure, or one procedure family to another.
| Looks similar | But isn't | Single clue | Coding impact |
|---|---|---|---|
| Arthralgia | Arthritis | -algia = pain; -itis = inflammation | Symptom vs disease logic |
| Nephrotomy | Nephrectomy | -otomy = incision; -ectomy = removal | Different CPT procedure family |
| Tracheotomy | Tracheostomy | -ostomy = opening created | Different operative intent |
| Electrocardiogram | Electrocardiography | -gram = record; -graphy = recording process | Documentation interpretation nuance |
| Hypoglycemia | Hyperglycemia | Prefix flips low vs high | Wrong diagnosis family if missed |
| Hematuria | Cystitis | Finding vs confirmed diagnosis | Do not infer disease from symptom |
- If the stem says “possible,” “suspected,” or “rule out” in outpatient documentation, think supported symptom/finding logic rather than confirmed disease.
- If the stem says “scope,” “visualization,” or -scopy, think endoscopic/inspection family before assuming excision.
- If the stem says “status post” or “history of,” think status/history wording rather than active disease.
- If the stem says “repair,” “reconstruction,” or -plasty, think restoration, not removal.
- If the stem says a root you know but an unfamiliar ending, think “read the suffix before choosing the code set.”
Related upcoming trap: in Eponyms Abbreviations And Symbols, a familiar abbreviation may look helpful but still be too ambiguous to support code assignment. The same discipline applies here: readable does not always mean reportable.
Tables
| High-yield suffix | Meaning | Typical coding implication |
|---|---|---|
| -algia | Pain | Usually symptom logic |
| -emia | Blood condition | Lab/condition meaning; verify context |
| -megaly | Enlargement | Finding/condition, not necessarily cause |
| -oma | Tumor/mass | Neoplasm or mass clue; verify pathology wording |
| -osis | Condition/abnormal state | Broad meaning; context needed |
| -pathy | Disease/disorder | General disease concept, not mechanism |
| -uria | Urine condition/finding | Urinary finding clue |
| -rrhea | Flow/discharge | Symptom/finding language |
| Comparison | Term A | Term B | Discriminator |
|---|---|---|---|
| Degree | hyper- | hypo- | Above normal vs below normal |
| Timing | pre- | post- | Before vs after |
| Position | intra- | peri- | Within vs around |
| Number/side | uni- | bi- | One vs two |
| Procedure intent | -otomy | -ostomy | Incision vs creation of opening |
| Procedure intent | -ectomy | -plasty | Removal vs repair |
| Documented term type | What it usually supports | Common trap | Best coding mindset |
|---|---|---|---|
| Symptom term | Finding/symptom code search | Upgrading to confirmed disease | Code only what is documented |
| Inflammation term | Active condition if clearly documented | Assuming infectious cause | Use exact wording |
| Procedure term | CPT family search | Confusing site with operative intent | Suffix first, root second |
| Status/history term | Status/history logic | Treating as active disease | Honor context words |
| Uncertain diagnosis term | Outpatient symptom/finding logic | Coding as confirmed | Apply certainty rule |
| Vague lesion/mass term | Less specific supported search | Assuming malignancy or excision type | Wait for documented detail |
Algorithm / Approach
Exam takeaway: A disciplined terminology-first workflow prevents wrong-section searches and unsupported specificity.
Rapid Review
- -scopy → viewing/inspection, not automatic excision
- -ectomy → removal, not repair
- -otomy → incision into, not permanent opening
- -ostomy → surgically created opening, not simple incision
- -algia → symptom clue, often pain
- -itis → inflammation term, not necessarily infection
- hyper- → high/excessive, opposite of hypo-
- pre- → before, opposite of post-
- root → body system map, not final code
- combining vowel → pronunciation helper, not meaning clue
- history/status words → do not treat as active disease
- possible/suspected outpatient diagnosis → do not code as confirmed disease
- vague procedure wording → operative intent must be documented
Self-check quiz
1. A 45-year-old woman with obesity and seasonal allergies is seen for follow-up after urgent care. The note lists “persistent arthralgia of the right shoulder” and separately documents a past history of dermatitis. Which interpretation is most appropriate?
- Arthralgia indicates joint pain.
- Arthralgia indicates joint inflammation.
- Arthralgia indicates joint repair.
- Arthralgia indicates joint fusion.
2. A 60-year-old man with hypertension, GERD, and a remote cholecystectomy undergoes “diagnostic bronchoscopy” for chronic cough. Which word-part interpretation best supports the documented service?
- bronch- = bronchus; -scopy = visual examination
- bronch- = lung removal; -scopy = tissue destruction
- bronch- = pleura; -scopy = reconstruction
- bronch- = mediastinum; -scopy = incision
3. A 33-year-old woman with migraine, anxiety, and prior nephrolithiasis presents to clinic for dysuria and visible blood in the urine. The assessment states “hematuria, dysuria, possible cystitis; culture pending.” Which interpretation most appropriately guides coding?
- Code confirmed cystitis because hematuria strongly suggests infection.
- Use the supported symptom/finding terminology rather than coding the possible diagnosis as confirmed.
- Code pyelonephritis because the patient has a prior renal history.
- Assign a bladder biopsy procedure because urinary bleeding suggests lesion evaluation.
4. A 52-year-old man with diabetes, neuropathy, and hyperlipidemia is scheduled for “colostomy revision.” The note also mentions chronic constipation and prior colonoscopy. Which suffix interpretation best clarifies the procedure family?
- -ostomy means incision into the colon only.
- -ostomy means repair of the colon wall.
- -ostomy means creation or presence of a surgically formed opening.
- -ostomy means excision of the colon.
5. A 41-year-old woman with rheumatoid arthritis, hypothyroidism, and obesity is referred for “arthroplasty of the left hip.” A distracting note mentions prior diagnostic arthroscopy of the knee last year. Which interpretation is most appropriate?
- This term indicates visual examination of a joint.
- This term indicates reconstruction or repair of a joint.
- This term indicates inflammation of a joint.
- This term indicates fixation of a joint.
6. A 68-year-old man with COPD, atrial fibrillation, and tobacco dependence undergoes airway surgery. The operative summary states “tracheostomy created; no tracheal lesion excised.” Which interpretation is most appropriate for distinguishing the documented procedure from a close-call distractor?
- The term supports incision into the trachea only.
- The term supports creation of an opening in the trachea.
- The term supports removal of tracheal tissue.
- The term supports endoscopic visualization of the trachea.
7. A 57-year-old woman with chronic kidney disease stage 3, hypertension, and recurrent urinary tract infections is seen after imaging. The provider writes “renal mass, etiology unclear; history of hematuria.” Which terminology-based conclusion is most appropriate?
- Code kidney cancer because a mass in this setting is likely malignant.
- Code nephritis because the renal root suggests inflammatory disease.
- Recognize that the term identifies organ site but does not by itself support a specific disease category such as malignancy.
- Assign nephrectomy because renal masses are commonly removed.
8. A 49-year-old woman with type 2 diabetes, obesity, and GERD has outpatient documentation stating “episodes of hypoglycemia today; history of hyperglycemia last month.” A tempting answer choice uses the chronic diabetic pattern rather than the current term. Which interpretation is most appropriate?
- The active documented state is hyperglycemia because diabetes usually causes elevated glucose.
- The active documented state is hypoglycemia because the prefix identifies the current low-glucose episode.
- The active documented state is diabetic ketoacidosis because glucose fluctuation suggests decompensation.
- No glucose-related term is supported because the terms conflict.
Answer key
1. Correct answer: A
- A: Tempting because it is the plain-language read of the term, and it is correct. The pathophysiology/meaning is pain in a joint; the discriminating clue is the suffix -algia, which points to pain rather than inflammation. Source support: terminology conventions used in medical coding texts and official coding education emphasize symptom-vs-disease wording distinctions.
- B: Tempting because joint pain is often associated with inflammatory disorders. It is incorrect here because inflammation would be suggested by -itis, not -algia. The single clue is the ending.
- C: Tempting because orthopedic terms often describe procedures. It is incorrect because repair would require a procedural suffix such as -plasty. The clue is that this is a symptom term, not an operative term.
- D: Tempting because severe joint disease may lead to fusion. It is incorrect because fusion is associated with -desis, not -algia. The discriminating clue is again the suffix.
2. Correct answer: A
- A: Tempting and correct because it uses both root and suffix accurately. Bronch- points to the bronchus/airway, and -scopy indicates visual examination. The single clue is the suffix.
- B: Tempting because bronchoscopic procedures may involve interventions. It is incorrect because -scopy does not mean removal or destruction. The discriminating clue is “diagnostic bronchoscopy.”
- C: Tempting because thoracic structures are anatomically related. It is incorrect because neither the root nor suffix supports pleural reconstruction. The single clue is the actual root.
- D: Tempting because airways and mediastinum are close in location. It is incorrect because incision would require different operative language such as -otomy. The clue is the suffix -scopy.
3. Correct answer: B
- A: Tempting because hematuria and dysuria make cystitis clinically plausible. It is incorrect in this specific outpatient scenario because the provider documents “possible cystitis,” which does not support coding it as confirmed. The discriminating clue is the uncertainty word possible. Authoritative support: ICD-10-CM outpatient diagnosis reporting guidelines direct coders not to code uncertain diagnoses as confirmed.
- B: Tempting and correct because it follows outpatient certainty rules and terminology meaning. Hematuria and dysuria are documented findings/symptoms; they are supported regardless of the suspected cause. The clue is that only symptoms are certain.
- C: Tempting because prior nephrolithiasis may bias the reader toward upper urinary pathology. It is incorrect because pyelonephritis is neither documented nor supported by the term set in the note. The clue is absence of confirmed diagnosis wording.
- D: Tempting because urinary bleeding can lead to procedural evaluation. It is incorrect because no biopsy procedure was documented. The clue is that the stem asks for terminology-guided coding interpretation, not a future clinical step.
4. Correct answer: C
- A: Tempting because many learners confuse entry into an organ with creation of an opening. It is incorrect because incision alone would be -otomy. The discriminating clue is the suffix -ostomy.
- B: Tempting because revision procedures often involve repair. It is incorrect because the suffix does not mean repair; -plasty would fit repair language better. The clue is the exact operative ending.
- C: Tempting and correct because -ostomy indicates a surgically created opening or related stoma concept. The discriminating clue is the suffix itself.
- D: Tempting because colon surgery sometimes includes resection. It is incorrect because removal would correspond to -ectomy rather than -ostomy. The clue is the suffix mismatch.
5. Correct answer: B
- A: Tempting because the stem mentions prior arthroscopy, creating noise around another joint procedure. It is incorrect because visualization corresponds to -scopy, not -plasty. The single clue is the current term ending.
- B: Tempting and correct because -plasty indicates repair or reconstruction. The discriminating clue is the operative suffix, not the prior history.
- C: Tempting because rheumatoid arthritis is an inflammatory disorder and is included to distract. It is incorrect because inflammation would be -itis. The clue is that the term names a procedure, not a diagnosis.
- D: Tempting because orthopedic procedures can stabilize joints. It is incorrect because fixation is associated with -pexy, not -plasty. The single clue is the suffix.
6. Correct answer: B
- A: Tempting because a tracheostomy involves surgical entry into the trachea, which superficially resembles incision language. It is incorrect because the documented procedure is creation of an opening, not incision only. The discriminating clue is the suffix -ostomy.
- B: Tempting and correct because the mechanism/meaning is a surgically created tracheal opening. The clue is both the suffix and the operative wording “created.”
- C: Tempting because the stem includes a lesion reference. It is incorrect because the operative note specifically says no lesion was excised. The discriminating clue is that explicit exclusion.
- D: Tempting because airway procedures often begin with visualization. It is incorrect because the documented final service is not endoscopy. The clue is the named procedure and “created” wording.
7. Correct answer: C
- A: Tempting because renal masses can be malignant and the clinical context raises concern. It is incorrect because the documented terminology does not confirm cancer. The discriminating clue is “etiology unclear.” Authoritative support: outpatient coding requires documented certainty, not inference.
- B: Tempting because the root is renal/nephr-, which can bias the reader toward a kidney diagnosis family. It is incorrect because nephritis specifically implies inflammation, which is not documented. The clue is absence of inflammatory wording.
- C: Tempting and correct because it reflects the coder’s role: identify organ site without overcalling disease category. The discriminating clue is that “mass” is nonspecific.
- D: Tempting because nephrectomy may be performed for some renal masses. It is incorrect because no procedure was documented. The clue is that the note is diagnostic/assessment wording only.
8. Correct answer: B
- A: Tempting because diabetes is commonly associated with elevated glucose and the history mentions hyperglycemia. It is incorrect for this scenario because the active documented current episode is hypoglycemia. The discriminating clue is “today” plus the prefix hypo-.
- B: Tempting and correct because the prefix identifies the current low-glucose state and the stem contrasts it against a historical hyperglycemia mention. The single clue is timing plus prefix meaning.
- C: Tempting because severe diabetic complications are familiar board distractors. It is incorrect because ketoacidosis is not documented and would require more explicit clinical support. The discriminating clue is absence of that diagnosis.
- D: Tempting because conflicting glucose terms appear in the stem. It is incorrect because they are separated by timing: current episode vs past history. The clue is the documentation time frame.