Why it matters
- Board stems often hide the correct psychopharmacotherapy answer inside the history, not the diagnosis label.
- The safest recommendation frequently depends on one prior exposure: past response, past adverse effect, substance use pattern, pregnancy status, or adherence barrier.
- Psychiatric pharmacists are expected to identify what must be clarified before optimizing treatment, especially when withdrawal, overdose risk, suicidality, or serious drug reactions are possible.
- A well-structured history prevents common exam errors such as treating side effects as disease progression or restarting a previously harmful agent.
Key Terms & Must-Know Facts
1.1.1.1 Key terms
- Chief concern: the patient-stated reason for evaluation or medication review
- History of present illness (HPI): chronology of current symptoms, severity, triggers, and functional impact
- Past psychiatric history: prior episodes, hospitalizations, attempts, and prior diagnoses from prior clinicians
- Psychotropic medication history: past and current agents, doses, duration, response, and tolerability
- Adherence history: how consistently the patient took the regimen and why doses were missed
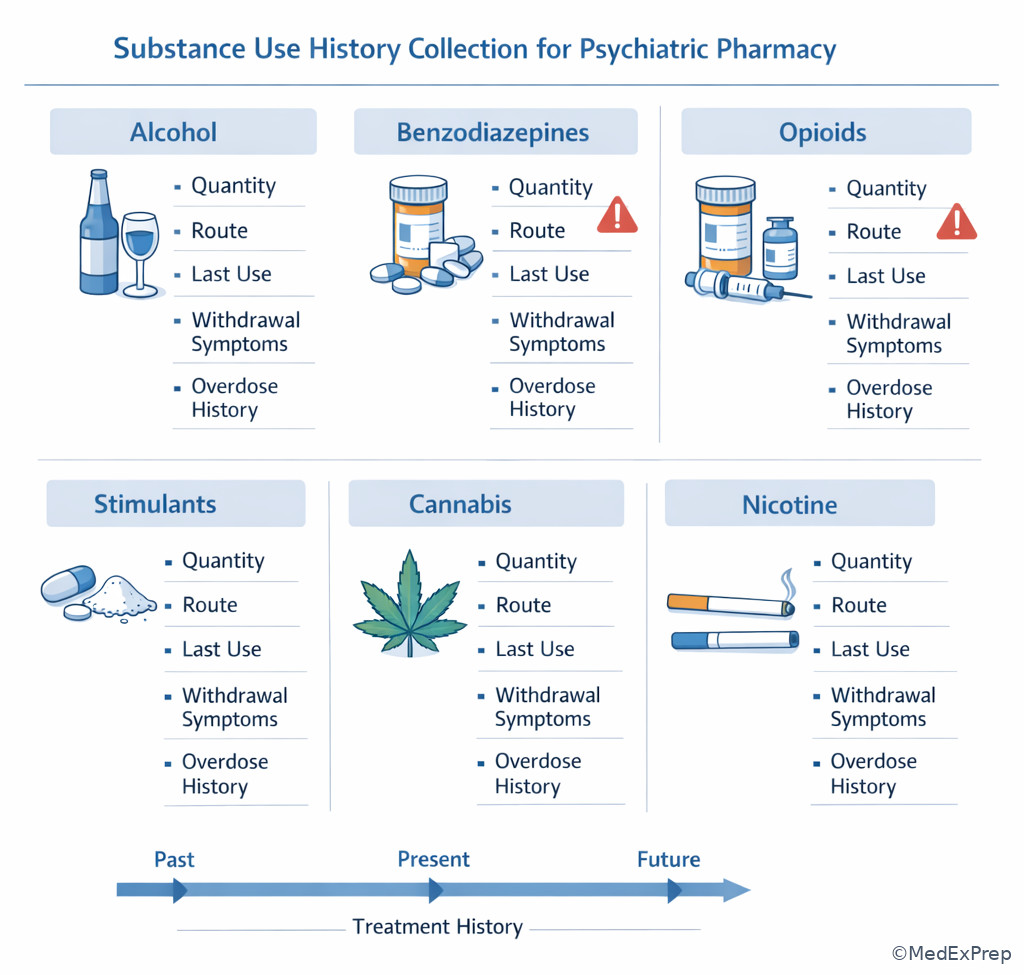
- Substance use history: alcohol, opioids, stimulants, cannabis, sedatives, nicotine, and withdrawal patterns
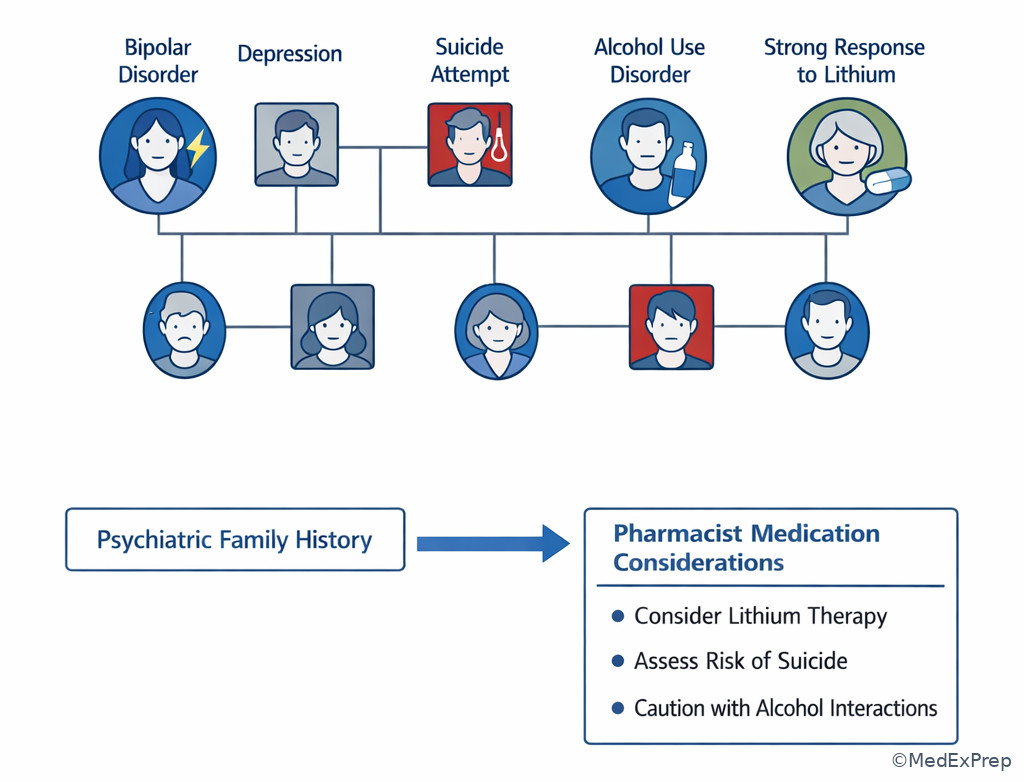
- Family psychiatric history: psychiatric illness, suicide, bipolar disorder, and medication response in relatives
- Social history: housing, support, work, trauma exposure, access, and legal or transportation barriers
- Safety history: suicidality, self-harm, violence risk, overdose, access to lethal means
- Collateral: information from family, caregivers, pharmacy fill data, charts, or outpatient team
- Medication reconciliation: verifying what is actually being taken, not just what is listed
- Withdrawal history: symptoms that occur when a substance or medication is reduced or stopped
- Treatment resistance clue: failure of adequate trials rather than simple exposure to many drugs
1.1.1.2 Must-know facts
- For exams, the most valuable psychiatric history detail is often prior medication response at an adequate dose and duration.
- A history of mania or hypomania symptoms changes antidepressant interpretation and treatment recommendations.
- Past serious reactions such as rash, NMS, serotonin syndrome, severe EPS, agranulocytosis, or prolonged QT require immediate clarification before restarting related therapy.
- Substance use history is not background noise; it can explain anxiety, insomnia, psychosis, tremor, tachycardia, or poor adherence.
- “Nonresponse” is uninterpretable without asking dose, duration, adherence, and timing of assessment.
- Recent discontinuation of SSRIs, benzodiazepines, or antipsychotics can mimic relapse.
- Family history of bipolar disorder, suicide, or strong medication response can influence pharmacist recommendations.
- History must separate what was prescribed from what the patient actually took.
- Care transition errors commonly arise from duplicate agents, omitted maintenance therapy, or undocumented PRN use.
Exam takeaway: Use history domains to identify the single medication-relevant clue that changes the safest recommendation.
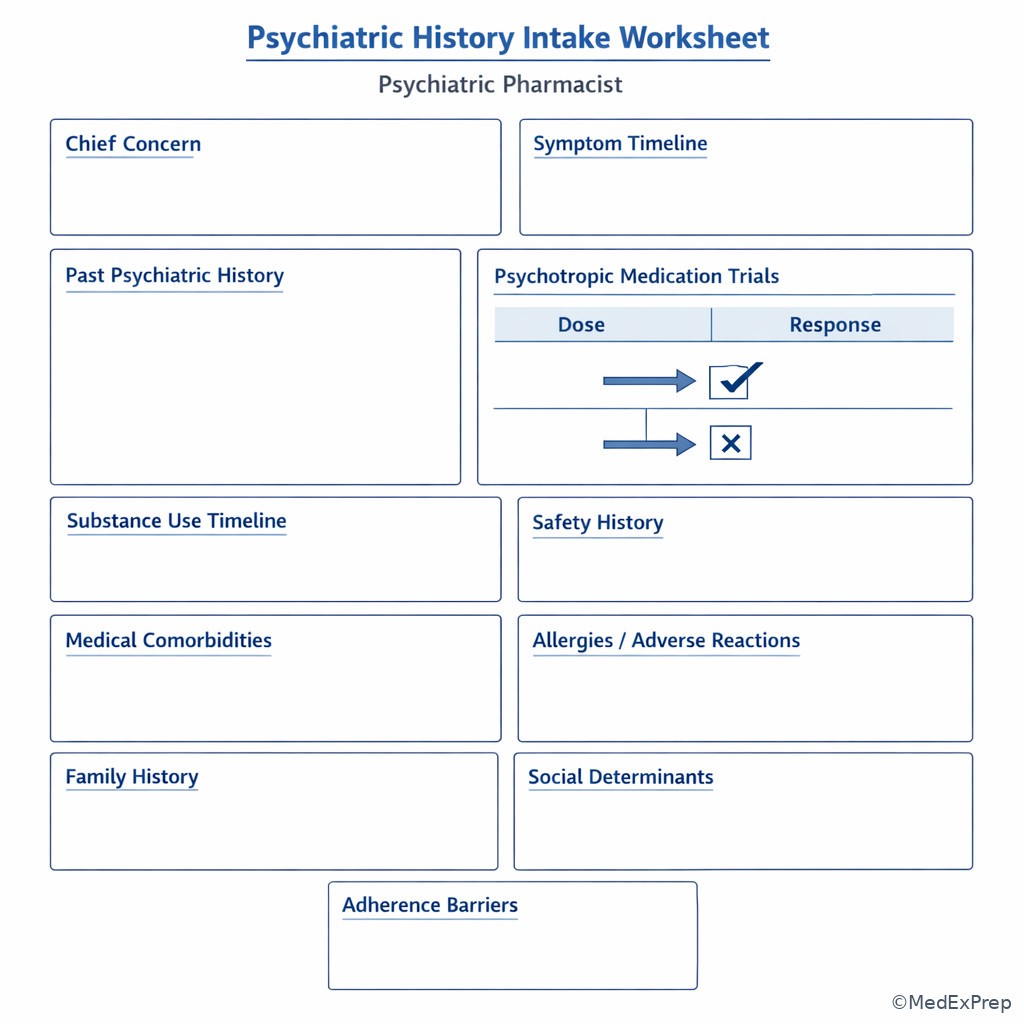
flowchart TD A[Psychiatric history stem] --> B[Current symptom timeline] A --> C[Past episodes and hospitalizations] A --> D[Medication trials and response] A --> E[Substance use and withdrawal] A --> F[Safety and access barriers] B --> G[Relapse vs side effect vs withdrawal] C --> H[Bipolarity or recurrence pattern] D --> I[Choose/reject drug based on prior response] E --> J[Intoxication or withdrawal risk] F --> K[Adherence and follow-up plan]
See Fig 1 for the global structure: on the BCPP exam, psychiatric history is not collected for completeness alone; it is collected to answer a medication question.
Exam takeaway: A prior “failed” medication trial should be rejected as evidence only if dose, duration, or adherence was inadequate.
flowchart LR
A[Prior medication listed] --> B{Adequate dose?}
B -- No --> C[Do not label true nonresponse]
B -- Yes --> D{Adequate duration?}
D -- No --> C
D -- Yes --> E{Actually taken?}
E -- No --> C
E -- Yes --> F[Interpret efficacy and tolerability]
F --> G[Reuse, augment, switch, or avoid] See Fig 2 whenever a case claims that “several meds failed.” The exam usually wants you to test whether they truly failed.
Exam takeaway: Organize the history into symptom timeline, medication exposure, substances, safety, and social barriers to avoid missing the deciding clue.
See Fig 3 as a visual checklist for what a pharmacist should verify before making a regimen recommendation.
Exam takeaway: Time course and medication/substance exposure are the fastest way to distinguish disease recurrence from withdrawal or toxicity.
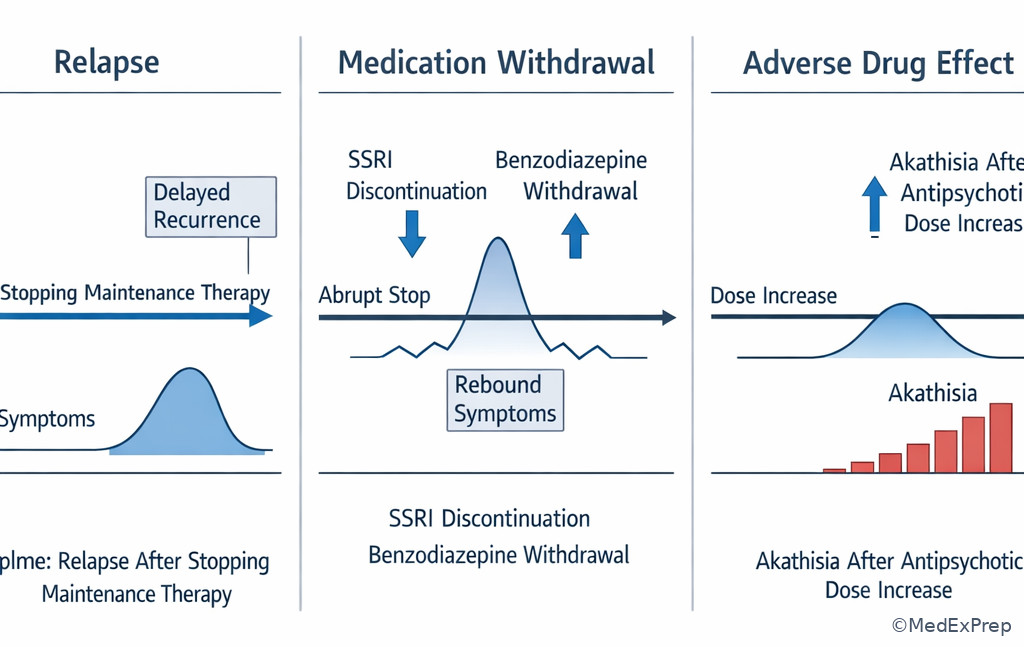
See Fig 4 for one of the highest-yield stem distinctions in psychiatric pharmacy.
Exam takeaway: Certain history findings require immediate clarification or urgent escalation before any routine medication recommendation.
flowchart TD
A[History obtained] --> B{Active suicidality, overdose, severe withdrawal, NMS, serotonin syndrome clues?}
B -- Yes --> C[Urgent escalation / notify team / emergency protocol]
B -- No --> D{Serious prior reaction or dangerous interaction risk?}
D -- Yes --> E[Hold recommendation until clarified]
D -- No --> F{Adherence or access barrier identified?}
F -- Yes --> G[Adjust regimen and follow-up plan]
F -- No --> H[Proceed with standard optimization] See Fig 5 for the safety-first sequence expected of the pharmacist candidate.
Exam takeaway: The medication list, fill history, patient report, and collateral often disagree, and reconciling them changes the best next step.
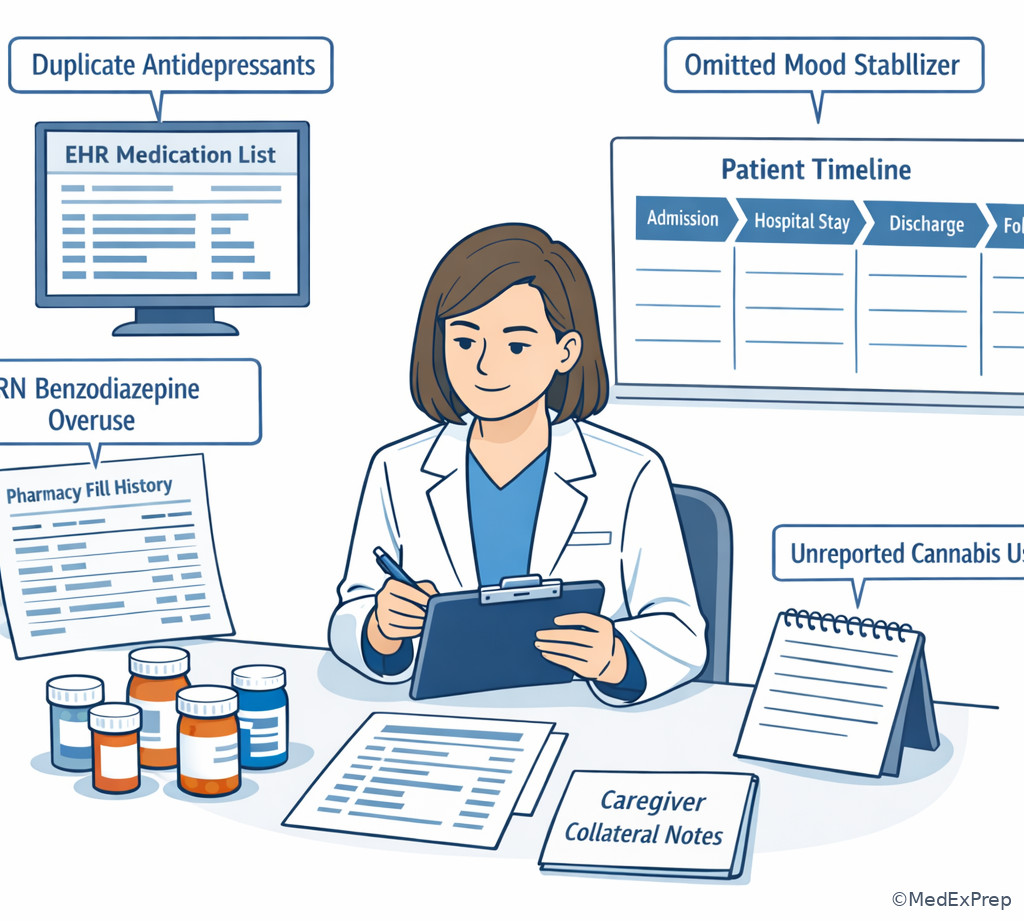
See Fig 6 when thinking about inpatient admission, discharge, or urgent ambulatory follow-up.
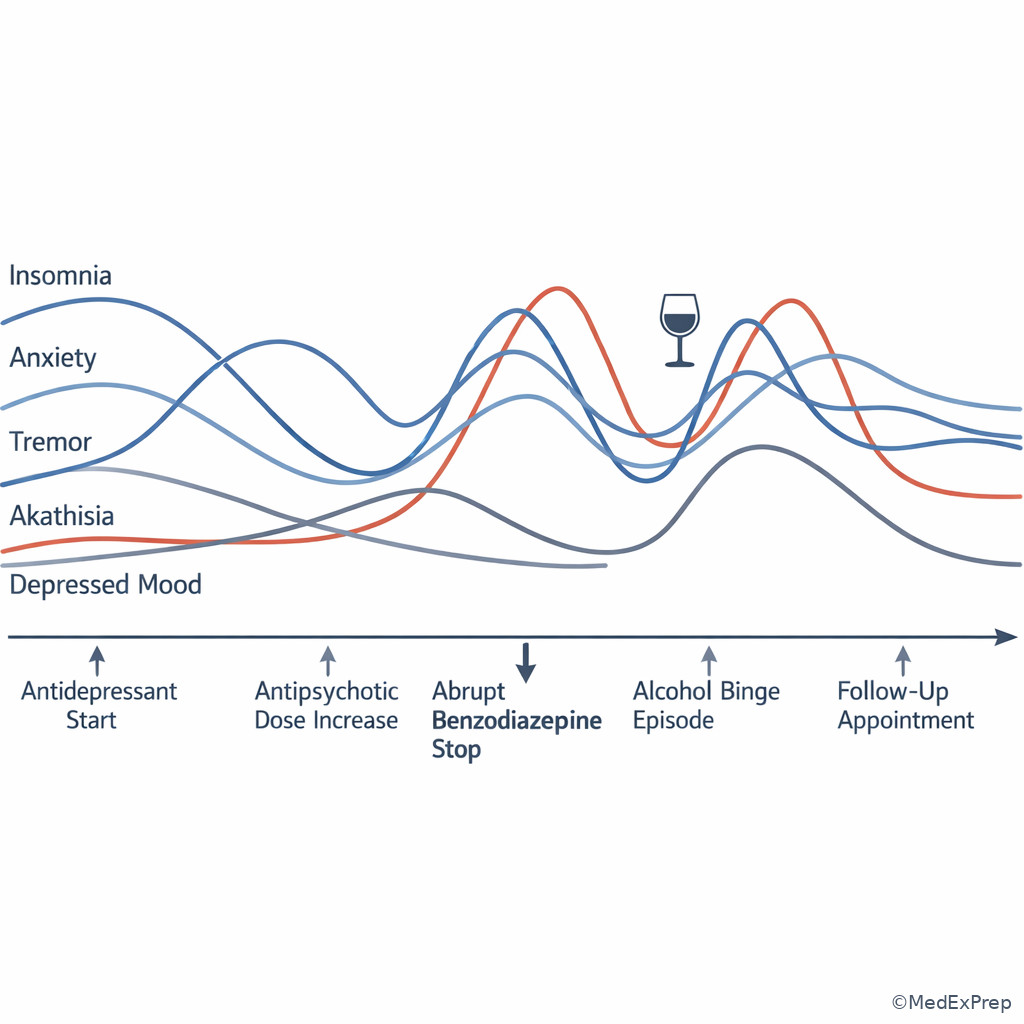
Exam takeaway: Plotting symptoms against dose changes is often enough to identify whether the problem is efficacy failure or drug-related harm.
Exam takeaway: Family history can influence suspicion for bipolarity, suicide risk, and probable medication response patterns.
Exam takeaway: Substance type, last use, quantity, and prior withdrawal complications are more useful than a vague “uses drugs” note.
Core content
1.1.1.3 Foundational structure: what belongs in a medication-relevant psychiatric history?
A Explanation
The decision conflict is simple: which history details actually change a psychopharmacotherapy recommendation, and which details are background? The resolving rule is to prioritize domains that alter safety, efficacy, adherence, or monitoring. For the BCPP exam, a psychiatric history is not a generic interview checklist. It is a framework for deciding whether a medication should be started, resumed, avoided, clarified, or escalated.
Start with the chief concern and HPI, but interpret them through a medication lens: onset, duration, severity, functional change, recent dose changes, discontinuations, missed doses, substance use, and collateral. Then ask past psychiatric history: prior episodes, hospitalizations, suicide attempts, self-harm, violence, prior manic symptoms, psychosis, or severe withdrawal. Add medical comorbidities because they change drug choice and monitoring. Finally, close the loop with social and access history: unstable housing, inability to obtain refills, caregiver burden, transportation limits, and low health literacy can make a “failed regimen” really an implementation failure.
WHY THIS IS TESTED: exam stems commonly bury the decisive clue in the history domain most learners skip: prior hypomania before an SSRI, abrupt benzodiazepine stoppage before “panic,” or a prior dystonic reaction before antipsychotic re-exposure.
B Worked example
A 34-year-old woman with generalized anxiety disorder, migraines, and hypothyroidism presents for pharmacist-led medication review after “sertraline failure.” Her active list includes sertraline 50 mg orally daily, hydroxyzine 25 mg orally at bedtime as needed, and levothyroxine 100 mcg orally daily. She reports persistent anxiety and insomnia for 3 weeks. A distracting clue is that she also drinks two large energy drinks daily. Chart review shows sertraline was started 18 days ago after she had stopped paroxetine 40 mg/day abruptly because she ran out. The task is to recommend the most appropriate next step in medication assessment.
Reasoning chain: Identify task: determine whether sertraline truly failed. Extract key facts: low-dose early sertraline exposure, abrupt paroxetine stop, insomnia/anxiety shortly after switch, stimulant intake noise. Apply rule: no medication should be labeled ineffective before adequate duration and adherence are assessed; discontinuation symptoms from prior SSRI may mimic relapse. Eliminate distractors: increasing hydroxyzine treats symptoms but ignores the timeline; switching sertraline again is premature; declaring stimulant-induced anxiety alone misses the antidepressant transition. Verify: clarify discontinuation symptoms, adherence, refill access, and whether a more gradual cross-taper or supportive management is needed.
C Exam trap
Why it is tempting: learners remember the interview outline but forget that psychopharmacotherapy hinges on prior drug response and adverse effects.
Single clue that eliminates it: if the stem asks for the best medication recommendation, the useful history is the part that changes treatment choice, especially prior trial quality and serious reactions.
D Checkpoint
Question: A pharmacist reviews a referral for “multiple antidepressant failures” in a 41-year-old man taking escitalopram 10 mg orally daily for 2 weeks. Which psychiatric history detail most requires clarification before recommending augmentation?
- Whether his father had alcohol use disorder
- Whether the escitalopram trial reached an adequate dose and duration
- Whether he prefers evening dosing
- Whether he had childhood attention problems
Answer: B
- A: Tempting because family history matters, but it is not the single most immediate discriminator for declaring antidepressant failure here.
- B: Correct because adequacy of dose and duration determines whether augmentation is appropriate or premature.
- C: Tempting because tolerability and adherence can depend on timing, but dose-duration adequacy is the primary unresolved rule in this stem.
- D: Tempting because ADHD history may influence future treatment, but it does not decide whether the current antidepressant failed.
1.1.1.4 Past psychiatric and medication history: choosing between true nonresponse, intolerance, and inadequate trial
A Explanation
The key decision conflict is whether a prior psychotropic exposure should push you to reuse, avoid, or reinterpret a medication. The single rule is that every prior medication exposure must be sorted into one of four buckets: effective and tolerated, effective but not tolerated, ineffective despite an adequate trial, or never adequately tested. These are not equivalent, and the exam often hinges on this distinction.
For each prior agent, collect the name, dose, route, frequency, duration, adherence, benefit, onset of benefit, adverse effects, discontinuation reason, and whether discontinuation was abrupt or planned. Ask specifically about severe reactions: dystonia, akathisia, parkinsonism, tardive symptoms, serotonin syndrome, NMS, rash, neutropenia, mania induction, severe sedation, sexual dysfunction, weight gain, or QT-related events. One prior severe reaction can eliminate an otherwise attractive option.
Past psychiatric history also includes prior hospitalization, suicide attempts, ECT, long-acting injectable use, treatment court or supervised administration, and prior periods of excellent stability. Those details guide future recommendations. A patient who did well for years on one agent but stopped because of cost or transportation is different from a patient who had no benefit after multiple adequate trials.
WHY THIS IS TESTED: many stems try to make a medication look ineffective when the actual issue is short duration, low dose, poor adherence, or intolerability that could be managed rather than a true class failure.
B Worked example
A 52-year-old man with schizophrenia, type 2 diabetes, and tobacco use disorder is admitted from an ED boarding unit. Home medications are listed as olanzapine 20 mg orally nightly, metformin 1000 mg orally twice daily, and nicotine patch 21 mg/day. A tempting wrong clue is his fasting glucose of 220 mg/dL, which may push learners away from olanzapine. His sister reports he was “doing best” on olanzapine but stopped it 3 months ago because he lost insurance and gained weight; since then he intermittently used leftover quetiapine 100 mg at bedtime. The team asks for a pharmacist recommendation on antipsychotic restart.
Reasoning chain: Identify task: choose whether prior olanzapine should be reused or rejected. Extract key facts: documented robust response on olanzapine, discontinuation due to access and metabolic burden rather than inefficacy, poor adherence after loss of insurance, partial self-treatment with subtherapeutic quetiapine. Apply rule: prior strong response is high-value evidence; if stopped for cost or adherence, consider strategies that preserve efficacy while addressing barriers. Eliminate distractors: declaring “olanzapine failure” is wrong; using the recent quetiapine exposure as evidence of antipsychotic nonresponse is wrong because the dose/pattern were inadequate; ignoring the metabolic history is also wrong because the same response must be balanced against risk. Verify: recommend restarting an antipsychotic with recognition of prior efficacy, but pair the recommendation with metabolic mitigation and access planning; if local team is considering a long-acting option, note that upcoming LAI topics build on this logic.
C Exam trap
Why it is tempting: stems often list many drugs to create an illusion of refractory illness.
Single clue that eliminates it: true resistance requires adequate prior trials; a medication stopped after 5 days for nausea or taken intermittently is not equivalent to an adequate failure.
D Checkpoint
Question: A patient reports that venlafaxine XR 75 mg orally daily “did not work,” and the prescriber asks whether this supports class failure. Which additional history best determines whether the trial was interpretable?
- Whether the patient took it with breakfast
- Whether the patient’s sibling responded to duloxetine
- Whether the patient remained on the dose long enough with consistent adherence
- Whether the patient prefers capsules to tablets
Answer: C
- A: Tempting because administration issues can affect tolerability, but the core question is adequacy of exposure.
- B: Tempting because family response can be clinically useful, but it does not validate this patient’s supposed nonresponse.
- C: Correct because duration plus adherence determine whether the reported failure can guide future class selection.
- D: Tempting because formulation preference matters for adherence, but it does not answer whether the prior trial was adequate.
- The most useful detail in a prior medication history is prior response at an adequate dose and duration.
- True or False: A drug stopped after severe akathisia should be documented as “nonresponse.”
- Name the 3 minimum details that make a prior trial interpretable: dose, duration, and ______.
1.1.1.5 Substance use, withdrawal, and medical history: when the “psychiatric” complaint is not primary psychiatric worsening
A Explanation
The decision conflict here is whether symptoms should be interpreted as primary psychiatric illness, substance-related effects, medication withdrawal, or medical contributors. The single resolving rule is to anchor the case to timing of exposure and timing of symptom onset. If the symptom started after dose change, abrupt stop, intoxication, binge, or withdrawal window, do not rush to intensify chronic psychiatric medications.
Substance history should be concrete: drug, amount, route, frequency, last use, longest abstinence, prior withdrawal, seizures, delirium, overdose, treatment history, and relapse triggers. “Social drinking” is not enough. Likewise, benzodiazepine and alcohol history are high-yield because withdrawal may present as anxiety, tremor, tachycardia, insomnia, agitation, or perceptual disturbances. Stimulant use can mimic mania or panic. Heavy cannabis use can complicate anxiety, cognition, and psychosis interpretation. Nicotine changes the history because smoking status may alter CYP1A2-substrate antipsychotic exposure after admission or cessation.
Medical history matters because thyroid disease, seizure history, eating disorders, arrhythmia risk, pregnancy, liver disease, renal disease, and sleep apnea all alter medication safety. Psychiatric pharmacists are not expected to independently diagnose the medical condition, but they are expected to recognize when that history makes a drug choice unsafe or when urgent referral is required.
WHY THIS IS TESTED: stems often tempt learners to escalate antidepressants or antipsychotics when the better answer is first to recognize withdrawal, intoxication, or a medical contraindication hidden in the history.
B Worked example
A 46-year-old man with major depressive disorder, alcohol use disorder, and hypertension presents to an outpatient behavioral health clinic for “worsening panic.” Medications are bupropion XL 300 mg orally every morning, trazodone 100 mg orally at bedtime, and lisinopril 20 mg orally daily. He reports tremor, insomnia, diaphoresis, and anxiety beginning 12 hours after his last drink; he drinks 10–12 beers nightly and had a withdrawal seizure 3 years ago. A distracting clue is that bupropion can worsen anxiety, making dose reduction seem attractive. The clinic pharmacist is asked for the most appropriate recommendation.
Reasoning chain: Identify task: determine whether this is panic worsening or substance-related danger. Extract key facts: heavy daily alcohol use, short interval since last use, autonomic symptoms, prior withdrawal seizure, bupropion on board. Apply rule: alcohol withdrawal history takes priority, and seizure risk is high; this is not a routine outpatient “panic medication adjustment” problem. Eliminate distractors: increasing trazodone or adding hydroxyzine addresses symptoms but misses the emergency risk; simply blaming bupropion is tempting but incomplete. Verify: recommend urgent evaluation/escalation for possible alcohol withdrawal and communicate that bupropion may further lower seizure threshold in this context.
C Exam trap
Why it is tempting: the patient is in a psychiatric clinic and symptoms overlap strongly with anxiety or mood disorders.
Single clue that eliminates it: the symptom cluster begins in a known withdrawal window after last use and is paired with prior severe withdrawal history.
D Checkpoint
Question: A 29-year-old patient taking fluoxetine 20 mg orally daily reports new insomnia, anxiety, and palpitations. Which psychiatric history item most helps distinguish relapse from substance-related symptoms?
- Whether the patient has ever had counseling
- Whether the patient recently changed caffeine, stimulant, alcohol, or cannabis use
- Whether the patient prefers morning appointments
- Whether the patient had childhood bedwetting
Answer: B
- A: Tempting because prior treatment engagement matters, but it does not rapidly distinguish symptom cause in this scenario.
- B: Correct because recent substance changes can produce exactly this symptom cluster and alter interpretation of antidepressant response.
- C: Tempting because scheduling can affect adherence, but it is not the discriminating history element here.
- D: Tempting only as a broad developmental history clue, but it does not answer the immediate medication question.
1.1.1.6 Family, social, trauma, and adherence history: the hidden reasons regimens fail
A Explanation
The decision conflict is whether poor outcomes reflect the wrong medication or the wrong fit for the patient’s context. The resolving rule is to identify whether access, insight, trauma triggers, caregiver support, stigma, or daily routine predict nonadherence or unsafe use. This is where many stems test advanced pharmacist thinking: not “What drug is first-line in theory?” but “What recommendation is most likely to succeed for this patient?”
Family history matters because bipolar disorder, suicide, substance use, and medication response in relatives may alter your level of caution or support a future recommendation. Social history matters because housing instability, food insecurity, transportation loss, shift work, childcare, legal stress, and language barriers can make once-daily oral therapy unrealistic. Trauma history can shape tolerability and acceptance; for example, sedation, weight changes, or sexual dysfunction may be especially unacceptable and drive silent nonadherence.
Adherence history should go beyond “Do you take your meds?” Ask how many doses were missed in the last week, how refills are obtained, whether side effects led to self-adjustment, whether the patient splits tablets, uses PRNs differently than prescribed, or stops medications when feeling better. Pharmacy claims, pill bottles, caregiver report, and previous discharge summaries often uncover discrepancies. This is where See Fig 6 becomes practical: the best medication decision may be impossible until the list is reconciled.
WHY THIS IS TESTED: board questions reward the candidate who notices that the apparently “best” drug is unrealistic because the patient cannot access it, cannot tolerate it, or will not reliably take it.
B Worked example
A 27-year-old woman with bipolar disorder, obesity, and PTSD is seen after a psychiatric hospitalization discharge. Her prescribed regimen is lamotrigine 25 mg orally daily with weekly titration, quetiapine 300 mg orally nightly, and propranolol 10 mg orally twice daily as needed for anxiety. She says quetiapine “never works” and admits she takes it only on weekends because she works early shifts and cannot tolerate morning sedation. She also missed the lamotrigine for 6 consecutive days because the pharmacy was across town. A distracting clue is a family history of “antidepressants helping everyone,” which may lure the learner toward an SSRI-based answer. The team asks what most needs to be addressed in the history before declaring the current regimen ineffective.
Reasoning chain: Identify task: interpret apparent nonresponse. Extract key facts: major adherence barriers from sedation, work schedule, and pharmacy access; interrupted lamotrigine titration; PTSD symptoms as noise. Apply rule: a regimen cannot be judged ineffective if it is not being taken as intended; social and adherence history are central, not peripheral. Eliminate distractors: family response to antidepressants does not answer the current problem; simply increasing quetiapine ignores the reason it is not taken; adding another agent compounds complexity. Verify: recommend addressing sedation-related adherence, refill access, and safe lamotrigine retitration if interruption duration requires it per product labeling/local policy confirmation.
C Exam trap
Why it is tempting: symptoms remain uncontrolled, so increasing intensity feels proactive.
Single clue that eliminates it: the patient explicitly reports not taking the medication as prescribed due to a practical barrier or intolerable adverse effect.
D Checkpoint
Question: A patient prescribed aripiprazole 10 mg orally daily after discharge says he has “failed” it because hallucinations returned. Which psychiatric history detail most changes the pharmacist recommendation?
- Whether he likes taking tablets with juice
- Whether the family history includes panic disorder
- Whether he filled the medication and has taken it consistently since discharge
- Whether he had chickenpox as a child
Answer: C
- A: Tempting because administration preferences can matter, but it does not resolve the claim of treatment failure.
- B: Tempting because family history is relevant in some cases, but it is not the key determinant of current efficacy interpretation.
- C: Correct because adherence and fill completion decide whether recurrence reflects drug failure or no effective exposure.
- D: Plausible as a background medical history item, but unrelated to the present medication question.
- True or False: A medication can be labeled ineffective even if the patient never filled it.
- The best single collateral source for recent medication possession is the ______ history.
- Name 3 social barriers that commonly masquerade as “medication failure.”
1.1.1.7 Safety history and pharmacist synthesis: what requires immediate clarification or escalation?
A Explanation
The final decision conflict is whether the history supports routine optimization or whether it contains a red flag that changes the priority to immediate clarification, withholding a recommendation, or urgent escalation. The resolving rule is to screen every history for safety-critical items before discussing fine points of efficacy.
High-priority psychiatric history items include current or recent suicidality, self-harm behavior, homicidal threats, overdose, access to lethal means, severe agitation with intoxication, recent abrupt withdrawal from alcohol or sedative-hypnotics, serotonin syndrome features after serotonergic exposure, NMS-like history after antipsychotics, clozapine-related neutropenia, severe rash with lamotrigine or carbamazepine, pregnancy considerations, and major interaction risks from current medication or substance use. In board-style practice, the pharmacist does not independently determine legal disposition, but must promptly notify the team, recommend urgent evaluation, or activate protocol when safety demands it.
History synthesis means prioritizing the one finding that changes management first. If a patient has insomnia, low mood, and missed doses, but also has escalating suicidal thoughts and stockpiled medications, the history is not “depression follow-up”; it is a safety escalation case. If a patient requests antidepressant restart but reports prior SSRI-induced mania, that single clue outranks routine depression treatment logic. If a patient has psychotic relapse and stopped smoking on admission, antipsychotic concentration changes may matter, but safety still starts with risk assessment and medication reconciliation. See Fig 5 for the sequence.
WHY THIS IS TESTED: the exam often measures whether you can shift from optimization thinking to urgent safety thinking based on one history red flag.
B Worked example
A 38-year-old man with depression, chronic pain, and insomnia presents for refill review. Current medications are duloxetine 60 mg orally daily, trazodone 150 mg orally nightly, gabapentin 600 mg orally three times daily, and tramadol 50 mg orally every 6 hours as needed from another prescriber. He reports worsening mood and requests a higher duloxetine dose. A distracting clue is neuropathic pain, which could support escalation. However, he also reveals that he stopped all medications for 5 days last month “to save them,” resumed them all at once, has had passive death wishes, and recently stockpiled unused tablets after a breakup.
Reasoning chain: Identify task: determine whether this is routine antidepressant adjustment. Extract key facts: suicidality-related warning, medication stockpiling, variable adherence, serotonergic/polypharmacy exposure. Apply rule: safety red flags override routine dose optimization; pharmacist role is to urgently notify the team and clarify overdose risk, not simply recommend a dose increase. Eliminate distractors: increasing duloxetine for pain is superficially attractive; focusing only on adherence counseling misses acute risk; dismissing the stockpile because thoughts are “passive” is unsafe. Verify: escalate promptly, communicate overdose and serotonergic risk, and recommend immediate prescriber/team review.
C Exam trap
Why it is tempting: the stem begins like a standard antidepressant follow-up and includes a medication-based rationale for adjustment.
Single clue that eliminates it: any active safety signal such as suicidality with stockpiled medication, recent overdose, or severe withdrawal history changes the task from optimization to escalation.
D Checkpoint
Question: Which psychiatric history finding most requires immediate clarification before recommending a routine antidepressant increase?
- Family history of seasonal depression
- Past benefit from cognitive behavioral therapy
- Recent medication stockpiling with escalating suicidal thoughts
- Preference for bedtime dosing
Answer: C
- A: Tempting because family history can shape formulation of the case, but it is not the urgent deciding clue.
- B: Tempting because prior benefit informs comprehensive care, but it does not outrank an immediate safety issue.
- C: Correct because stockpiling plus suicidal thoughts creates acute overdose concern and requires urgent team communication before routine adjustment.
- D: Tempting because dosing preference may improve adherence, but it is irrelevant compared with imminent safety risk.
Exam Traps & Differentiators
Most common wrong answer and why: Calling a regimen “ineffective” without proving adequate exposure. This is tempting because stems often list persistent symptoms and multiple prior medications. The differentiator is whether the patient actually took a therapeutic dose for long enough, without confounding discontinuation or substance-related symptoms.
| Looks similar | Actually is | Single discriminator | Medication implication |
|---|---|---|---|
| Relapse of anxiety/depression | SSRI discontinuation | Symptoms begin soon after abrupt stop or missed doses | Do not declare current replacement ineffective too early |
| Antidepressant nonresponse | Inadequate trial | Low dose, short duration, or poor adherence | Clarify before augmenting or switching |
| Panic worsening | Alcohol or sedative withdrawal | Last use timing plus autonomic symptoms or seizure history | Urgent evaluation may be needed |
| Psychosis despite treatment | No medication access after discharge | Refill gap or never-filled prescription | Address transitions-of-care barrier before changing class |
| Routine depression follow-up | Acute safety escalation | Suicidal thoughts with stockpiled medication or recent overdose | Urgent team notification before routine optimization |
| If the stem says... | Think... |
|---|---|
| “Several antidepressants failed” | Were they adequate trials, and were they actually taken? |
| “Anxiety worsened after medication change” | Withdrawal or activation timeline before assuming disease progression |
| “Psychosis recurred after discharge” | Medication reconciliation, fill history, and adherence barriers |
| “Patient wants a higher dose today” | Safety screen first: suicidality, overdose, substance withdrawal, serious reactions |
| “No side effects reported” | Patients may have self-discontinued; ask directly about sedation, weight, sexual dysfunction, EPS, and stigma |
| “Family member says they did better before” | Collateral may reveal the most effective prior regimen and the real reason it was stopped |
Related future trap: in Mental Status Exam Findings, learners often confuse a historical report of hallucinations with current active perceptual disturbance. History tells you what has happened over time; MSE tells you what is present now. Related future trap in Screening And Monitoring Scales: symptom severity scores do not replace a good medication and safety history.
Tables
| History element | What to ask | Why it matters for medication decisions |
|---|---|---|
| Current symptom timeline | When did symptoms start and what changed first? | Distinguishes relapse from withdrawal, activation, or intoxication |
| Past medication trials | Drug, dose, duration, adherence, benefit, adverse effects | Determines true nonresponse versus inadequate trial |
| Prior serious reactions | Rash, NMS, serotonin syndrome, severe EPS, neutropenia | May eliminate re-exposure or require urgent clarification |
| Substance use | Type, amount, route, last use, withdrawal history | Explains symptoms and modifies safety planning |
| Medical comorbidities | Seizures, arrhythmia risk, renal/hepatic disease, pregnancy | Changes drug selection, interactions, and monitoring |
| Adherence/access | Missed doses, refill gaps, cost, transportation, side-effect burden | Prevents false labeling of medication failure |
| Family history | Bipolar disorder, suicide, substance use, strong medication response | Supports risk assessment and treatment interpretation |
| Safety history | Suicidality, self-harm, overdose, stockpiling, lethal means | May require immediate team notification or emergency referral |
| Comparison point | True medication failure | Intolerance | Inadequate trial/nonadherence |
|---|---|---|---|
| Dose | Therapeutic | May be therapeutic or low | Often subtherapeutic or inconsistent |
| Duration | Adequate | May stop early due to side effects | Often too short to judge |
| Adherence | Consistent | Usually consistent until adverse effect | Interrupted, missed, or never filled |
| Outcome statement | No meaningful benefit despite adequate exposure | Benefit limited by unacceptable harm | Outcome uninterpretable |
| Exam action | Consider switch or augmentation | Consider mitigation or alternative | Clarify before changing strategy |
| Differential history pattern | Key clue | Likely interpretation | Pharmacist-facing next step |
|---|---|---|---|
| Anxiety after stopping paroxetine | Abrupt cessation and rapid onset | Antidepressant discontinuation | Clarify stop history before labeling the new drug ineffective |
| Agitation after antipsychotic increase | Recent dose increase, inner restlessness | Akathisia possibility | Assess adverse effect rather than assuming worsening psychosis |
| Tremor, diaphoresis, insomnia after last drink | Withdrawal window and prior seizure | Alcohol withdrawal | Urgent escalation and medication-risk review |
| Relapse after discharge | Prescription never picked up | No effective maintenance exposure | Address access and reconciliation first |
| Request for routine refill change | Medication stockpiling plus suicidal ideation | Acute safety concern | Notify team immediately before routine optimization |
Algorithm / Approach
Exam takeaway: Convert each history clue into one of four actions—optimize, clarify, monitor, or escalate.
flowchart TD
A[History clue identified] --> B{Safety red flag?}
B -- Yes --> C[Escalate urgently]
B -- No --> D{Adequate prior trial?}
D -- No --> E[Clarify before switching]
D -- Yes --> F{Helpful but intolerable?}
F -- Yes --> G[Mitigate or choose alternative]
F -- No --> H{Adherence/access barrier?}
H -- Yes --> I[Fix implementation plan]
H -- No --> J[Optimize regimen] Rapid Review
- Prior trial quality → dose + duration + adherence separate true failure from noise
- Symptoms after abrupt SSRI stop → think discontinuation before relapse
- “Panic” after last drink → withdrawal timing outranks routine anxiolytic adjustment
- Past benefit on one antipsychotic → stopped-for-cost differs from stopped-for-nonresponse
- Family bipolar history → increases caution with unopposed antidepressant interpretation
- Medication list disagreement → patient report plus fill history beats chart list alone
- Return of symptoms after discharge → first ask whether the prescription was filled
- Severe prior reaction → avoid casual rechallenge until exact event clarified
- Stockpiling medication → safety escalation, not routine dose titration
- Side-effect-driven missed doses → implementation failure, not necessarily class failure
- Substance use history → quantity, last use, and withdrawal history beat vague labels
- Social barriers → regimen fit can matter more than theoretical first-line status
- Collateral from family/caregiver → often reveals actual adherence and prior stability pattern
Self-check quiz
1. A 33-year-old man with major depressive disorder and GERD is taking escitalopram 10 mg orally daily for 12 days and omeprazole 20 mg orally daily. The prescriber asks whether to add augmentation because the patient reports no improvement yet. Which history detail is most appropriate to clarify first?
- Whether the escitalopram trial has reached an adequate duration with consistent adherence
- Whether the patient prefers capsules over tablets
- Whether the patient’s cousin responded to sertraline
- Whether the patient drinks tea in the evening
2. A 40-year-old woman with panic symptoms and chronic insomnia takes paroxetine 40 mg orally daily but stopped it abruptly 4 days ago after running out. She now reports dizziness, anxiety, and “electric shock” sensations. Which history interpretation is most appropriate?
- Probable immediate antidepressant class failure
- Probable discontinuation symptoms after abrupt SSRI cessation
- Proof that she requires an antipsychotic
- Evidence that paroxetine caused treatment-resistant panic disorder
3. A 51-year-old man with schizophrenia, obesity, and type 2 diabetes is prescribed olanzapine 15 mg orally nightly after an inpatient stay. At follow-up, he reports worsening hallucinations. Fill records show the prescription was never picked up because of cost, and he has been taking leftover risperidone 1 mg orally at bedtime every few days. What is the most appropriate pharmacist interpretation?
- Olanzapine failed despite an adequate trial and should be avoided
- The recurrence most likely reflects nonadherence and access barriers rather than true olanzapine failure
- Risperidone 1 mg every few days proves antipsychotic class resistance
- The main issue is that bedtime dosing is always ineffective for psychosis
4. A 45-year-old woman with depression, alcohol use disorder, and hypertension takes bupropion XL 300 mg orally every morning and trazodone 100 mg orally nightly. She presents to clinic with tremor, diaphoresis, insomnia, and anxiety 10 hours after her last alcohol intake. She had a prior alcohol-withdrawal seizure. Which recommendation is most appropriate?
- Increase bupropion XL to 450 mg orally every morning for worsening mood
- Recommend urgent medical evaluation for possible alcohol withdrawal and communicate seizure risk
- Continue current medications and reassess in 4 weeks because symptoms may be anxiety relapse
- Increase trazodone to 200 mg orally nightly as the best initial step
5. A 28-year-old woman with bipolar disorder and PTSD takes quetiapine 300 mg orally nightly and lamotrigine 50 mg orally daily. She reports persistent symptoms and says quetiapine “does nothing,” but then states she takes it only on weekends due to sedation before early work shifts. Which is the most appropriate pharmacist conclusion?
- Quetiapine is ineffective and should be replaced immediately
- The symptom persistence cannot be interpreted as drug failure until adherence and regimen fit are addressed
- PTSD always explains nonresponse to bipolar medications
- Lamotrigine should be doubled first because it has fewer sedative effects
6. A 37-year-old man with major depressive disorder, neuropathic pain, and insomnia takes duloxetine 60 mg orally daily, trazodone 150 mg orally nightly, gabapentin 600 mg orally three times daily, and tramadol 50 mg orally every 6 hours as needed. He requests a duloxetine increase because his mood is worse. During review, he reports passive death wishes and says he has stockpiled extra tablets after missed refill pickups. Which is the most appropriate next step for the pharmacist?
- Recommend increasing duloxetine to 90 mg orally daily because pain and mood both remain uncontrolled
- Recommend urgent team notification and safety evaluation before routine antidepressant adjustment
- Recommend stopping trazodone only because it may contribute to oversedation
- Recommend outpatient follow-up in 1 month because passive thoughts alone are low risk
7. A 32-year-old woman with depression and obesity is taking sertraline 50 mg orally daily for 3 weeks after abruptly stopping paroxetine 40 mg orally daily when she ran out. She reports anxiety, nausea, insomnia, and feeling “wired.” She also drinks three energy drinks daily and takes ondansetron 4 mg orally as needed for migraine-associated nausea. Which interpretation is most appropriate?
- This proves sertraline nonresponse, so immediate augmentation is required
- The symptoms are most consistent with a history that requires clarification for discontinuation and activation before labeling treatment failure
- The only important clue is ondansetron use, so the syndrome should be treated as serotonin syndrome
- The energy drinks fully explain the case, so the antidepressant timeline can be ignored
8. A 60-year-old man with schizoaffective disorder, CKD stage 3, and tobacco use disorder was stable for years on clozapine per family report but presents after 2 months off medications when his pharmacy closed. Current chart allergies list “antipsychotics—bad reaction,” but no details are available. He now takes no psychotropics, smokes one pack per day, and has recurrent psychosis. Which history element most requires clarification before any specific antipsychotic recommendation is finalized?
- The exact nature of the prior “bad reaction,” including whether it represented a serious reaction versus nonspecific intolerance
- Whether he prefers blister packs to bottles
- Whether his cousin had depression
- Whether he drinks coffee after dinner
Answer key
1.1.1.8 1. Question 1
Correct answer: A
- A: Tempting because it may feel too basic, but it is correct: escitalopram 10 mg daily for 12 days is usually too early to label ineffective, and adherence must be confirmed before augmentation. The discriminating clue is the short treatment duration. Authoritative support: Lexicomp SSRI monographs; DiPiro Pharmacotherapy principles of antidepressant trial assessment.
- B: Tempting because formulation preference can influence adherence, but the single fact that eliminates it is that no adequate trial has yet occurred. Source support: antidepressant evaluation principles in AHFS and standard psychopharmacology texts.
- C: Tempting because family response can inform future selection, but it does not answer whether this patient’s current trial is interpretable. The discriminating clue is the patient’s own early course on therapy. Source: DiPiro; Clinical Pharmacology drug class guidance.
- D: Tempting because caffeine or tea can worsen insomnia or anxiety, but evening tea does not supersede the need to verify adequate duration and adherence. The discriminating clue is the 12-day escitalopram exposure. Source: Lexicomp and antidepressant monitoring guidance.
1.1.1.9 2. Question 2
Correct answer: B
- A: Tempting because symptoms returned after the medication was stopped, but abrupt cessation with dizziness and “electric shocks” points to discontinuation rather than class failure. The discriminating clue is the abrupt stop 4 days ago. Source: Lexicomp paroxetine monograph; FDA labeling and psychopharmacology references on SSRI discontinuation.
- B: Correct because paroxetine has a high discontinuation-risk profile, and the symptom cluster plus timing strongly supports discontinuation syndrome. The discriminating clue is the rapid onset after running out. Source: Lexicomp; AHFS Drug Information.
- C: Tempting because severe distress can push learners toward “stronger” therapy, but no psychosis clue is provided. The discriminating clue is the classic sensory symptom description. Source: standard antidepressant discontinuation references.
- D: Tempting because panic symptoms are present, but the single fact that eliminates it is that symptoms track abrupt drug cessation, not adequate exposure failure. Source: DiPiro and antidepressant practice references.
1.1.1.10 3. Question 3
Correct answer: B
- A: Tempting because hallucinations persist and olanzapine carries metabolic burden, but the drug was never picked up, so no adequate trial occurred. The discriminating clue is the fill record showing zero possession. Source: Lexicomp olanzapine monograph; ASHP medication reconciliation principles.
- B: Correct because the recurrence is best explained by access-related nonadherence and inconsistent subtherapeutic leftover use. The discriminating clue is the never-filled discharge prescription. Source: ASHP transitions-of-care guidance; DiPiro adherence principles.
- C: Tempting because another antipsychotic was used and symptoms persisted, but risperidone 1 mg every few days is not an interpretable antipsychotic trial. The discriminating clue is the clearly inadequate dose pattern. Source: Lexicomp risperidone monograph.
- D: Tempting only if a learner overfocuses on administration timing; bedtime dosing is common and does not explain the failure here. The discriminating clue remains the prescription nonfill. Source: standard antipsychotic dosing references.
1.1.1.11 4. Question 4
Correct answer: B
- A: Tempting because depression is present and bupropion is already in use, but the single fact that eliminates it is suspected alcohol withdrawal with prior seizure history; also, bupropion may worsen seizure risk. Source: FDA bupropion labeling; Lexicomp.
- B: Correct because tremor, diaphoresis, insomnia, and anxiety soon after last drink with prior withdrawal seizure indicate urgent risk. The discriminating clue is the prior alcohol-withdrawal seizure. Source: ASAM alcohol withdrawal guidance; Lexicomp bupropion safety information.
- C: Tempting because anxiety relapse is plausible, but the timing after last alcohol use and seizure history make watchful waiting unsafe. Source: ASAM guidance and withdrawal references.
- D: Tempting because trazodone may help insomnia, but it does not address the acute withdrawal syndrome or seizure risk. The discriminating clue is the withdrawal window with autonomic symptoms. Source: alcohol withdrawal guidelines.
1.1.1.12 5. Question 5
Correct answer: B
- A: Tempting because symptoms persist and quetiapine can be sedating, but the drug’s efficacy cannot be judged when it is taken only on weekends. The discriminating clue is inconsistent administration due to sedation and schedule mismatch. Source: Lexicomp quetiapine monograph; adherence principles in psychopharmacology texts.
- B: Correct because the regimen has not been implemented as prescribed, so the right move is to address adherence and fit before declaring failure. The discriminating clue is weekend-only use. Source: DiPiro; ASHP transitions-of-care and adherence guidance.
- C: Tempting because comorbidity can complicate symptom interpretation, but PTSD does not explain away the adherence problem. The discriminating clue is the self-reported nonadherence reason. Source: psychopharmacology treatment-interpretation principles.
- D: Tempting because lamotrigine is less sedating, but doubling it first ignores the primary reason symptoms remain uncontrolled and could create unsafe titration issues depending on interruption history. Source: FDA lamotrigine labeling; Lexicomp.
1.1.1.13 6. Question 6
Correct answer: B
- A: Tempting because duloxetine could reasonably be increased for pain and mood in some patients, but the single fact that eliminates it is passive death wishes plus stockpiled medication, which raises overdose concern. Source: FDA duloxetine labeling; suicide-risk management principles in psychiatric pharmacy references.
- B: Correct because safety red flags override routine antidepressant optimization; pharmacist action is urgent notification and evaluation. The discriminating clue is stockpiling combined with suicidal ideation. Source: APA-related suicide risk principles; ASHP patient safety guidance; Lexicomp interaction/safety monographs.
- C: Tempting because trazodone contributes to polypharmacy and sedation, but focusing narrowly on one drug misses the immediate self-harm risk. The discriminating clue is the safety history, not just polypharmacy. Source: Lexicomp and clinical safety guidance.
- D: Tempting because “passive” may sound less urgent, but medication stockpiling makes delayed follow-up unsafe. The discriminating clue is preparation/access to means. Source: suicide-risk assessment standards and psychiatric pharmacy safety practice.
1.1.1.14 7. Question 7
Correct answer: B
- A: Tempting because symptoms continue despite 3 weeks of sertraline, but the single fact that eliminates it is abrupt paroxetine discontinuation just before the switch, making discontinuation and early activation plausible. Source: Lexicomp sertraline and paroxetine monographs.
- B: Correct because the history contains multiple confounders—abrupt SSRI stop, early new-trial timing, and stimulant intake—so treatment failure cannot yet be declared. The discriminating clue is the medication transition timeline. Source: AHFS and standard antidepressant switching guidance.
- C: Tempting because ondansetron and serotonergic agents may trigger concern, but classic serotonin syndrome features are not provided, and the history fits a more common alternative. The discriminating clue is the abrupt paroxetine cessation with discontinuation-type symptoms. Source: FDA labeling and serotonin syndrome references.
- D: Tempting because three energy drinks daily can worsen anxiety and insomnia, but saying they “fully explain” the case ignores the more important SSRI transition history. The discriminating clue is the temporal relationship to stopping paroxetine. Source: psychopharmacology transition principles.
1.1.1.15 8. Question 8
Correct answer: A
- A: Correct because “bad reaction” is too vague to support safe antipsychotic selection; the difference between severe EPS, NMS, neutropenia, sedation, or “felt bad” radically changes the recommendation. The discriminating clue is the undocumented allergy label paired with a strong family report of prior stability on clozapine. Source: FDA clozapine labeling; Lexicomp antipsychotic safety monographs.
- B: Tempting because packaging may improve adherence, especially in a patient with pharmacy disruption, but it does not resolve whether a class-limiting serious reaction occurred. Source: adherence literature and ASHP transitions guidance.
- C: Tempting only as broad family context, but it does not affect immediate antipsychotic safety selection. The discriminating clue is the antipsychotic reaction history. Source: psychopharmacology safety principles.
- D: Tempting because caffeine can affect sleep and anxiety, but it does not outrank the need to clarify a potentially dangerous prior reaction. The discriminating clue is the vague allergy documentation. Source: Lexicomp and product labeling.