Why it matters
- Step 3 repeatedly tests whether you act on airway, breathing, circulation, and hypoperfusion before you chase a diagnosis.
- In real practice and on the exam, one missed shock state can turn a stable-appearing stem into a mortality question within minutes.
- Many wrong answers are technically reasonable tests or treatments, but they are unsafe because they come before stabilization.
- The same framework drives ED questions, inpatient deterioration, perioperative instability, pediatric dehydration, obstetric hemorrhage, and CCS orders.
Key Terms & Must-Know Facts
1.1.1.1 Key terms
- Airway compromise: inability to protect or maintain a patent airway
- Respiratory failure: inadequate oxygenation and/or ventilation
- Shock: circulatory failure causing inadequate tissue perfusion
- Hypoperfusion: reduced end-organ blood flow
- MAP: mean arterial pressure; practical perfusion target often \( \geq 65 \) mm Hg in many shock states
- Lactate: marker of anaerobic metabolism and global hypoperfusion
- Hypovolemic shock: low preload from volume loss
- Cardiogenic shock: pump failure with low forward flow
- Distributive shock: pathologic vasodilation, often septic or anaphylactic
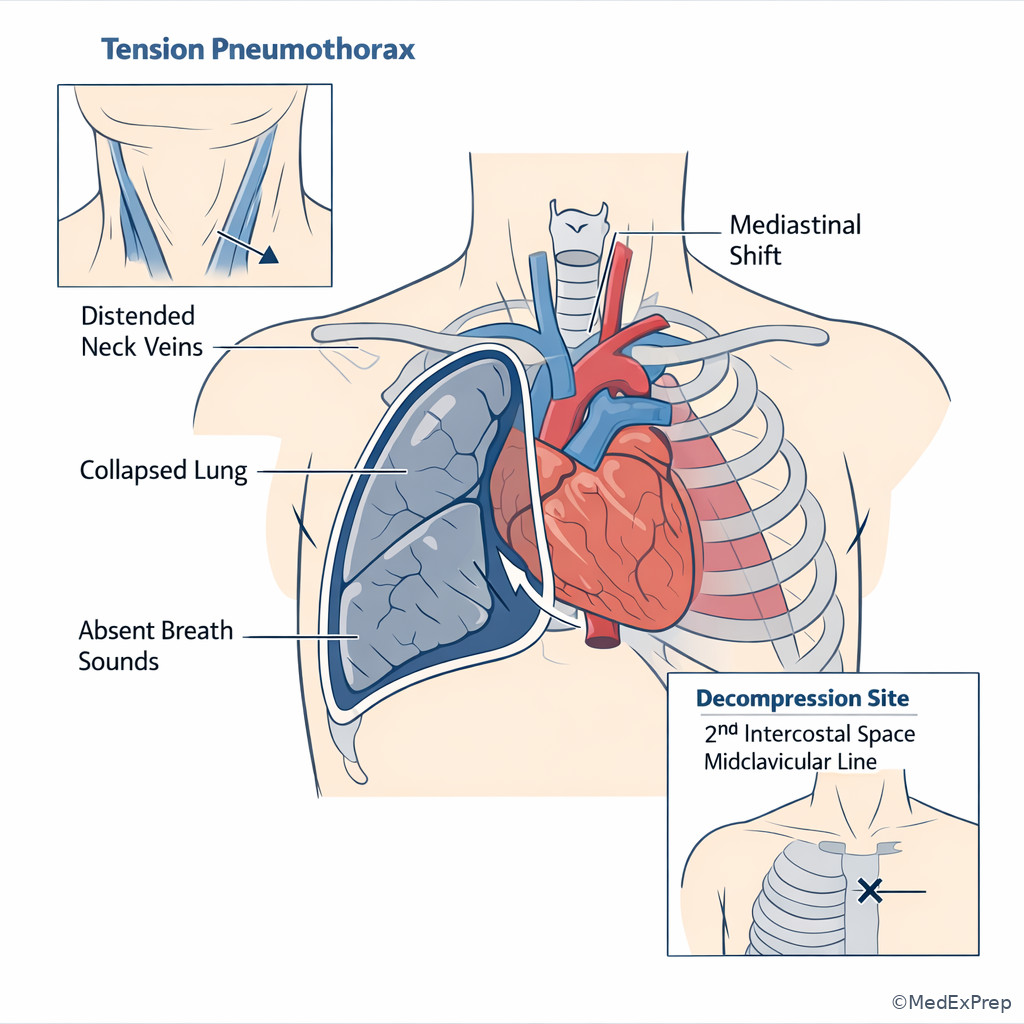
- Obstructive shock: impaired filling or outflow, such as tamponade, tension pneumothorax, massive PE
- Pressor: vasopressor used when fluids alone do not restore perfusion
- Source control: removing or controlling the cause, such as drainage, surgery, or treating infection
1.1.1.2 Must-know facts
- Unstable airway or impending respiratory arrest outranks all diagnostic testing.
- Hypotension is not required for shock; altered mental status, cool extremities, oliguria, or elevated lactate may be earlier clues.
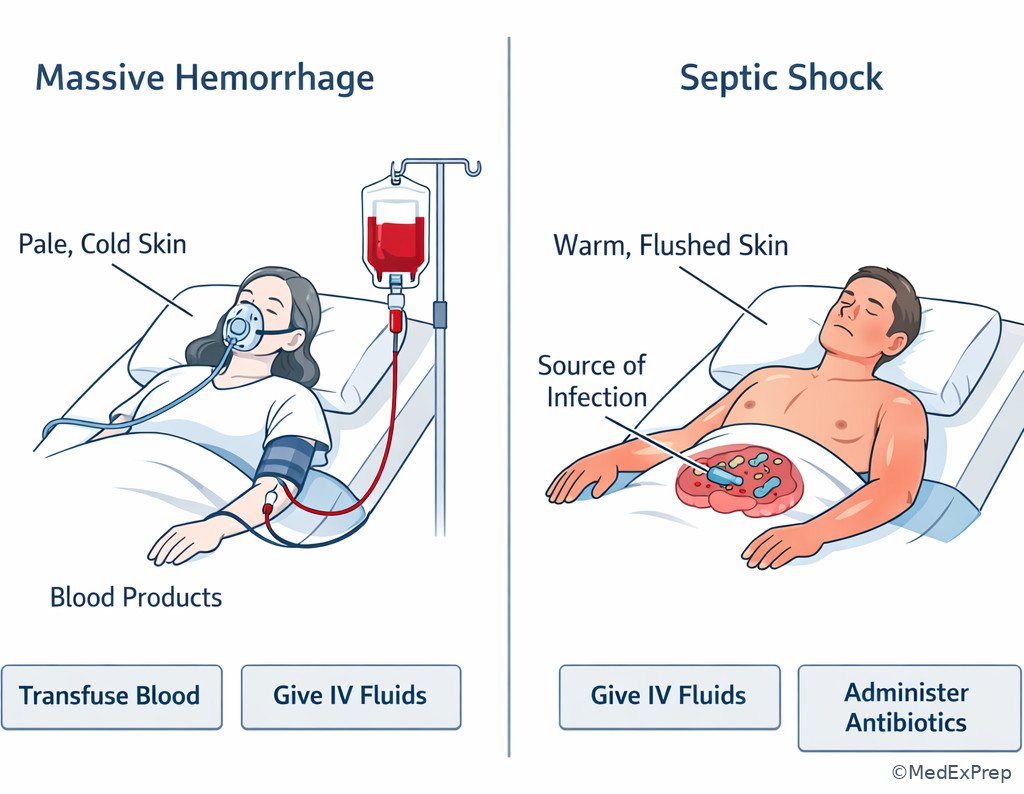
- Warm extremities with low SVR suggest distributive shock; cold clammy skin suggests low cardiac output or hypovolemia.
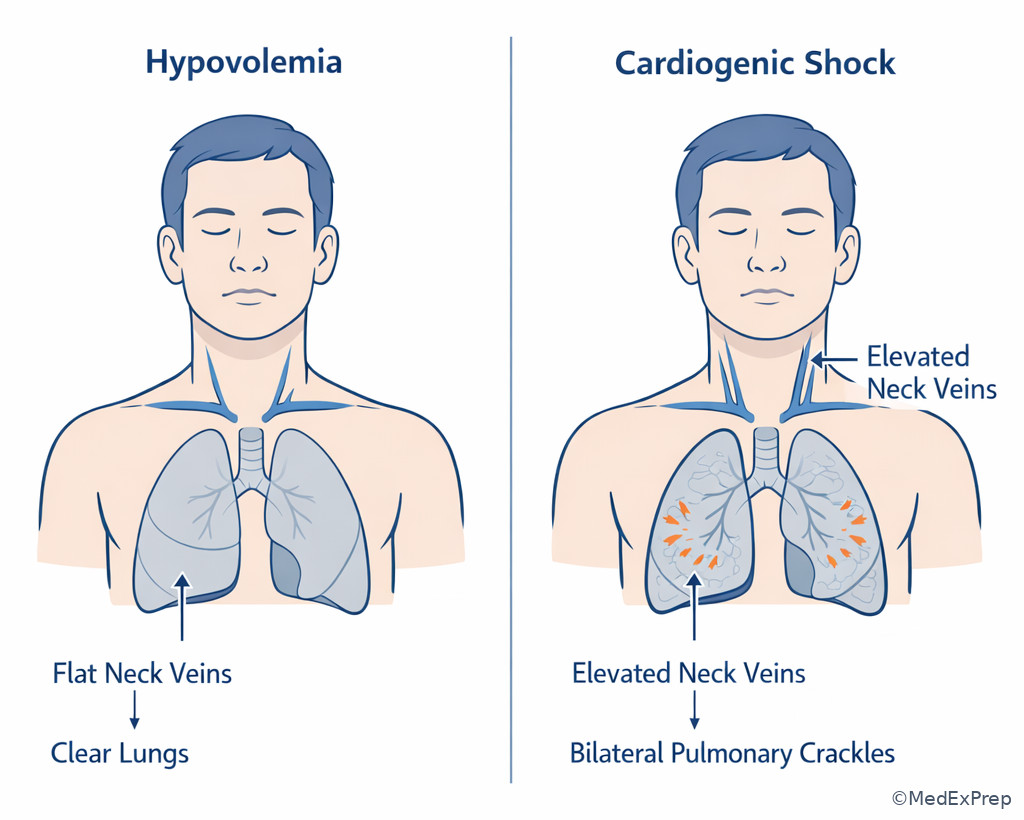
- Flat neck veins favor hypovolemia; elevated JVP favors cardiogenic or obstructive shock.
- Massive hemorrhage requires blood products, not just crystalloid.
- Tension pneumothorax is treated immediately with decompression; do not wait for imaging.
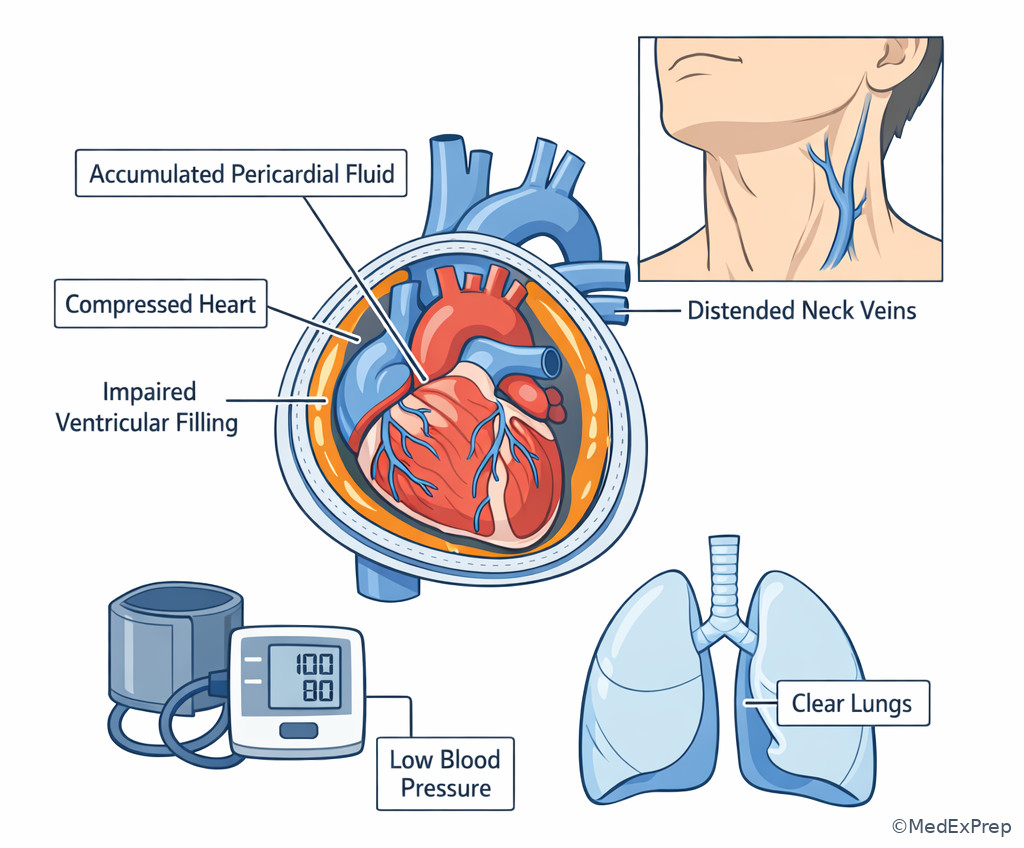
- Cardiac tamponade causes obstructive shock and needs urgent pericardial drainage after stabilization.
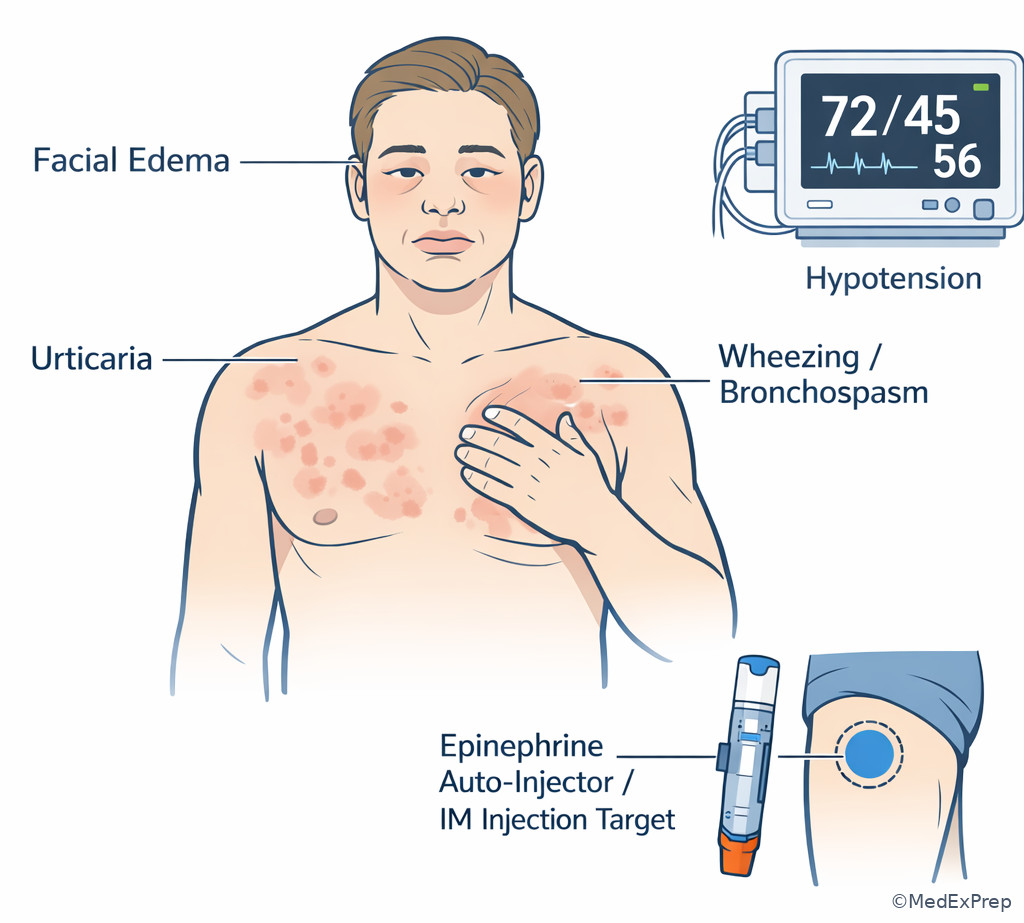
- Anaphylaxis requires IM epinephrine first, even if wheezing might tempt bronchodilator-only treatment.
- Cardiogenic shock often worsens with large indiscriminate fluid boluses.
- Response to initial therapy is part of diagnosis: reassessment is a tested skill, not an afterthought.
Exam takeaway: Use the ABC sequence to decide what must be treated before any confirmatory testing.
flowchart TD
A[Unstable patient] --> B{Airway protected?}
B -- No --> C[Intubate or open airway now]
B -- Yes --> D{Breathing adequate?}
D -- No --> E[Oxygen ventilation decompression if needed]
D -- Yes --> F{Perfusion adequate?}
F -- No --> G[IV IO access fluids blood pressor based on cause]
F -- Yes --> H[Focused workup and disposition] See Fig 1 for the core sequencing rule that prevents the most common Step 3 error: choosing the right diagnosis but in the wrong order.
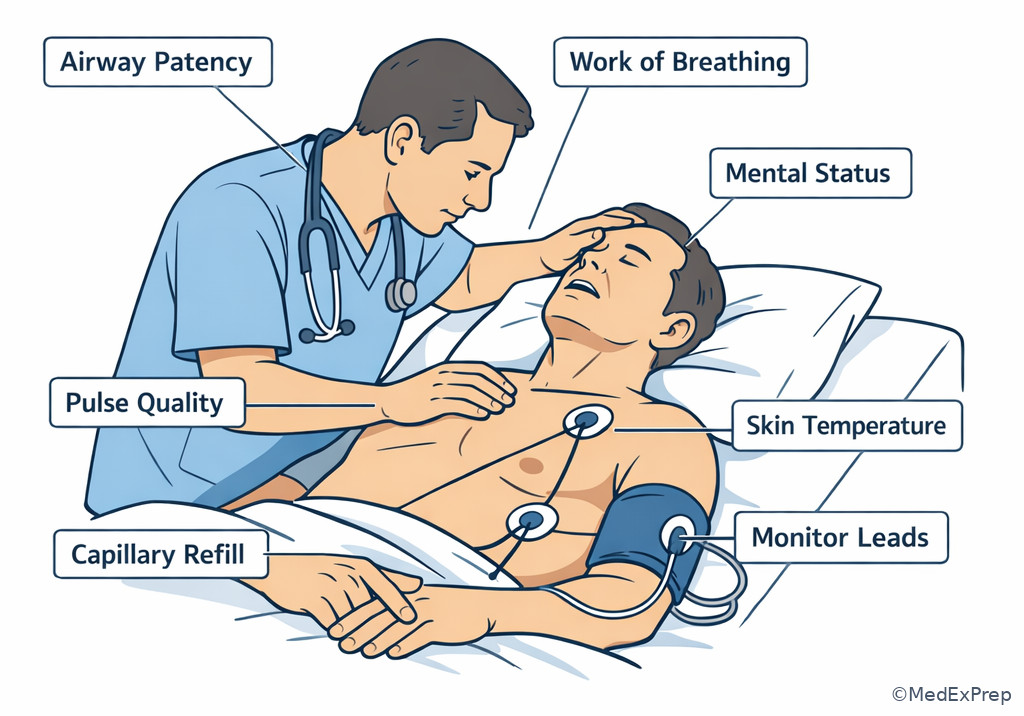
Exam takeaway: Visually anchor the first-minute survey of airway, breathing pattern, mental status, pulses, and skin perfusion.
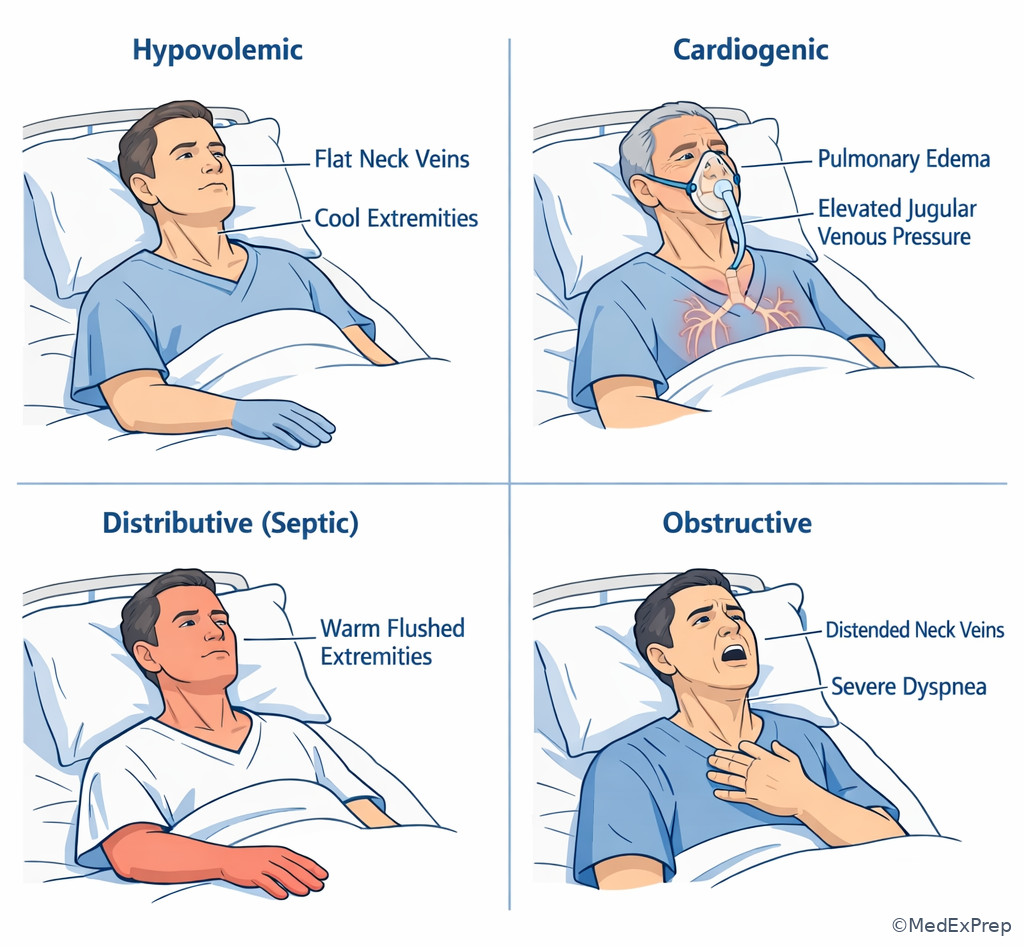
Exam takeaway: Skin temperature, neck veins, and lung findings help separate shock categories before invasive data are available.
Core content
1.1.1.3 Foundational approach: ABCs before diagnosis
A Explanation
The decision conflict is simple but heavily tested: do you continue evaluating the cause, or do you first stabilize the failing system? The resolving rule is that threatened airway, inadequate breathing, or shock always come before diagnostic completeness. On Step 3, the trap is often a beautiful diagnosis hidden inside an unstable patient. If the patient cannot speak, is tiring out, has stridor, severe hypoxemia, agonal breathing, or rapidly worsening mental status, the correct move is airway and ventilatory support now. If airway and breathing are adequate but perfusion is failing, circulation becomes the priority: IV/IO access, monitors, bedside glucose when altered, targeted fluids or blood, and cause-specific intervention.
WHY THIS IS TESTED: the exam wants to know whether you can reject a tempting but delayed answer such as CT, troponin, antibiotics, or echocardiography when the patient first needs oxygenation, decompression, transfusion, or vasopressor support. The board style is “best next step,” not “best complete plan.” Choose what changes mortality in the next minute.
Use first-look clues fast: inability to phonate or handle secretions points to airway danger; cyanosis, severe work of breathing, or absent breath sounds point to breathing failure; weak pulses, cool clammy skin, altered mentation, oliguria, narrow pulse pressure, or rising lactate point to circulatory shock. If a patient is peri-arrest, perform resuscitation while gathering history. Pulse oximetry, cardiac monitoring, ECG, bedside ultrasound, and initial labs support—not replace—the first intervention.
B Worked example
A 67-year-old man is brought to the ED for confusion and shortness of breath. He has COPD, type 2 diabetes, and prior stroke. He was seen earlier for fever and cough and has not taken his metformin today. Temperature is 38.8°C, BP 78/46 mm Hg, HR 128/min, RR 34/min, oxygen saturation 84% on room air. He answers only one-word questions and has diffuse crackles. Lactate is 5.1 mmol/L; troponin is mildly elevated. The team asks for the most appropriate next step.
Reasoning chain: Identify the task: this is a best-next-step stabilization question. Extract key facts: hypotension, hypoxemia, tachypnea, altered mental status, likely infection, elevated lactate. The tempting clue is the troponin, which could pull you toward ACS workup. Apply the rule: unstable ABCs first. He needs oxygen and likely ventilatory support while circulation is addressed with immediate resuscitative measures. Eliminate distractors: CT chest does not come first; serial troponins do not come first; a full pneumonia workup without stabilization is unsafe. Verify: after oxygenation and circulation support begin, cultures, antibiotics, imaging, and further differentiation follow.
C Exam trap
D Checkpoint
Question: A 54-year-old woman with metastatic breast cancer, chronic opioid use, and hypertension presents with progressive somnolence. She is breathing 6/min, oxygen saturation is 79%, pupils are pinpoint, and BP is 92/58 mm Hg. Which is the most appropriate next step?
- Administer naloxone and support ventilation — tempting because opioid toxicity is strongly suggested, and it is right because hypoventilation is the immediate life threat and this intervention addresses breathing first.
- Obtain arterial blood gas — tempting because it quantifies respiratory failure, but it is wrong because the patient is already clinically in ventilatory failure and needs treatment before confirmation.
- Order CT head — tempting because altered mental status could reflect intracranial pathology in a cancer patient, but it is wrong because respiratory depression is more immediately lethal and more directly supported by the stem.
- Give IV normal saline bolus only — tempting because she is hypotensive, but it is wrong because circulation support alone does not correct the primary breathing failure.
Answer: A
1.1.1.4 Foundational classification: identifying the shock category fast
A Explanation
The decision conflict here is whether hypotension should be treated generically or by matching bedside findings to a shock phenotype. The resolving rule is that skin temperature, jugular venous pressure, lung exam, and likely trigger usually classify shock before invasive monitoring. Hypovolemic shock comes from fluid or blood loss: low preload, flat neck veins, cool extremities, tachycardia, and often clear lungs unless there is concurrent disease. Cardiogenic shock is pump failure: low output with elevated filling pressures, pulmonary edema, cool clammy skin, elevated JVP, and often chest pain or new ischemia. Distributive shock, especially septic shock, features vasodilation and relative maldistribution: warm flushed skin early, wide pulse pressure, low SVR, and infection or anaphylaxis clues. Obstructive shock is mechanical blockage to filling or output: think tension pneumothorax, cardiac tamponade, or massive PE, often with elevated JVP and dramatic respiratory or hemodynamic findings.
WHY THIS IS TESTED: Step 3 wants you to choose which immediate therapy fits the physiology. A large fluid bolus may help hypovolemic or some distributive shock, but it can worsen cardiogenic pulmonary edema. Needle decompression fixes tension pneumothorax, not pressors alone. Blood products fix hemorrhagic shock more effectively than liters of crystalloid.
Use pattern recognition, not memorized lists alone. Cool + flat neck veins = low volume until proven otherwise. Cool + wet lungs + elevated JVP = pump failure. Warm + infected or allergic picture = distributive. Elevated JVP + unilateral absent breath sounds or muffled heart sounds or sudden right-heart strain = obstructive. See Fig 2 for a comparison pathway that compresses this bedside differentiation.
Exam takeaway: Neck veins, lung findings, skin temperature, and trigger usually identify the shock type before advanced testing.
flowchart TD
A[Hypotension or hypoperfusion] --> B{JVP elevated?}
B -- No --> C[Think hypovolemic]
B -- Yes --> D{Breath sounds absent on one side?}
D -- Yes --> E[Obstructive: tension pneumothorax]
D -- No --> F{Pulmonary edema crackles?}
F -- Yes --> G[Cardiogenic shock]
F -- No --> H{Warm flushed skin or infection/allergy clues?}
H -- Yes --> I[Distributive shock]
H -- No --> J[Consider tamponade or massive PE] B Worked example
A 72-year-old woman presents two days after an anterior MI with dizziness and dyspnea. She has chronic kidney disease, diabetes, and heart failure with reduced ejection fraction. BP is 82/54 mm Hg, HR 118/min, RR 28/min, oxygen saturation 90% on 4 L nasal cannula. She is cool and diaphoretic, has elevated JVP, diffuse crackles, and urine output has dropped. A resident suggests a 2-L crystalloid bolus because she is hypotensive.
Reasoning chain: Identify task: choose the shock category and best immediate support. Extract key facts: recent MI, cool extremities, elevated JVP, pulmonary edema, oliguria. The distracting detail is CKD, which can coexist with volume overload and might confuse urine output interpretation. Apply the rule: this is cardiogenic shock, not hypovolemic shock. Eliminate the fluid bolus because lungs are wet and filling pressures are high. Verify: the safer next step is hemodynamic support with vasopressor/inotrope strategy, urgent reperfusion evaluation if indicated, and ICU-level care.
C Exam trap
D Checkpoint
Question: A 35-year-old man develops sudden dyspnea and hypotension after subclavian central line placement. BP is 76/44 mm Hg, HR 132/min, oxygen saturation 82%, neck veins are distended, and right breath sounds are absent. Which shock category best explains this presentation?
- Hypovolemic shock — tempting because hypotension and tachycardia fit, but it is wrong because distended neck veins and unilateral absent breath sounds argue against low preload from volume loss.
- Cardiogenic shock — tempting because JVP is elevated, but it is wrong because the immediate trigger after line placement plus unilateral absent breath sounds favors mechanical obstruction rather than pump failure.
- Distributive shock — tempting because procedures can trigger reactions, but it is wrong because absent unilateral breath sounds point to tension pneumothorax rather than vasodilatory shock.
- Obstructive shock — tempting and right because tension pneumothorax impairs venous return and cardiac output, producing obstructive shock.
Answer: D
- The most useful bedside clue separating hypovolemic from cardiogenic shock is JVP/lung findings.
- True or False: Hypotension must be present to diagnose shock. False.
- Name the 3 classic obstructive shock causes tested most often: tension pneumothorax, cardiac tamponade, massive pulmonary embolism.
| Shock type | Preload/JVP | Skin/lungs | Typical trigger | Immediate first move |
|---|---|---|---|---|
| Hypovolemic | Low / flat neck veins | Cool, clammy; lungs often clear | Bleeding, GI losses, dehydration | Crystalloid if nonhemorrhagic; blood if hemorrhagic |
| Cardiogenic | High / elevated JVP | Cool, clammy; crackles | MI, severe cardiomyopathy, arrhythmia | Pressor/inotrope support; treat cause; avoid indiscriminate fluids |
| Distributive | Variable, often low-normal | Warm early; lungs variable | Sepsis, anaphylaxis, neurogenic | Fluids plus cause-specific therapy; pressor if persistent hypotension |
| Obstructive | High / elevated JVP | Often severe dyspnea; lungs or heart clues depend on cause | Tamponade, tension PTX, massive PE | Relieve obstruction urgently |
Exam takeaway: Elevated neck veins with wet lungs strongly support cardiogenic shock, while flat veins with clear lungs support hypovolemia.
1.1.1.5 Application: using perfusion markers, vitals, and bedside data
A Explanation
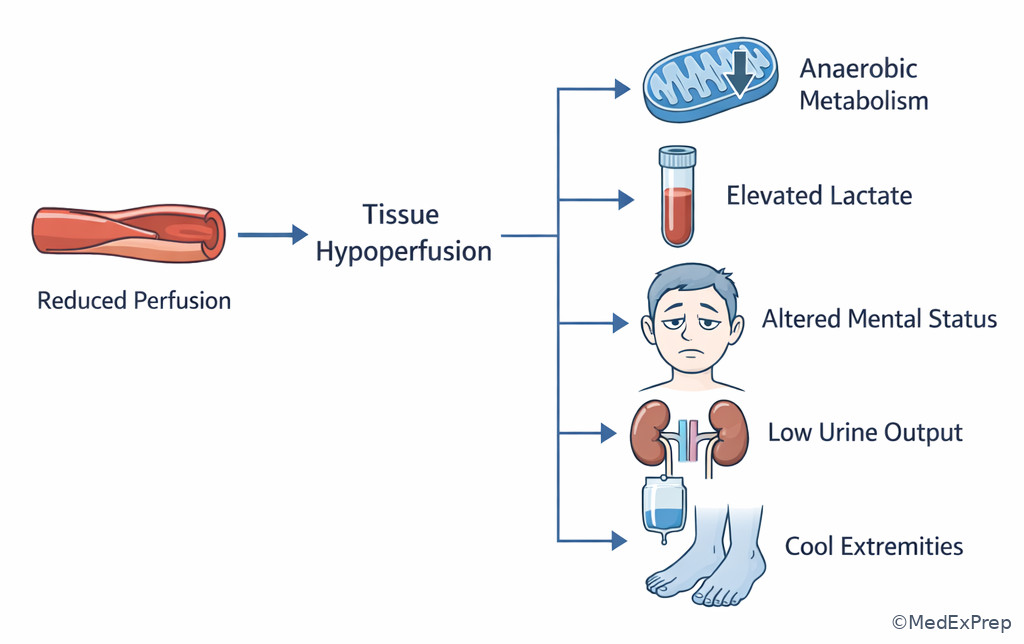
The decision conflict is whether the patient is merely “sick” or truly hypoperfused and at risk for rapid deterioration. The single rule that resolves it is this: organ dysfunction plus abnormal perfusion markers equals shock until proven otherwise, even before blood pressure fully collapses. Key clues are altered mentation, low urine output, delayed capillary refill, cool extremities, rising lactate, metabolic acidosis, and narrow pulse pressure. Tachycardia helps but is not universal; beta-blockers, pacemakers, advanced age, spinal injury, or medications can blunt expected compensatory changes.
WHY THIS IS TESTED: Step 3 often hides early shock behind a “normal” blood pressure or a misleading isolated value. A patient with BP 102/64 mm Hg may still be in compensated shock if the baseline is hypertensive and end-organ perfusion is falling. Conversely, chronic low blood pressure does not equal shock if mentation, urine output, and skin perfusion are preserved. The exam wants you to interpret the whole physiologic pattern, not single numbers.
Lactate is useful because it tracks global hypoperfusion and response to treatment, but it is not specific. Elevated lactate can also occur with seizures, liver dysfunction, or beta-agonists; the trend after resuscitation matters more than a single value. Urine output is a practical bedside metric: falling output suggests inadequate renal perfusion or severe kidney injury. Point-of-care ultrasound can refine decisions quickly: a hyperdynamic underfilled ventricle supports low preload or vasodilation, whereas poor contractility or a large pericardial effusion redirects management. See Fig 3 for a decision visual on hypoperfusion markers.
Exam takeaway: End-organ signs and lactate trend can identify shock before severe hypotension appears.
flowchart LR
A[Patient appears ill] --> B{End-organ signs?}
B -- AMS oliguria cool skin --> C[Assume hypoperfusion]
B -- None --> D[Observe and reassess]
C --> E{Cause likely fluid responsive?}
E -- Yes --> F[Fluids or blood]
E -- No or unclear --> G[POCUS ECG targeted intervention]
F --> H[Reassess MAP urine lactate mental status]
G --> H B Worked example
A 60-year-old man with cirrhosis, hypertension, and chronic atrial fibrillation presents with weakness and black stools. He took ibuprofen for back pain. BP is 106/68 mm Hg, HR 112/min, RR 24/min, oxygen saturation 98% on room air. He is pale, confused, and cool to touch; urine output has been minimal for 6 hours. Hemoglobin is 7.8 g/dL, lactate is 4.4 mmol/L, and INR is 1.6.
Reasoning chain: Identify the task: is he in shock despite a “not terrible” blood pressure? Extract key facts: melena, tachycardia, confusion, oliguria, cool skin, elevated lactate. The distracting detail is atrial fibrillation, which can make tachycardia seem chronic. Apply the rule: end-organ hypoperfusion is present; he has hemorrhagic/hypovolemic shock until proven otherwise. Eliminate “observe and repeat CBC later” because organ perfusion is already failing. Verify: immediate resuscitation with IV access, blood preparation/transfusion strategy, GI bleed management, and close monitoring is appropriate.
C Exam trap
D Checkpoint
Question: Which finding most strongly indicates clinically significant hypoperfusion in a patient with suspected shock?
- Lactate 2.3 mmol/L after a generalized seizure — tempting because lactate is a shock marker, but it is wrong because a seizure can transiently elevate lactate without ongoing circulatory failure.
- Urine output 10 mL/hour with new confusion and cool extremities — tempting and right because multiple end-organ and bedside perfusion markers point to active shock physiology.
- Heart rate 104/min in a patient taking albuterol — tempting because tachycardia accompanies shock, but it is wrong because it is nonspecific and can be medication related.
- Systolic BP 94 mm Hg in a healthy young adult with normal mentation — tempting because the number appears low, but it is wrong because the question asks for the strongest evidence of hypoperfusion, which requires end-organ dysfunction.
Answer: B
| Marker | Why it matters | Common trap | Better interpretation |
|---|---|---|---|
| Lactate | Global hypoperfusion trend | Treating a single mild value as diagnostic alone | Interpret with perfusion signs and repeat after therapy |
| Urine output | Kidney perfusion marker | Ignoring it in non-ICU stems | Low output plus other signs suggests shock |
| Mental status | Brain perfusion marker | Attributing confusion only to age or infection | New confusion in unstable patient is hypoperfusion until proven otherwise |
| Skin temperature/cap refill | Peripheral perfusion | Dismissing as subjective | Helpful when integrated with JVP and lungs |
| Blood pressure | Late or incomplete marker | Using a single cutoff as the sole definition | Trend with pulse pressure and organ dysfunction |
Exam takeaway: Use lactate as a trend within a broader perfusion assessment, not as an isolated diagnosis.
1.1.1.6 Application: choosing the immediate intervention
A Explanation
The central Step 3 conflict is no longer “what is the diagnosis?” but “what is the first therapy that changes outcome?” The rule is match the intervention to the mechanism of shock. If hemorrhage or severe volume loss is driving shock, replace volume appropriately—blood for major bleeding, crystalloid for nonhemorrhagic losses. If vasodilation is dominant and fluid responsiveness is limited or exhausted, start a vasopressor. If pump failure is dominant, support pressure and contractility while treating the cause; avoid drowning the lungs with reflexive fluids. If mechanical obstruction is the cause, remove the obstruction now.
WHY THIS IS TESTED: multiple answer choices are often individually useful somewhere in the patient’s course. The exam separates the candidate who knows the disease from the candidate who knows the sequence. Needle decompression comes before chest x-ray in tension pneumothorax. IM epinephrine comes before antihistamines in anaphylaxis. Pericardiocentesis is definitive for tamponade after immediate recognition and stabilization. Early antibiotics matter in sepsis, but they do not replace airway or perfusion support.
Watch for “fluids first” bias. Fluids are appropriate when preload is low or distributive vasodilation is suspected, but small test boluses and reassessment are safer than routine liters in the patient with crackles or high JVP. Vasopressors are not a substitute for blood loss control, and blood products are not the answer to pure anaphylaxis. Mechanism drives treatment.
B Worked example
A 29-year-old woman with asthma, eczema, and peanut allergy arrives after restaurant exposure with diffuse urticaria, vomiting, hoarse voice, wheezing, and BP 84/50 mm Hg. She took diphenhydramine at home. A nurse notes that the wheeze improved slightly after an albuterol nebulizer started in triage. The team asks for the most appropriate next step.
Reasoning chain: Identify task: choose the immediate therapy. Extract key facts: allergen exposure, mucosal/airway symptoms, wheeze, GI symptoms, hypotension. The distracting clue is slight bronchodilator improvement, which makes albuterol feel sufficient. Apply the rule: anaphylaxis with shock requires IM epinephrine first. Eliminate steroids and antihistamines as initial answers; they are adjuncts. Verify: epinephrine addresses airway edema, bronchospasm, and vasodilation, the life-threatening triad here.
C Exam trap
D Checkpoint
Question: A 64-year-old man with ischemic cardiomyopathy presents with chest pressure, cool extremities, BP 80/48 mm Hg, elevated JVP, bibasilar crackles, and new ST depressions. Which is the most appropriate initial management principle?
- Large-volume crystalloid bolus — tempting because hypotension often prompts fluids, but it is wrong because elevated JVP and crackles indicate high filling pressures and cardiogenic physiology.
- Immediate vasopressor/inotrope support with evaluation for acute coronary cause — tempting and right because this presentation is cardiogenic shock requiring hemodynamic support and cause-directed management.
- IM epinephrine — tempting because shock is present, but it is wrong because there is no allergic trigger or anaphylaxis pattern.
- Needle thoracostomy — tempting because obstructive shock is a key emergency, but it is wrong because there are no unilateral breath sound changes or procedural trigger.
Answer: B
- The first-line treatment for anaphylactic shock is IM epinephrine.
- True or False: Tension pneumothorax should be confirmed by chest x-ray before decompression. False.
- Massive hemorrhage responds best to blood products and bleeding control, not crystalloid alone.
| Presentation | Tempting but wrong first step | Correct first step | Discriminator |
|---|---|---|---|
| Anaphylaxis with hypotension | Antihistamine alone | IM epinephrine | Airway symptoms or shock after allergen exposure |
| Tension pneumothorax | Chest x-ray first | Immediate decompression | Hypotension + unilateral absent breath sounds + distended neck veins |
| Hemorrhagic shock | Large crystalloid-only resuscitation | Blood products and control bleeding | Active blood loss or strong bleeding source |
| Cardiogenic shock | Routine large fluid bolus | Hemodynamic support and treat cardiac cause | Wet lungs + elevated JVP + low output |
| Cardiac tamponade | Delayed observation | Urgent drainage after recognition/stabilization | Shock + elevated JVP + effusion/Beck-type clues |
Exam takeaway: Sudden hypotension with unilateral absent breath sounds is a treat-now diagnosis, not an image-first diagnosis.
See Fig 4 whenever a post-procedure or trauma stem gives unilateral absent breath sounds plus hypotension.
Exam takeaway: Hypotension plus airway or bronchospastic symptoms after exposure means epinephrine first.
1.1.1.7 Integration: reassessment, monitoring, and when to escalate
A Explanation
After the first intervention, the decision conflict becomes whether to continue the current plan, escalate support, or pivot because the physiology was misclassified. The rule is every shock intervention requires a timed reassessment of perfusion and a disposition decision. Step 3 does not reward “give fluids” as a complete answer if you never check whether they worked. Reassess mental status, MAP, heart rate, urine output, oxygen requirement, work of breathing, capillary refill, and lactate trend when appropriate. If a patient remains hypotensive after a reasonable initial fluid challenge, ask why: ongoing bleeding, persistent vasodilation, pump failure, obstruction, or impending respiratory collapse may require a different next step.
WHY THIS IS TESTED: the exam increasingly emphasizes physician-level longitudinal thinking. A patient who transiently improves but still has rising oxygen needs or falling urine output is not “fixed.” Safe practice includes ICU recognition, early consultant involvement, and avoiding premature transfer or discharge.
Escalate early when vasoactive medications, invasive monitoring, intubation, urgent procedure, or continuous reassessment is needed. Admit patients with persistent shock physiology, ongoing bleeding, escalating oxygen requirement, or uncertain response. Discharge is wrong if the cause has not been stabilized and perfusion has not normalized. See Fig 5 for a mini-algorithm of post-resuscitation reassessment.
Exam takeaway: Response to therapy determines whether to continue, escalate, or rethink the shock mechanism and disposition.
flowchart TD
A[Initial intervention given] --> B{Perfusion improved?}
B -- Yes --> C[Continue targeted therapy and identify definitive cause]
B -- No --> D{Mechanism correct?}
D -- No --> E[Reclassify shock with bedside data POCUS ECG]
D -- Yes --> F[Escalate: pressor blood airway procedure ICU]
C --> G[Safe disposition planning]
E --> G
F --> G B Worked example
A 48-year-old man with pancreatitis, obesity, and alcohol use disorder is admitted for hypotension. After 2 L isotonic crystalloid, BP rises from 82/48 to 96/60 mm Hg, but he remains tachycardic, confused, and oliguric; lactate falls only from 5.0 to 4.7 mmol/L. He now requires 4 L oxygen for new tachypnea. The intern proposes transfer to the floor because the blood pressure improved.
Reasoning chain: Identify task: determine response and disposition. Extract key facts: only partial pressure improvement, persistent end-organ hypoperfusion, rising respiratory needs. The distracting clue is the numerically improved blood pressure. Apply the rule: response is inadequate because perfusion markers remain abnormal. Eliminate floor transfer; the patient still needs close monitoring and likely escalation. Verify: ICU or step-up level care with continued reassessment is safest.
C Exam trap
D Checkpoint
Question: After initial treatment for septic-appearing shock, which finding most strongly indicates the need for escalation rather than routine floor admission?
- BP improved from 84/50 to 98/62 mm Hg, but urine output remains 10 mL/hour — tempting because the pressure improved, but it is right because persistent oliguria shows ongoing hypoperfusion requiring closer monitoring/escalation.
- Temperature remains 38.5°C after acetaminophen — tempting because fever implies severity, but it is wrong because fever alone is less decisive than ongoing end-organ hypoperfusion.
- White blood cell count rises from 14,000 to 16,000/µL — tempting because infection seems worse, but it is wrong because disposition should be driven by hemodynamics and organ perfusion, not WBC alone.
- Lactate is 2.1 mmol/L and mental status normalized — tempting because lactate is important, but it is wrong as a trigger for escalation because these findings actually suggest improvement.
Answer: A
1.1.1.8 Integration: high-yield differentials and source-specific rescue decisions
A Explanation
This final integration section asks you to choose between shock look-alikes and shock subtypes that demand different rescue actions. The rule is that one discriminating clue often separates a life-saving intervention from a dangerous delay. Tension pneumothorax versus massive PE: both can cause obstructive shock with JVP elevation and hypoxemia, but unilateral absent breath sounds after a procedure points to tension PTX, whereas clear lungs with sudden pleuritic symptoms and right-heart strain clues point toward PE. Tamponade versus cardiogenic shock: both may raise JVP and lower output, but a pericardial effusion or muffled heart sounds with pulsus paradoxus shifts toward tamponade. Septic shock versus hemorrhagic shock: both can produce lactate elevation and tachycardia, but bleeding source, melena, trauma, or postpartum hemorrhage changes the resuscitation target to blood and bleeding control.
WHY THIS IS TESTED: these close-call differentials generate the strongest distractors because the wrong options are not absurd—they are correct for a slightly different patient. The board wants you to use a single bedside clue, timing feature, or exam finding to choose the safest next step.
Also distinguish treatment sequence from definitive cure. Massive PE may require anticoagulation or reperfusion strategy, but first you stabilize airway and circulation and obtain urgent specialty involvement when indicated. Cardiogenic shock from MI needs hemodynamic support plus urgent evaluation for reperfusion. Hemorrhagic shock needs blood and control of the bleeding source; endoscopy, surgery, obstetric intervention, or trauma activation may be the actual lifesaving next layer. See Fig 6 for a rescue-focused comparison algorithm.
Exam takeaway: One bedside discriminator often decides between decompression, blood, epinephrine, cardiac support, or obstruction relief.
flowchart TD
A[Shock patient] --> B{Allergen exposure with airway or skin findings?}
B -- Yes --> C[IM epinephrine]
B -- No --> D{Bleeding source or volume loss?}
D -- Yes --> E[Blood and control hemorrhage]
D -- No --> F{Wet lungs and high JVP after cardiac event?}
F -- Yes --> G[Cardiogenic support]
F -- No --> H{Unilateral absent breath sounds or tamponade clue?}
H -- Yes --> I[Relieve obstruction urgently]
H -- No --> J[Consider distributive or PE-focused pathway] B Worked example
A 33-year-old postpartum woman develops sudden hypotension, tachycardia, and shortness of breath one hour after delivery complicated by heavy vaginal bleeding. She also has asthma and mild wheezing from a recent viral illness. BP is 74/40 mm Hg, HR 138/min, oxygen saturation 91%, uterus is boggy, and ongoing vaginal bleeding is present. The tempting clue is the wheeze, which makes anaphylaxis or bronchospasm seem plausible.
Reasoning chain: Identify task: select the lifesaving immediate intervention. Extract key facts: postpartum status, heavy bleeding, boggy uterus, profound hypotension. The distracting clue is wheeze. Apply the rule: hemorrhagic shock from postpartum hemorrhage is the dominant process; prioritize blood resuscitation, uterotonic management, hemorrhage control, and obstetric escalation. Eliminate bronchodilator-centered management as first-line because it does not address the cause of circulatory collapse. Verify: this is a circulation-first hemorrhage stem, not a primary airway-allergy scenario.
C Exam trap
D Checkpoint
Question: A 58-year-old man presents with sudden hypotension, tachycardia, distended neck veins, and muffled heart sounds 3 days after a malignancy-related pericardial effusion was noted. Lungs are clear. Which is the most appropriate next step?
- Large crystalloid bolus alone and observation — tempting because tamponade is preload dependent, but it is wrong because definitive urgent relief of obstruction is required.
- Urgent pericardial drainage with stabilization measures — tempting and right because obstructive shock from tamponade requires prompt drainage after recognition.
- High-dose diuretics — tempting because JVP is elevated, but it is wrong because reducing preload worsens tamponade physiology.
- Empiric broad-spectrum antibiotics — tempting because malignancy patients can be septic, but it is wrong because the triad points to tamponade, not distributive shock.
Answer: B
Exam takeaway: Shock with elevated JVP and clear lungs should trigger tamponade vs PE thinking, not reflex fluids alone.
Exam takeaway: Source clues such as active bleeding shift first-line resuscitation from vasodilation-focused care to blood-centered resuscitation.
Exam Traps & Differentiators
- Most common wrong answer and why: choosing a diagnostic test before stabilization. It is tempting because the stem strongly hints at the eventual diagnosis, but the single clue that eliminates the test-first answer is any ABC failure or end-organ hypoperfusion.
- Looks similar but isn’t: cardiogenic shock vs hypovolemia. Both can be cool and tachycardic; wet lungs/elevated JVP favor cardiogenic shock, while flat neck veins/clear lungs favor hypovolemia.
- Looks similar but isn’t: tension pneumothorax vs massive PE. Both can cause obstructive shock and distended neck veins; unilateral absent breath sounds after procedure/trauma points to tension PTX.
- Looks similar but isn’t: anaphylaxis vs asthma exacerbation. Both wheeze; hypotension, hives, GI symptoms, or hoarseness after exposure points to anaphylaxis and epinephrine first.
- Looks similar but isn’t: sepsis vs hemorrhage. Both elevate lactate; active bleeding source or melena/postpartum hemorrhage shifts resuscitation to blood and source control.
| If the stem says... | Think... | Reject... |
|---|---|---|
| Cannot speak full sentences, stridor, gurgling, severe somnolence | Airway/ventilation first | CT or ABG before airway support |
| Cool, clammy, elevated JVP, crackles after MI | Cardiogenic shock | Routine large fluid bolus |
| Warm flushed patient with infection clues and hypotension | Distributive/septic physiology | Delay fluids and antibiotics while waiting for perfect data |
| Distended neck veins plus unilateral absent breath sounds | Tension pneumothorax | Chest x-ray first |
| Hives, hoarseness, wheeze, hypotension after exposure | Anaphylactic shock | Antihistamine-only therapy |
| Oliguria, confusion, lactate elevation despite BP near normal | Compensated shock/hypoperfusion | Reassurance based on BP alone |
Related future traps: in Sepsis and Time-Sensitive Care, the distractor often becomes “wait for cultures or imaging before antibiotics,” whereas in Disposition of Unstable Patients, the distractor becomes “premature floor transfer after partial response.” Those are extensions of the same core error taught in Fig 1 and Fig 5.
Algorithm / Approach
Rapid Review
- Airway compromise → inability to protect airway outranks imaging
- Hypoperfusion → confusion or oliguria beats “acceptable” BP
- Hypovolemic shock → flat neck veins with clear lungs
- Cardiogenic shock → wet lungs plus elevated JVP after cardiac event
- Distributive shock → warm vasodilated bedside appearance early
- Obstructive shock → elevated JVP with a mechanical clue
- Tension pneumothorax → unilateral absent breath sounds mandates decompression
- Tamponade → elevated JVP with clear lungs and effusion clues
- Anaphylaxis → hypotension plus airway/skin/GI symptoms means epinephrine first
- Hemorrhagic shock → blood and source control outperform crystalloid-only resuscitation
- Lactate → trend marker, not stand-alone diagnosis
- Response to treatment → persistent oliguria means resuscitation is incomplete
- Disposition → pressor need or ongoing shock physiology implies ICU-level care
Self-check quiz
1. A 45-year-old man with hypertension and alcohol use disorder presents with hematemesis. He is pale, cool, confused, and making very little urine. BP is 104/66 mm Hg, HR 118/min. Which finding most strongly supports shock rather than simple anxiety-related tachycardia?
- Heart rate 118/min
- Urine output 10 mL/hour with confusion
- Systolic BP 104 mm Hg
- Respiratory rate 22/min
2. A 31-year-old woman with eczema and allergic rhinitis develops hives, vomiting, hoarseness, wheezing, and BP 82/48 mm Hg minutes after eating shellfish. Which is the best initial therapy?
- IV methylprednisolone
- Albuterol nebulization
- IM epinephrine
- Diphenhydramine
3. A 69-year-old man with diabetes, prior MI, and chronic kidney disease presents with chest pressure and dyspnea. BP is 78/46 mm Hg, HR 122/min, neck veins are distended, lungs have diffuse crackles, and extremities are cool. Which is the most appropriate next step in management?
- Administer a 2-L crystalloid bolus
- Begin hemodynamic support for cardiogenic shock and urgent cardiac evaluation
- Give IM epinephrine
- Perform immediate needle thoracostomy
4. A 40-year-old woman with breast cancer undergoes central venous catheter placement. Minutes later she becomes acutely dyspneic and hypotensive. BP is 74/42 mm Hg, HR 136/min, oxygen saturation 80%, neck veins are distended, and breath sounds are absent on the right. What is the most appropriate next step?
- Portable chest x-ray
- CT angiography of the chest
- Immediate decompression of the right chest
- IV furosemide
5. A 58-year-old man with cirrhosis and osteoarthritis presents with melena after taking daily ibuprofen. BP is 98/60 mm Hg, HR 116/min, he is confused and cool, urine output is low, and lactate is 4.8 mmol/L. Which is the most appropriate interpretation?
- He is not in shock because the systolic BP is above 90 mm Hg
- He has likely compensated hemorrhagic shock with end-organ hypoperfusion
- He most likely has isolated medication-induced tachycardia
- He can be safely observed while awaiting repeat CBC in 6 hours
6. A 62-year-old woman with metastatic lung cancer and a known pericardial effusion presents with hypotension and dyspnea. BP is 80/50 mm Hg, HR 124/min, neck veins are distended, heart sounds are distant, and lungs are clear. Which is the most appropriate next step?
- Urgent pericardial drainage with stabilization
- Large-volume crystalloid bolus followed by floor admission
- High-dose IV diuretics
- Immediate broad-spectrum antibiotics as sole first action
7. A 70-year-old man with COPD, coronary artery disease, and obesity presents with fever, cough, hypotension, and hypoxemia. After oxygen, IV access, and an initial fluid bolus, BP rises from 82/48 to 96/60 mm Hg. He remains confused, urine output is 12 mL/hour, and lactate is 4.6 mmol/L. Which disposition is most appropriate?
- Discharge with oral antibiotics because the blood pressure improved
- Routine medical floor admission because the MAP is now acceptable
- ICU-level care or equivalent escalation because end-organ hypoperfusion persists
- Observation unit only, pending repeat lactate tomorrow
8. A 27-year-old postpartum woman develops severe hypotension 30 minutes after delivery. She has active vaginal bleeding, a boggy uterus, HR 142/min, oxygen saturation 93%, and mild expiratory wheezing from a recent viral illness. Which is the most appropriate immediate management focus?
- Treat bronchospasm first with repeated nebulizers only
- Initiate blood-centered resuscitation and hemorrhage control
- Observe for spontaneous uterine contraction while trending vitals
- Give antihistamines for possible allergic reaction
Answer key
1. Correct answer: B
- A. Heart rate 118/min: tempting because tachycardia is common in shock; incorrect for this specific scenario because tachycardia alone is nonspecific and can reflect anxiety, pain, fever, or volume loss without proving end-organ hypoperfusion. Single stem clue: confusion and oliguria are stronger perfusion markers. Source: Harrison’s Principles of Internal Medicine; UpToDate on evaluation of shock.
- B. Urine output 10 mL/hour with confusion: tempting because it bundles multiple abnormalities; correct because kidney and brain hypoperfusion together indicate clinically significant shock physiology even when blood pressure is not profoundly low. Single stem clue: low urine output plus altered mental status. Source: Harrison’s; First Aid for the USMLE Step 3.
- C. Systolic BP 104 mm Hg: tempting because learners over-anchor on BP thresholds; incorrect because a near-normal BP does not exclude compensated shock. Single stem clue: preserved systolic pressure despite end-organ dysfunction. Source: Harrison’s; UpToDate.
- D. Respiratory rate 22/min: tempting because tachypnea occurs in shock; incorrect because mild tachypnea is less specific than oliguria and confusion. Single stem clue: organ dysfunction, not respiratory rate alone, discriminates. Source: UpToDate; Harrison’s.
2. Correct answer: C
- A. IV methylprednisolone: tempting because steroids are commonly used in allergic reactions; incorrect because they are adjunctive and do not rapidly reverse airway edema, bronchospasm, and hypotension. Single stem clue: shock with hoarseness and wheezing after exposure. Source: UpToDate on anaphylaxis; First Aid.
- B. Albuterol nebulization: tempting because wheeze suggests bronchospasm; incorrect because bronchodilation alone does not treat systemic anaphylaxis or hypotension. Single stem clue: hypotension and multisystem involvement. Source: UpToDate; Harrison’s.
- C. IM epinephrine: tempting and correct because it is the first-line treatment for anaphylaxis, addressing vasodilation, mucosal edema, and bronchospasm. Single stem clue: hives plus GI symptoms plus airway symptoms plus hypotension after shellfish. Source: UpToDate; NEJM review on anaphylaxis.
- D. Diphenhydramine: tempting because hives are prominent; incorrect because antihistamines treat cutaneous symptoms but not life-threatening shock. Single stem clue: BP 82/48 mm Hg requires epinephrine first. Source: UpToDate; Harrison’s.
3. Correct answer: B
- A. Administer a 2-L crystalloid bolus: tempting because hypotension often triggers reflex fluid resuscitation; incorrect because elevated JVP and diffuse crackles indicate high filling pressures and cardiogenic shock. Single stem clue: wet lungs plus distended neck veins after cardiac symptoms. Source: Harrison’s; AHA/ACC guidance for cardiogenic shock principles.
- B. Begin hemodynamic support for cardiogenic shock and urgent cardiac evaluation: tempting and correct because pump failure after ischemic symptoms requires pressure/forward-flow support and urgent cause-directed cardiac management. Single stem clue: chest pressure with cool extremities, crackles, and elevated JVP. Source: AHA/ACC guidelines; UpToDate.
- C. Give IM epinephrine: tempting because the patient is hypotensive; incorrect because there is no allergic trigger or anaphylaxis phenotype. Single stem clue: cardiac presentation dominates. Source: UpToDate; Harrison’s.
- D. Perform immediate needle thoracostomy: tempting because obstructive shock can mimic this picture; incorrect because there is no unilateral absent breath sound or procedure/trauma trigger. Single stem clue: diffuse crackles rather than unilateral lung finding. Source: Harrison’s; ATLS principles referenced in acute care texts.
4. Correct answer: C
- A. Portable chest x-ray: tempting because it confirms pneumothorax; incorrect because unstable tension pneumothorax is treated immediately, not imaged first. Single stem clue: hypotension after line placement with absent unilateral breath sounds and JVD. Source: Harrison’s; emergency care standards.
- B. CT angiography of the chest: tempting because PE is a shock cause in cancer patients; incorrect because the timing after line placement and unilateral absent breath sounds point away from PE. Single stem clue: absent breath sounds on the right. Source: UpToDate; Harrison’s.
- C. Immediate decompression of the right chest: tempting and correct because this is obstructive shock from tension pneumothorax and decompression is lifesaving. Single stem clue: post-procedure sudden deterioration with JVD and unilateral absent breath sounds. Source: ATLS-aligned emergency management; Harrison’s.
- D. IV furosemide: tempting because dyspnea and JVD may suggest volume overload; incorrect because this is mechanical obstruction, not cardiogenic pulmonary edema. Single stem clue: abrupt onset after central line placement. Source: UpToDate; Harrison’s.
5. Correct answer: B
- A. He is not in shock because the systolic BP is above 90 mm Hg: tempting because of a common threshold myth; incorrect because shock is defined by hypoperfusion, not only by BP. Single stem clue: confusion, oliguria, cool skin, and high lactate. Source: Harrison’s; UpToDate.
- B. He has likely compensated hemorrhagic shock with end-organ hypoperfusion: tempting and correct because melena plus NSAID use plus low urine output and altered mentation indicate bleeding-related hypoperfusion despite a borderline blood pressure. Single stem clue: GI bleeding source with end-organ signs. Source: Harrison’s; First Aid.
- C. He most likely has isolated medication-induced tachycardia: tempting because medications can affect vitals; incorrect because the multisystem perfusion pattern is far more concerning than isolated tachycardia. Single stem clue: lactate 4.8 with low urine output. Source: UpToDate; Harrison’s.
- D. He can be safely observed while awaiting repeat CBC in 6 hours: tempting because bleeding evaluation often includes serial hemoglobin; incorrect because current perfusion failure requires immediate resuscitative management. Single stem clue: ongoing shock markers now, not later. Source: Harrison’s; acute GI bleed management reviews.
6. Correct answer: A
- A. Urgent pericardial drainage with stabilization: tempting and correct because known effusion plus hypotension, JVD, distant heart sounds, and clear lungs indicates tamponade causing obstructive shock. Single stem clue: clear lungs despite elevated JVP and known pericardial effusion. Source: Harrison’s; UpToDate on cardiac tamponade.
- B. Large-volume crystalloid bolus followed by floor admission: tempting because temporary preload support may help; incorrect because it is not definitive and floor admission is unsafe in active obstructive shock. Single stem clue: current shock state requires urgent drainage and higher level care. Source: UpToDate; Harrison’s.
- C. High-dose IV diuretics: tempting because JVD implies high filling pressures; incorrect because lowering preload worsens tamponade physiology. Single stem clue: lungs are clear and tamponade signs are present. Source: Harrison’s; UpToDate.
- D. Immediate broad-spectrum antibiotics as sole first action: tempting because cancer patients are infection-prone; incorrect because the presentation fits tamponade more specifically than sepsis. Single stem clue: distant heart sounds plus known effusion. Source: UpToDate; Harrison’s.
7. Correct answer: C
- A. Discharge with oral antibiotics because the blood pressure improved: tempting because one number improved; incorrect because persistent confusion, oliguria, and elevated lactate show ongoing shock physiology. Single stem clue: end-organ hypoperfusion after treatment. Source: UpToDate; Harrison’s.
- B. Routine medical floor admission because the MAP is now acceptable: tempting because the patient no longer looks profoundly hypotensive on paper; incorrect because organ perfusion remains inadequate and close hemodynamic reassessment is needed. Single stem clue: urine output 12 mL/hour. Source: critical care standards summarized in Harrison’s and UpToDate.
- C. ICU-level care or equivalent escalation because end-organ hypoperfusion persists: tempting and correct because partial numeric improvement without recovery of perfusion markers indicates ongoing instability requiring escalation. Single stem clue: confusion plus oliguria plus lactate 4.6 after initial resuscitation. Source: UpToDate; Harrison’s.
- D. Observation unit only, pending repeat lactate tomorrow: tempting because trending lactate is appropriate; incorrect because waiting until tomorrow ignores a currently unstable physiology. Single stem clue: need for immediate ongoing reassessment, not delayed observation. Source: Harrison’s; UpToDate.
8. Correct answer: B
- A. Treat bronchospasm first with repeated nebulizers only: tempting because wheezing is present; incorrect because mild wheeze does not explain severe postpartum hypotension with active vaginal bleeding and a boggy uterus. Single stem clue: ongoing hemorrhage source. Source: obstetric emergency guidance; Harrison’s.
- B. Initiate blood-centered resuscitation and hemorrhage control: tempting and correct because postpartum hemorrhage causing hemorrhagic shock requires immediate resuscitation and uterine/obstetric hemorrhage management. Single stem clue: boggy uterus with active bleeding. Source: ACOG-aligned postpartum hemorrhage guidance; UpToDate.
- C. Observe for spontaneous uterine contraction while trending vitals: tempting because uterine atony can improve with time; incorrect because active shock demands immediate intervention, not observation. Single stem clue: HR 142/min and profound hypotension. Source: UpToDate; obstetric emergency texts.
- D. Give antihistamines for possible allergic reaction: tempting because wheeze can suggest allergic disease; incorrect because no allergen-linked airway/skin pattern is given, and massive bleeding explains the shock. Single stem clue: postpartum hemorrhage findings outweigh nonspecific wheeze. Source: UpToDate; Harrison’s.