Why it matters
- PANRE questions often become easy or hard based on whether you recognize the task type before reading details.
- Many wrong answers are not medically absurd; they are answers to the wrong question—correct treatment when the item asks for diagnosis, or correct test when the patient first needs stabilization.
- As a PA-facing exam, PANRE rewards safe generalist reasoning: identify acuity, order common studies, start evidence-based care, and escalate when needed.
- This lesson provides the framework used throughout the course, so later cardiology, pulmonary, GI, endocrine, neurology, and preventive care topics all fit into one repeatable approach.
Exam takeaway: Decide the task first, then match the best diagnosis, test, treatment, or disposition to that task.
flowchart TD
A[Read last line first] --> B{What is being asked?}
B -->|Diagnosis| C[Identify discriminating finding]
B -->|Evaluation| D[Choose best test]
B -->|Management| E[Choose first safe action]
B -->|Disposition| F[Decide outpatient vs ED vs admit]
C --> G[Eliminate look-alikes]
D --> G
E --> G
F --> G
G --> H[Verify safety and contraindications] Use this lesson as the master framework for all later topics. See Fig 1.
Key Terms & Must-Know Facts
1.1.1.1 Key terms
- Task type: The specific action the question asks for: diagnosis, evaluation, management, monitoring, prevention, or disposition.
- Stem cue: Wording that signals the task, such as “most likely diagnosis” or “most appropriate next step.”
- Discriminating finding: The single clue that separates the right answer from the closest distractor.
- Next best step: The safest, most appropriate immediate action for the exact scenario.
- Initial management: First-line treatment or stabilization before definitive therapy.
- Disposition: Where the patient should go next: home, close follow-up, urgent referral, ED transfer, or admission.
- Red flag: Clinical feature suggesting serious disease, instability, or need for escalation.
- Clinical noise: Extra details in the stem that are true but not decisive.
- Generalist scope: PANRE-level expectation for broad, practical PA clinical reasoning.
- Contraindication: A finding that makes a test or treatment unsafe or inappropriate.
- Premature closure: Choosing an answer too early based on one familiar clue.
- Pattern recognition: Identifying classic presentations quickly, then verifying with a rule-out step.
- Escalation threshold: The point at which specialist consultation, ED transfer, or admission is required.
1.1.1.2 Must-know facts
- Read the last line first; it often reveals the task type before the details bias you.
- If the patient is unstable, stabilization outranks diagnostic completeness.
- The correct answer is usually the one that is best for this patient now, not the most comprehensive plan overall.
- Distractors are commonly answers for a slightly different patient or a later step.
- PANRE tests broad clinical reasoning across organ systems, not narrow subspecialty trivia.
- When recommendations vary by setting or guideline version, the exam favors the broadly accepted safe next step.
- A strong answer matches both the disease pattern and the question verb.
- PA framing matters: recognize when to treat directly versus when to stabilize and consult or refer.
| Question wording | Task type | What you should do mentally | Common trap |
|---|---|---|---|
| Most likely diagnosis | Diagnosis | Match pattern to illness script | Picking treatment you already know |
| Best initial test | Evaluation | Choose the study that changes next action | Ordering definitive but unnecessary testing first |
| Most appropriate next step | Management or evaluation | Check stability first, then urgency | Ignoring airway, breathing, circulation, or severe red flags |
| Best initial therapy | Treatment | Choose first-line care for current severity | Jumping to second-line or specialist therapy |
| Requires immediate clarification | Safety/medication review | Look for contraindication, pregnancy, interaction, or dangerous omission | Focusing on efficacy instead of safety |
| Most important to monitor | Monitoring/follow-up | Link treatment to toxicity or response marker | Choosing a non-actionable lab or symptom |
Core content
1.1.1.3 Foundational task types: what PANRE is really asking
A Explanation
PANRE does not reward memorization alone; it rewards recognition of which clinical job the stem wants you to do. The decision conflict is usually this: Do I identify the disease, choose a test, start treatment, or decide disposition? The single rule that resolves the conflict is simple: the last line defines the task, and the rest of the stem provides the evidence. If the last line asks for “most likely diagnosis,” then even a brilliant treatment plan is wrong. If it asks for “most appropriate next step,” you must first decide whether the patient is stable enough for workup or instead needs immediate intervention.
WHY THIS IS TESTED: Many examinees know the disease but miss the item because they answer the wrong task category. PANRE commonly turns one clinical scenario into different question types: diagnosis, confirmatory testing, initial therapy, long-term management, complication recognition, or referral.
Choose-vs-reject framing helps. Choose diagnosis mode when the question asks what the patient has. Choose evaluation mode when the disease is suspected but not yet established and a study will change the next move. Choose management mode when the diagnosis is clear enough and the exam tests what to do now. Reject the urge to over-advance to later steps unless the stem explicitly asks for them.
B Worked example
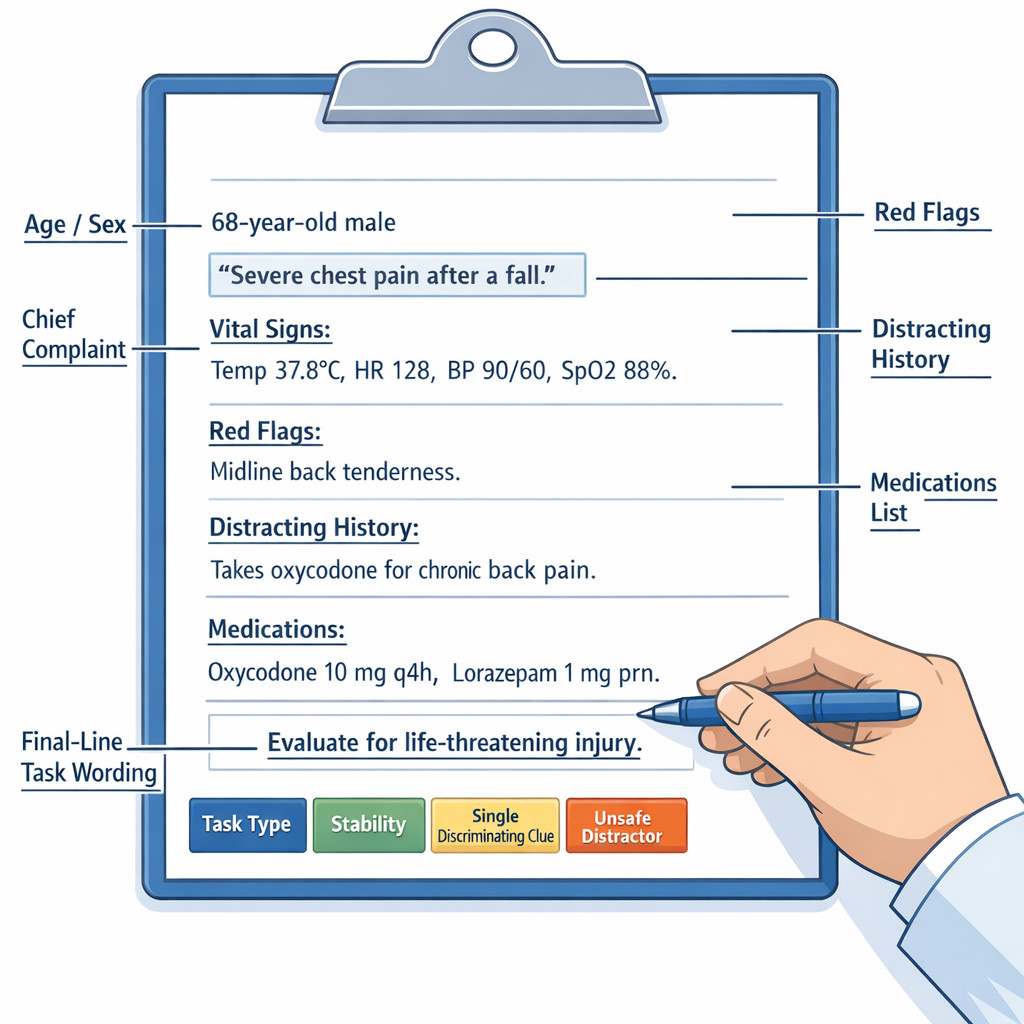
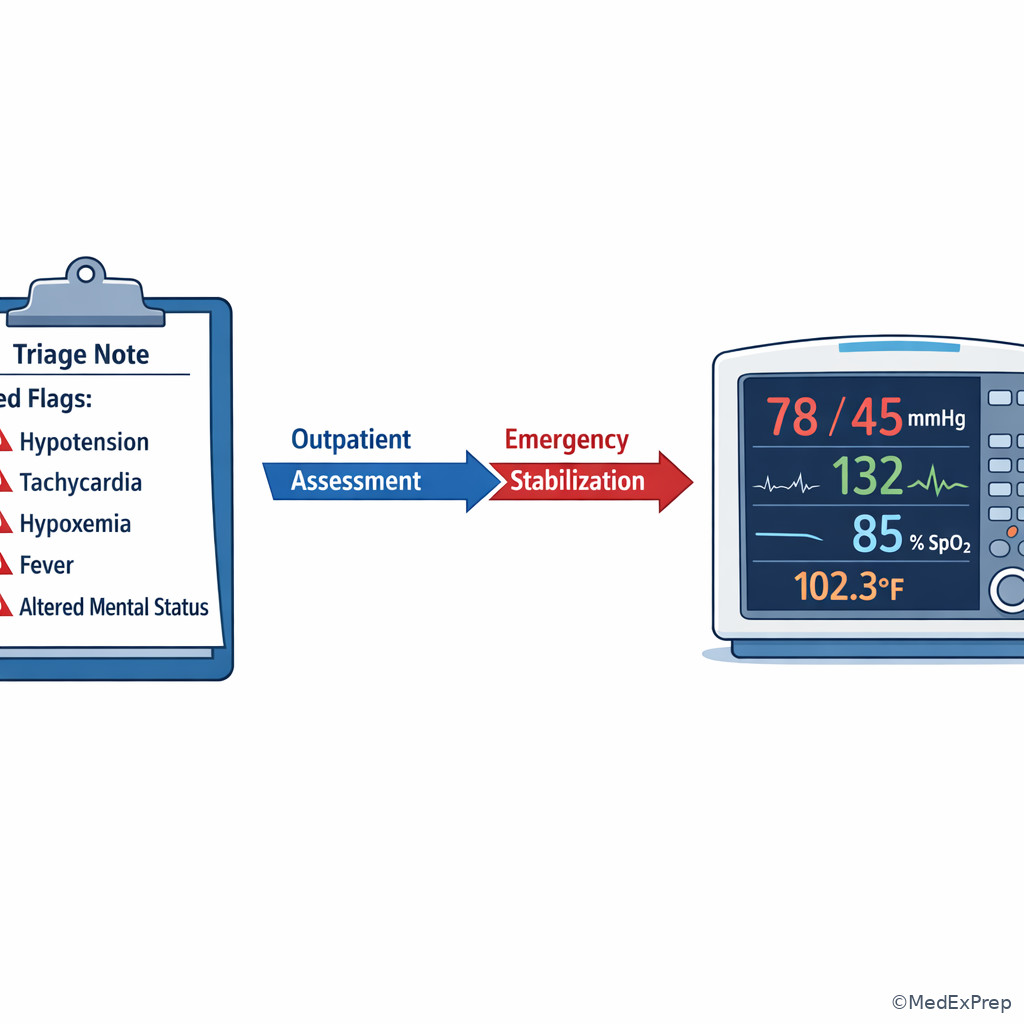
A 58-year-old man with hypertension, type 2 diabetes, and GERD presents with 90 minutes of chest pressure radiating to the left arm. He reports a similar but milder episode after climbing stairs last week. He took antacids without relief. Blood pressure is 88/56 mm Hg, pulse 118/min, oxygen saturation 91% on room air. The stem asks: “What is the most appropriate next step?” A tempting-but-wrong clue is his prior exertional discomfort, which may pull you toward stable angina evaluation.
Reasoning chain: Identify task: next best step, not diagnosis alone. Extract key facts: hypotension, tachycardia, hypoxemia, ongoing ischemic-type pain. Apply rule: unstable patients are stabilized and managed emergently before outpatient-style testing. Eliminate distractors: stress testing is wrong because he is unstable; empiric GERD treatment ignores shock physiology; coronary CT angiography is not first in an unstable high-risk patient. Verify: the best next step is emergency ACS management and escalation, not elective diagnostic sorting.
C Exam trap
D Checkpoint
Question: A 34-year-old woman with asthma and migraine presents with unilateral throbbing headache, photophobia, and nausea. Neurologic examination is normal, and she has had similar episodes monthly. The stem asks, “Which of the following is the most likely diagnosis?” Which approach is best?
- Choose acute migraine treatment immediately. Tempting because the pattern strongly suggests migraine, but wrong because the question asks for diagnosis rather than management.
- Choose migraine as the diagnosis. Tempting because it fits recurrent unilateral throbbing headache with photophobia; right because the task is diagnosis and the pattern supports migraine.
- Order brain MRI first. Tempting because imaging can feel safer, but wrong because there are no red flags and the stem is asking for diagnosis, not evaluation.
- Refer urgently to neurology. Tempting because headache can be serious, but wrong because the scenario lacks focal deficits, thunderclap onset, or other escalation triggers.
Best answer: B.
1.1.1.4 Scope-aware reasoning: what a PANRE PA is expected to do
A Explanation
The decision conflict here is not disease versus disease; it is manage directly versus stabilize and escalate. PANRE expects a certified PA to function as a broad generalist: obtain history, perform assessment, order common labs and imaging, initiate evidence-based therapy for common conditions, monitor response, and recognize when the patient needs ED transfer, admission, or specialist input. The single rule that resolves most scope questions is this: choose the safest broadly accepted clinical action within routine PA practice, and escalate when acuity or complexity exceeds routine management.
WHY THIS IS TESTED: The exam is built around real clinical judgment. Unsafe options often fail not because they are never done in medicine, but because they are the wrong level of care for a generalist or they skip collaboration and escalation when indicated. For PANRE, your role is not specialist-only operative planning or institution-specific administrative policy. Your role is recognition, initial evidence-based action, monitoring, and timely escalation.
Choose direct outpatient treatment when the condition is common, diagnosis is straightforward, and no red flags are present. Reject outpatient management when the patient is unstable, has a must-not-miss diagnosis, or needs hospital-level intervention. Choose consultation or ED transfer for stroke symptoms, severe sepsis, unstable chest pain, respiratory failure, ectopic pregnancy suspicion with instability, or other high-risk states.
Exam takeaway: Choose routine diagnosis and treatment for common stable conditions, but stabilize and escalate high-acuity or specialist-level problems.
flowchart LR A[Stable common problem] --> B[Evaluate and treat in generalist setting] A2[Uncertain diagnosis but stable] --> C[Order common tests and close follow-up] A3[Red flags or instability] --> D[Stabilize now] D --> E[ED transfer or admission] A4[Specialist-level complexity] --> F[Consult or refer]
See Fig 2 for the exam-safe scope boundary.
B Worked example
A 27-year-old pregnant woman at 10 weeks with nausea, mild lower abdominal pain, and spotting presents to urgent care. She has a history of chlamydia and one prior spontaneous abortion. She is mildly anxious and mentions that she “usually gets cramps with IBS.” Blood pressure is 94/60 mm Hg, pulse 112/min. The stem asks for the most appropriate next step. A tempting-but-wrong clue is her IBS history, which could falsely downplay urgency.
Reasoning chain: Identify task: next best step. Extract key facts: first-trimester bleeding, pain, tachycardia, borderline hypotension, ectopic risk factors. Apply scope rule: this is not routine outpatient reassurance; unstable or potentially unstable early pregnancy bleeding requires urgent evaluation and escalation. Eliminate distractors: outpatient pelvic ultrasound next week is too slow; IBS treatment ignores pregnancy red flags; empiric treatment for cervicitis misses the hemodynamic concern. Verify: urgent ED transfer and ectopic evaluation is the safe PA-level next step.
C Exam trap
D Checkpoint
Question: A 71-year-old man with COPD and coronary artery disease presents with fever, productive cough, and dyspnea. He is confused, blood pressure is 82/48 mm Hg, respiratory rate 30/min, and oxygen saturation 86% on room air. Which is the most appropriate PANRE-level action?
- Start outpatient oral antibiotics and arrange 24-hour follow-up. Tempting because pneumonia is common and treatable, but wrong because shock and hypoxemia require escalation.
- Order chest radiography and wait for results before acting. Tempting because imaging is part of pneumonia evaluation, but wrong because instability requires immediate stabilization and transfer.
- Stabilize airway/breathing/circulation, begin urgent sepsis-directed care, and escalate to ED/hospital management. Tempting and right because the patient is unstable and needs immediate higher-acuity care.
- Schedule pulmonary clinic referral. Tempting because he has COPD, but wrong because chronic disease follow-up is irrelevant to the current emergency.
Best answer: C.
- The first question after reading the last line is: what task type is being tested?
- True or False: If the patient is unstable, the most definitive diagnostic test usually comes before stabilization. False.
- Name the 3 broad action lanes on PANRE: diagnose, evaluate, manage/escalate.
1.1.1.5 Signal words that separate diagnosis, evaluation, management, and monitoring
A Explanation
This section is about language recognition. The decision conflict is similar-looking verbs with different required actions. “Most likely diagnosis,” “best initial test,” “most appropriate next step,” and “most important to monitor” all sound close, but they demand different reasoning. The single rule: tie the stem verb to one clinical output. Diagnosis items want an illness label; evaluation items want a study; management items want an intervention; monitoring items want a follow-up measure or toxicity check.
WHY THIS IS TESTED: PANRE writers often use nearly identical stems but change the last line. That tests whether you can pivot from recognition to the correct clinical task. A learner who ignores the verb may choose a correct idea from the wrong category.
Choose diagnosis language when the stem asks what the patient most likely has or what finding most strongly supports the diagnosis. Choose evaluation language when uncertainty remains and a test will meaningfully narrow decisions. Choose management language when sufficient information already supports treatment or urgent action. Choose monitoring language when therapy is underway and the question asks what adverse effect, lab, or clinical target matters most.
Exam takeaway: Match the verb in the last line to the type of answer the question expects.
flowchart TB
A[Stem signal word] --> B{Category}
B -->|Most likely diagnosis| C[Diagnosis answer]
B -->|Best initial test| D[Evaluation answer]
B -->|Most appropriate next step| E[Management or stabilization answer]
B -->|Most important to monitor| F[Monitoring answer]
B -->|Requires immediate clarification| G[Safety/contraindication answer] See Fig 3 whenever the options feel all “kind of right.”
B Worked example
A 46-year-old woman with obesity, hypertension, and recurrent nephrolithiasis presents with fatigue and constipation. Laboratory studies show calcium 11.6 mg/dL and low phosphorus. The stem could generate several different PANRE questions. If it asks “most likely diagnosis”, you choose primary hyperparathyroidism. If it asks “best initial test to confirm”, you think PTH measurement. If it asks “most important long-term complication to monitor”, you think bone and renal effects. A distracting clue is her constipation, which may tempt treatment-focused thinking before you answer the asked category.
Reasoning chain: Identify task wording. Extract the same key facts each time. Apply the lane rule: same disease pattern, different final answer categories. Eliminate distractors from the wrong category. Verify that your chosen option is the right kind of answer for the verb.
C Exam trap
D Checkpoint
Question: A 62-year-old woman with osteoporosis and hypothyroidism has progressive exertional dyspnea, lower-extremity edema, and elevated jugular venous pressure. If the stem asks, “Which study is the best initial test?” which reasoning path is correct?
- Name the most likely diagnosis first and stop there. Tempting because heart failure is recognizable, but wrong because the question asks for evaluation.
- Choose the study that best establishes the cardiac cause of symptoms. Tempting and right because the stem asks for the best initial test, not treatment.
- Start diuretics immediately regardless of the question. Tempting because treatment may be needed clinically, but wrong here because it ignores the asked task.
- Refer to cardiology without testing. Tempting because subspecialists often manage heart failure, but wrong because the question asks for the best initial study.
Best answer: B.
1.1.1.6 How PANRE builds distractors: noise, near-miss answers, and unsafe sequencing
A Explanation
The decision conflict in many PANRE items is relevant clue versus tempting noise. The single rule that resolves it is: the best answer is driven by the finding that changes management, not by the most vivid detail. Noise can include old diagnoses, incidental lab abnormalities, family history, nonurgent symptoms, or familiar buzzwords. Near-miss distractors are especially dangerous because they would be correct for a slightly different patient.
WHY THIS IS TESTED: Real clinical practice is messy. PANRE mirrors that by giving you extra data and requiring you to prioritize. Examinees often miss questions from premature closure, overvaluing one classic clue while ignoring timing, severity, vital signs, pregnancy, medication risks, or organ-threatening symptoms.
Choose the option that addresses the active problem at the correct time point. Reject answers that are too late, too early, unsafe, or for the wrong severity tier. A definitive test may be wrong if the screening test is enough first. A long-term controller may be wrong if the patient first needs rescue treatment. An outpatient referral may be wrong if the patient needs immediate ED transfer. Distractors often differ by one variable: stability, pregnancy, comorbidity, contraindication, or severity.
Exam takeaway: Mark task, stability, red flags, and the single discriminating clue before comparing answer choices.
See Fig 4 for a visual model of what to extract from a noisy stem.
B Worked example
A 63-year-old man with atrial fibrillation on anticoagulation, chronic kidney disease, and a 40-pack-year smoking history presents with new severe back pain and lightheadedness. He also mentions months of chronic constipation and recent dyspepsia. Blood pressure is 84/52 mm Hg, pulse 122/min. The stem asks for the most appropriate next step. The tempting-but-wrong clue is dyspepsia, which may pull you toward GI causes and acid suppression.
Reasoning chain: Identify task: next step. Extract key facts: severe pain, hypotension, tachycardia, anticoagulation, older age. Apply rule: ignore nondecisive chronic symptoms; prioritize life-threatening instability. Eliminate distractors: outpatient constipation workup and GERD treatment do not fit shock; elective lumbar imaging is too slow; routine analgesics ignore possible hemorrhagic catastrophe. Verify: urgent stabilization and emergency vascular evaluation is the safe action.
C Exam trap
D Checkpoint
Question: A 29-year-old woman with ulcerative colitis and iron deficiency anemia presents with palpitations after starting a decongestant. She also has mild seasonal allergies and chronic fatigue. Heart rate is 164/min and irregular, blood pressure 78/44 mm Hg, and she is diaphoretic. Which principle best answers a PANRE “next step” item?
- Treat the allergies because the medication triggered the symptoms. Tempting because the decongestant is new, but wrong because instability is the decisive issue.
- Focus on the anemia because fatigue explains palpitations. Tempting because iron deficiency can cause tachycardia, but wrong because shock-level vitals demand immediate stabilization.
- Prioritize unstable tachyarrhythmia management over chronic background details. Tempting and right because the acute hemodynamic state determines the next step.
- Order outpatient Holter monitoring first. Tempting because arrhythmia evaluation often uses ambulatory monitoring, but wrong because this patient is unstable now.
Best answer: C.
- The most dangerous distractor is usually the one that would be correct for a slightly different patient.
- True or False: Chronic background symptoms should outweigh shock-level vital signs when choosing the next step. False.
- Name 3 common PANRE discriminators: stability, pregnancy, contraindication.
1.1.1.7 A repeatable exam-day framework: identify task → extract clues → choose action → verify safety
A Explanation
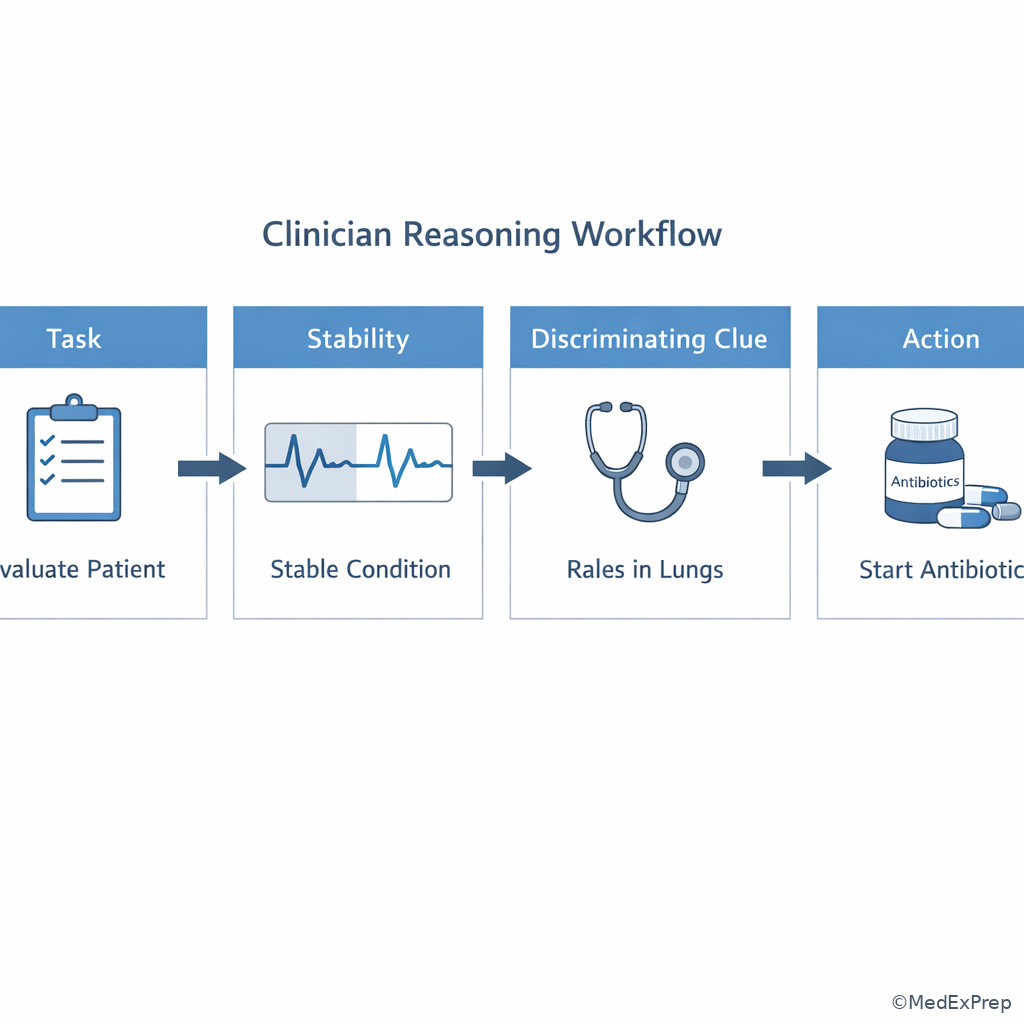
The final foundational skill is synthesis. The decision conflict is fast pattern recognition versus disciplined verification. The single rule is: never stop at recognition; always verify with safety, sequencing, and contraindication checks. The PANRE-friendly framework is: identify the task, extract age/sex/tempo/red flags/discriminating finding, choose the answer category, eliminate options that are unsafe or mistimed, then verify the winner against stability and scope.
WHY THIS IS TESTED: PANRE is not just about naming diseases. It tests whether you can move from recognition to appropriate action under uncertainty. The same framework works across all organ systems and reduces unforced errors. Foundational topics like this matter because later lessons will give disease-specific clues, but the reasoning engine remains the same.
Choose the answer that fits this moment in the case. Reject options that are medically correct in general but wrong in sequence. Monitoring questions require linkage between therapy and risk. Prevention questions require matching age and risk factors. Diagnostic questions require separating classic presentations from close look-alikes. Management may vary somewhat by guideline version or practice setting, but the exam usually favors widely accepted initial actions.
Exam takeaway: Use the same stepwise loop on every item to reduce errors from premature closure and wrong-task answers.
flowchart TD A[Identify task] --> B[Extract age sex tempo red flags] B --> C[Find discriminating clue] C --> D[Choose answer category] D --> E[Eliminate unsafe or mistimed options] E --> F[Verify with stability contraindications follow-up]
See Fig 5 as your default exam loop.
B Worked example
A 52-year-old woman with obesity, hyperlipidemia, and recent long-haul travel presents with pleuritic chest pain and dyspnea. She also has a history of panic attacks and says this “feels similar.” Heart rate is 124/min, oxygen saturation 89% on room air, and she has unilateral calf swelling. The stem asks for the most appropriate next step. A tempting-but-wrong clue is her prior panic history.
Reasoning chain: Identify task: next step. Extract clues: hypoxemia, tachycardia, pleuritic pain, unilateral leg swelling, travel risk. Choose answer lane: immediate evaluation/management of likely pulmonary embolism, not psychiatric diagnosis. Eliminate distractors: reassurance, outpatient anxiolytics, and routine follow-up do not match instability risk. Verify: urgent PE-directed evaluation and escalation are safest.
C Exam trap
D Checkpoint
Question: Which framework best fits a PANRE-style item asking for the most appropriate next step in a patient with possible serious disease?
- Recognize the disease and choose the first familiar option. Tempting because fast pattern recognition feels efficient, but wrong because it skips safety verification.
- Read all options first, then infer what the question must be asking. Tempting because answer choices can hint at the topic, but wrong because it increases anchoring and task confusion.
- Identify task, extract discriminating clues, choose the best category, and verify stability/contraindications. Tempting and right because it matches the repeatable exam-day process.
- Choose the most definitive long-term plan available. Tempting because comprehensive care is good medicine, but wrong because PANRE often asks for the immediate next step, not the whole management plan.
Best answer: C.
Exam Traps & Differentiators
Most common wrong answer and why: The most common miss is a correct clinical idea in the wrong category—for example, naming the diagnosis when the stem asks for the best initial test, or selecting a definitive test when the patient first needs stabilization.
| Looks similar | Actually means | Choose this | Do not choose this |
|---|---|---|---|
| Most likely diagnosis | Disease identification | Illness label supported by key clue | Test or treatment option |
| Best initial test | Evaluation step | Study that changes next action now | Most definitive but unnecessary first study |
| Most appropriate next step | Immediate action | Stabilize/treat/escalate as needed | Long-term plan or delayed workup |
| Most important to monitor | Follow-up or adverse effect surveillance | Marker linked to response or toxicity | Incidental lab not tied to the intervention |
| Requires immediate clarification | Safety screening | Contraindication, interaction, pregnancy issue | Minor optimization detail |
| If the stem says... | Think... | Reason |
|---|---|---|
| Hypotension, altered mental status, hypoxemia, severe pain, or active bleeding | Stabilize before definitive workup | Acuity outranks completeness |
| Most likely diagnosis | Pattern recognition with one discriminating clue | The answer must be a disease label |
| Best initial therapy | First-line treatment matched to severity | Do not jump to rescue or second-line therapy without a trigger |
| Requires immediate clarification | Medication safety, pregnancy, interaction, allergy, contraindication | These items are safety-first questions |
| History of a benign look-alike disorder | Do not anchor if new red flags are present | Prior diagnoses often function as distractors |
| Close-call options all seem reasonable | Find the one variable that changes the answer | Most PANRE distractors are right for a slightly different patient |
Exam takeaway: Distinguish diagnosis, testing, treatment, monitoring, and disposition as separate answer lanes.
Exam takeaway: Unstable vital signs change the answer from routine workup to immediate stabilization and escalation.
Looks similar but isn’t: Later in the course, you will see clinically similar traps such as panic attack vs pulmonary embolism, GERD vs acute coronary syndrome, migraine vs subarachnoid hemorrhage, and uncomplicated cystitis vs pyelonephritis. The same exam strategy applies: one clue changes the category or urgency. This is the bridge to the upcoming lessons on stem signal extraction and next-best-step logic.
Tables
| Reference summary | High-yield rule | Why it matters on PANRE |
|---|---|---|
| Read the last line first | Identify task before details | Prevents answering the wrong category |
| Assess stability early | ABC and red flags outrank routine workup | Catches emergency “next step” items |
| Use one discriminating clue | Find the fact that separates the top two options | Reduces premature closure |
| Match answer type to verb | Diagnosis vs test vs treatment vs monitoring | Stops correct-but-not-asked errors |
| Check contraindications | Pregnancy, drug interaction, organ failure, allergy | Common safety-based distractor pattern |
| Think in sequence | Best next step is often not the definitive final step | Prevents over-advancing care plans |
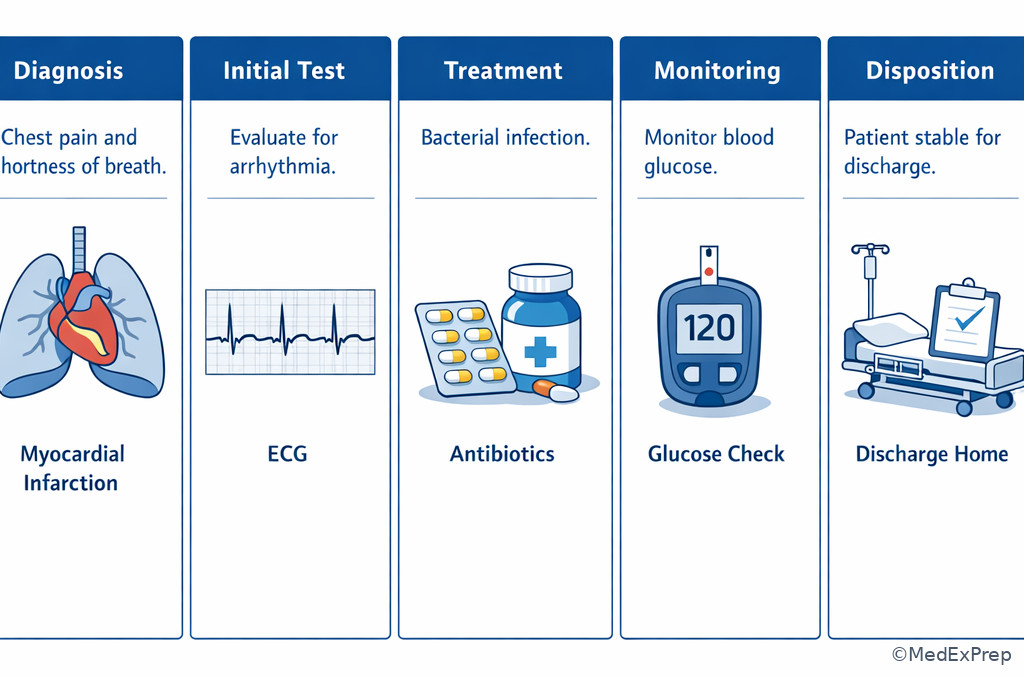
| Comparison | Diagnosis item | Evaluation item | Management item |
|---|---|---|---|
| What answer looks like | Disease name | Lab, imaging, ECG, or procedure | Medication, stabilization, referral, admission, counseling |
| Key thinking move | Pattern match | Choose study that changes action | Choose safest immediate action |
| Best discriminator | One defining finding | Pretest probability and urgency | Stability, severity, contraindications |
| Classic error | Picking a treatment | Jumping to a definitive but mistimed test | Skipping stabilization or choosing delayed care |
| Example wording | Most likely diagnosis | Best initial test | Most appropriate next step |
| Differential classification of wrong answers | What makes them tempting | Single clue that rules them out |
|---|---|---|
| Correct disease, wrong task | You recognized the illness script | The stem asks for a test or treatment instead |
| Correct test, wrong sequence | The test is truly useful | The patient is unstable or a simpler first test is required |
| Correct treatment, wrong severity tier | The drug is used for that disease | The patient needs milder or more urgent therapy instead |
| Correct plan for a different population | Guideline memory is partly right | Pregnancy, age, kidney disease, or allergy changes the choice |
| Correct outpatient plan, wrong disposition | The condition can be managed outpatient when stable | Red-flag vitals or organ threat require ED/hospital care |
| Attractive noise-based answer | It fits a familiar but nondecisive symptom | An acute objective finding outweighs the background detail |
Algorithm / Approach
Exam takeaway: Use a fixed sequence—task, stability, clue, category, safety—to choose the best answer reliably.
Keep this algorithm visible during practice. See Fig 6.
Exam takeaway: Organize every vignette into task, stability, key clue, and action to avoid distractor-driven errors.
Exam takeaway: Contraindications, pregnancy, allergy, and organ dysfunction frequently convert a plausible answer into the wrong one.
Rapid Review
- Task wording → last line determines answer category
- Most likely diagnosis → choose disease label, not test or treatment
- Best initial test → choose study that changes immediate management
- Most appropriate next step → stability check comes before diagnostic elegance
- Unstable patient → stabilize/escalate before comprehensive workup
- Near-miss distractor → usually right for a slightly different patient
- Clinical noise → background details do not outrank red flags
- Monitoring question → link therapy to toxicity or response marker
- Safety question → think contraindication, pregnancy, interaction, allergy
- Generalist PA framing → routine care directly, dangerous complexity escalated
- Premature closure → disease recognition without verify step
- Best answer → correct for this exact patient at this exact moment
Self-check quiz
1. A 41-year-old woman with hypothyroidism and seasonal allergies presents with 2 days of dysuria and urinary frequency. She has no fever, flank pain, or vomiting. The stem asks, “Which of the following is the most likely diagnosis?” Which answer category should you choose?
- Antibiotic treatment option
- Urinalysis test
- Disease label
- Disposition plan
2. A 67-year-old man with coronary artery disease and diabetes presents with crushing chest pain, diaphoresis, blood pressure 82/50 mm Hg, and oxygen saturation 88%. The stem asks for the “most appropriate next step.” Which principle most strongly controls the answer?
- Choose the most definitive outpatient test
- Stabilization outranks complete diagnostic workup
- Long-term secondary prevention is the immediate priority
- Chronic risk factor modification comes before acute care
3. A 29-year-old woman with asthma and obesity presents with recurrent wheezing and nighttime cough. She is speaking in full sentences, pulse oximetry is 98%, and exam shows mild expiratory wheezes. She asks whether she needs “a scan of the lungs.” The stem asks for the best initial therapy. Which is most appropriate?
- Choose the controller or reliever medication strategy that fits current severity
- Order chest CT because dyspnea always requires imaging
- Provide only reassurance because oxygen saturation is normal
- Refer to thoracic surgery for evaluation
4. A 56-year-old man with hypertension, CKD, and recent NSAID use presents with rising creatinine and decreased urine output. He is hemodynamically stable. The stem asks for the best initial test. Which reasoning path is correct?
- Pick the diagnosis that seems most likely and ignore the ask
- Choose the study or lab that best clarifies the cause of AKI at this stage
- Start dialysis because kidney injury is present
- Arrange renal transplant consultation
5. A 24-year-old pregnant woman with type 1 diabetes presents with vomiting and abdominal pain. She has missed insulin doses and appears dehydrated. The stem asks which medication order requires immediate clarification. Which lens should you apply first?
- Cost and convenience
- Pregnancy status, contraindications, and safety
- Long-term preventive counseling
- Most definitive endocrinology referral plan
6. A 63-year-old man with GERD, hypertension, and tobacco use presents with epigastric burning and chest pressure after dinner. He says antacids helped a little. Blood pressure is 84/58 mm Hg, heart rate 118/min, and he is diaphoretic. The stem asks for the most appropriate next step. Which option is best?
- Empiric acid suppression and outpatient follow-up
- Exercise stress testing later this week
- Immediate stabilization and emergency ACS-directed evaluation
- Routine GI referral for endoscopy
7. A 35-year-old woman with migraine history, oral contraceptive use, and recent prolonged travel presents with pleuritic chest pain and anxiety. She says it “feels like a panic attack.” Heart rate is 122/min, oxygen saturation 90%, and the left calf is swollen. The stem asks for the most likely diagnosis. Which choice best fits the task and clue pattern?
- Panic attack
- Gastroesophageal reflux disease
- Pulmonary embolism
- Costochondritis
8. A 72-year-old woman with heart failure, chronic atrial fibrillation, and CKD is started on a new medication for rate control. Two weeks later she reports nausea, decreased appetite, and yellow visual halos. The stem asks for the most important parameter to monitor. Which reasoning rule best applies?
- Choose a disease label because symptoms define the illness
- Choose the toxicity or response measure linked to the medication in question
- Choose the broadest preventive screening test available
- Choose a specialist referral because adverse effects always require consultation
Answer key
1.1.1.8 1. Question 1
Correct answer: C. Disease label. The pathophysiology here is not the focus; the exam skill is task classification. The stem asks for the most likely diagnosis, so the correct answer category is the disease name rather than a test, treatment, or disposition. Authoritative exam-style clinical reasoning frameworks consistently stress aligning the answer to the question task before moving to management. Sources: AAPA review frameworks; Harrison’s Principles of Internal Medicine.
- A. Antibiotic treatment option: Tempting because dysuria/frequency suggests uncomplicated cystitis and treatment may be obvious. Incorrect because the stem asks for diagnosis, not therapy. Discriminating clue: “Most likely diagnosis.”
- B. Urinalysis test: Tempting because urinalysis is a common evaluation step for urinary symptoms. Incorrect because the question asks for the illness label rather than a study. Discriminating clue: verb category mismatch.
- C. Disease label: Tempting and correct because the final line explicitly asks what the patient most likely has. Discriminating clue: direct diagnosis wording.
- D. Disposition plan: Tempting because disposition is always part of care. Incorrect because nothing in the stem asks where the patient should go next. Discriminating clue: no disposition wording or red flags.
1.1.1.9 2. Question 2
Correct answer: B. Stabilization outranks complete diagnostic workup. Hypotension, hypoxemia, and active ischemic symptoms indicate an unstable patient. Mechanism-to-treatment logic: instability suggests immediate threat to perfusion and oxygen delivery, so emergency stabilization and acute management precede elective diagnostic completeness. This aligns with AHA/ACC acute coronary syndrome principles and general emergency triage practice. Sources: AHA/ACC chest pain and ACS guidance; Harrison’s Principles of Internal Medicine.
- A. Choose the most definitive outpatient test: Tempting because testing clarifies diagnosis. Incorrect because unstable chest pain is not an outpatient scenario. Discriminating clue: blood pressure 82/50 mm Hg and oxygen saturation 88%.
- B. Stabilization outranks complete diagnostic workup: Tempting and correct because shock physiology makes immediate supportive and emergent management the priority. Discriminating clue: hypotension with ischemic symptoms.
- C. Long-term secondary prevention is the immediate priority: Tempting because CAD management includes long-term prevention. Incorrect because acute instability comes first. Discriminating clue: active severe presentation, not post-stabilization care.
- D. Chronic risk factor modification comes before acute care: Tempting because diabetes/CAD raise long-term risk. Incorrect because preventive counseling never outranks hemodynamic instability. Discriminating clue: current shock and hypoxemia.
1.1.1.10 3. Question 3
Correct answer: A. Choose the controller or reliever medication strategy that fits current severity. Mild stable asthma symptoms with normal oxygenation and no severe distress fit outpatient medical management rather than advanced imaging or referral. The key mechanism is severity-based treatment: management questions require selecting therapy proportional to present symptom burden. Sources: GINA guidance; Harrison’s Principles of Internal Medicine.
- A. Choose the controller or reliever medication strategy that fits current severity: Tempting and correct because the stem asks for best initial therapy, and the patient appears stable with mild symptoms. Discriminating clue: normal oxygen saturation and ability to speak full sentences.
- B. Order chest CT because dyspnea always requires imaging: Tempting because imaging can exclude other pathology. Incorrect because there is no red flag suggesting need for CT as the first step in mild recurrent asthma symptoms. Discriminating clue: stable asthma-pattern presentation.
- C. Provide only reassurance because oxygen saturation is normal: Tempting because she is not in severe distress. Incorrect because symptoms still warrant appropriate therapy, not dismissal. Discriminating clue: recurrent wheezing and nighttime cough.
- D. Refer to thoracic surgery for evaluation: Tempting only if one overreacts to dyspnea. Incorrect because this is outside the clinical problem and far beyond the needed initial step. Discriminating clue: common outpatient airway disease pattern.
1.1.1.11 4. Question 4
Correct answer: B. Choose the study or lab that best clarifies the cause of AKI at this stage. The mechanism-based logic is that stable acute kidney injury requires targeted initial evaluation to distinguish prerenal, intrinsic, or postrenal patterns before jumping to advanced interventions. PANRE-style test questions ask for the study that changes immediate clinical reasoning. Sources: KDIGO principles; Harrison’s Principles of Internal Medicine.
- A. Pick the diagnosis that seems most likely and ignore the ask: Tempting because NSAID-related AKI is familiar. Incorrect because the stem asks for the best initial test, not the diagnosis. Discriminating clue: explicit evaluation wording.
- B. Choose the study or lab that best clarifies the cause of AKI at this stage: Tempting and correct because stable AKI should be evaluated in a stepwise fashion. Discriminating clue: hemodynamically stable patient with question asking for testing.
- C. Start dialysis because kidney injury is present: Tempting because AKI can become severe. Incorrect because no emergent dialysis indication is described. Discriminating clue: absence of life-threatening complications.
- D. Arrange renal transplant consultation: Tempting only if one confuses acute with end-stage disease. Incorrect because this is not the initial evaluation step. Discriminating clue: early AKI scenario.
1.1.1.12 5. Question 5
Correct answer: B. Pregnancy status, contraindications, and safety. “Requires immediate clarification” is a medication-safety question. The mechanism is not disease confirmation but prevention of harm from contraindicated or inappropriate orders, especially in pregnancy and acute metabolic illness. Sources: standard pharmacology safety principles; ACOG and ADA-aligned pregnancy care principles.
- A. Cost and convenience: Tempting in outpatient care because adherence matters. Incorrect because safety outranks convenience in clarification items. Discriminating clue: wording “requires immediate clarification.”
- B. Pregnancy status, contraindications, and safety: Tempting and correct because pregnant patients with acute illness require extra medication safety screening. Discriminating clue: pregnancy plus urgent medication clarification framing.
- C. Long-term preventive counseling: Tempting because diabetes always requires counseling. Incorrect because the question is about immediate order safety. Discriminating clue: acute presentation and immediate clarification wording.
- D. Most definitive endocrinology referral plan: Tempting because type 1 diabetes in pregnancy is complex. Incorrect because referral does not answer which order is unsafe now. Discriminating clue: medication clarification is the explicit task.
1.1.1.13 6. Question 6
Correct answer: C. Immediate stabilization and emergency ACS-directed evaluation. Although GERD symptoms and partial antacid response are tempting, hypotension, diaphoresis, and chest pressure indicate possible acute coronary syndrome with instability. Mechanism-to-treatment logic: reduced coronary perfusion and shock physiology make emergency management the correct next step. Sources: AHA/ACC chest pain guidance; Harrison’s Principles of Internal Medicine.
- A. Empiric acid suppression and outpatient follow-up: Tempting because epigastric burning after dinner resembles reflux. Incorrect because unstable vital signs and diaphoresis are red flags against a benign GI-only explanation. Discriminating clue: blood pressure 84/58 mm Hg.
- B. Exercise stress testing later this week: Tempting because stress testing evaluates ischemia in stable patients. Incorrect because it is unsafe and mistimed in an unstable current event. Discriminating clue: active chest pressure with hypotension.
- C. Immediate stabilization and emergency ACS-directed evaluation: Tempting and correct because the patient’s acute physiology requires urgent management now. Discriminating clue: diaphoresis and hypotension in a high-risk chest pain presentation.
- D. Routine GI referral for endoscopy: Tempting if one anchors on GERD history. Incorrect because it ignores a possible life-threatening cardiac event. Discriminating clue: hemodynamic instability.
1.1.1.14 7. Question 7
Correct answer: C. Pulmonary embolism. The mechanism is venous thromboembolism causing pleuritic pain, tachycardia, hypoxemia, and unilateral leg swelling. Panic attack is a classic distractor because anxiety and chest symptoms overlap, but objective VTE clues shift the diagnosis. Sources: CHEST/PE diagnostic frameworks; Harrison’s Principles of Internal Medicine.
- A. Panic attack: Tempting because the patient feels anxious and reports similarity to prior episodes. Incorrect because panic does not explain unilateral calf swelling and hypoxemia as well as PE does. Discriminating clue: swollen calf with oxygen saturation 90%.
- B. Gastroesophageal reflux disease: Tempting because chest pain may be noncardiac. Incorrect because pleuritic pain and VTE risk factors do not fit GERD. Discriminating clue: pleuritic chest pain after prolonged travel.
- C. Pulmonary embolism: Tempting and correct because oral contraceptive use, travel, tachycardia, hypoxemia, and calf swelling form a classic pattern. Discriminating clue: unilateral calf swelling with low oxygen saturation.
- D. Costochondritis: Tempting because pleuritic-sounding pain can be musculoskeletal. Incorrect because costochondritis does not explain hypoxemia or DVT features. Discriminating clue: objective thromboembolic signs.
1.1.1.15 8. Question 8
Correct answer: B. Choose the toxicity or response measure linked to the medication in question. The symptom cluster suggests medication toxicity, classically digoxin-like. Monitoring questions require linking the treatment to its toxicity profile and relevant lab/clinical surveillance rather than re-solving the whole differential from scratch. Sources: standard cardiovascular pharmacology references; Harrison’s Principles of Internal Medicine.
- A. Choose a disease label because symptoms define the illness: Tempting because the symptom cluster is recognizable. Incorrect because the stem asks what to monitor, not what the diagnosis is. Discriminating clue: “most important parameter to monitor.”
- B. Choose the toxicity or response measure linked to the medication in question: Tempting and correct because monitoring items are therapy-linked by design. Discriminating clue: new rate-control medication followed by toxicity symptoms.
- C. Choose the broadest preventive screening test available: Tempting because older adults need preventive care. Incorrect because screening is unrelated to medication monitoring in this scenario. Discriminating clue: temporal relation to starting a new drug.
- D. Choose a specialist referral because adverse effects always require consultation: Tempting because CKD increases medication risk. Incorrect because the question asks for the most important parameter to monitor, not the referral pathway. Discriminating clue: monitoring-focused wording.