Why it matters
- Wrong-patient radiopharmaceutical administration is both a patient-safety event and a radiation-safety event.
- Many NMTCB questions hide the true issue inside workflow noise; the right answer is often to stop and re-identify the patient before proceeding.
- Identity verification anchors every later screening step, including pregnancy status, allergy review, consent support, dose documentation, and image labeling.
- In nuclear medicine, once the dose is administered, the error cannot simply be “taken back,” so verification must happen before injection, imaging, and release of labeled data.
Key Terms & Must-Know Facts
1.1.1.1 Key terms
- Two-identifier rule: Use at least two accepted patient identifiers before care.
- Accepted identifier: Commonly name, date of birth, medical record number, or another institution-approved unique identifier.
- Unaccepted identifier: Room number, physical appearance, diagnosis, or “the patient with the bone scan.”
- Order reconciliation: Matching patient, procedure, indication, and schedule before proceeding.
- Time-out: A brief pause to confirm the right patient and right procedure before a critical step.
- Verbal confirmation: Patient states identifiers when able; staff should not lead with the answer.
- Armband verification: Comparing the wristband to the order and verbal response.
- Proxy verification: Using caregiver, chart, armband, and team confirmation when the patient cannot speak.
- Discrepancy: Any mismatch between patient statement, armband, order, schedule, or documentation.
- Escalation: Stop the workflow and notify the authorized provider/supervisor when identity cannot be confirmed.
- Near miss: An error caught before the dose is administered or imaging proceeds.
- Wrong-patient event: Care delivered to the wrong individual.
- Chain of custody for dose: Traceable association between the prepared dose and the intended patient/procedure.
1.1.1.2 Must-know facts
- Identity verification must occur before administration and again when workflow risk increases.
- Ask the patient to state identifiers; do not convert the check into a yes/no guessing game.
- Room number is never a sufficient identifier.
- If the patient cannot self-identify, use institution-approved alternate verification and escalate uncertainty.
- The technologist may verify and screen; changing the ordered radiopharmaceutical without authorization is out of scope.
- A matching armband alone is not enough if another part of the workflow conflicts.
- Similar names require deliberate pause-and-compare action.
- Documentation must reflect what was verified and what discrepancy action was taken.
Exam takeaway: Use a two-identifier plus order-match workflow before any dose leaves the safe path.
flowchart TD
A[Patient arrives] --> B[Ask patient to state full name and DOB]
B --> C[Check armband or approved record]
C --> D[Match order, procedure, schedule, and patient]
D --> E{Any mismatch?}
E -- No --> F[Proceed to next safety screen]
E -- Yes --> G[Stop workflow]
G --> H[Resolve discrepancy and document]
H --> I[Escalate if unresolved] Exam takeaway: Reject convenience identifiers even when the workflow feels routine.
flowchart LR A[Strong identifiers] --> A1[Full name] A --> A2[Date of birth] A --> A3[Medical record number] B[Weak identifiers] --> B1[Room number] B --> B2[Diagnosis] B --> B3[Physical appearance] B --> B4[Procedure nickname]
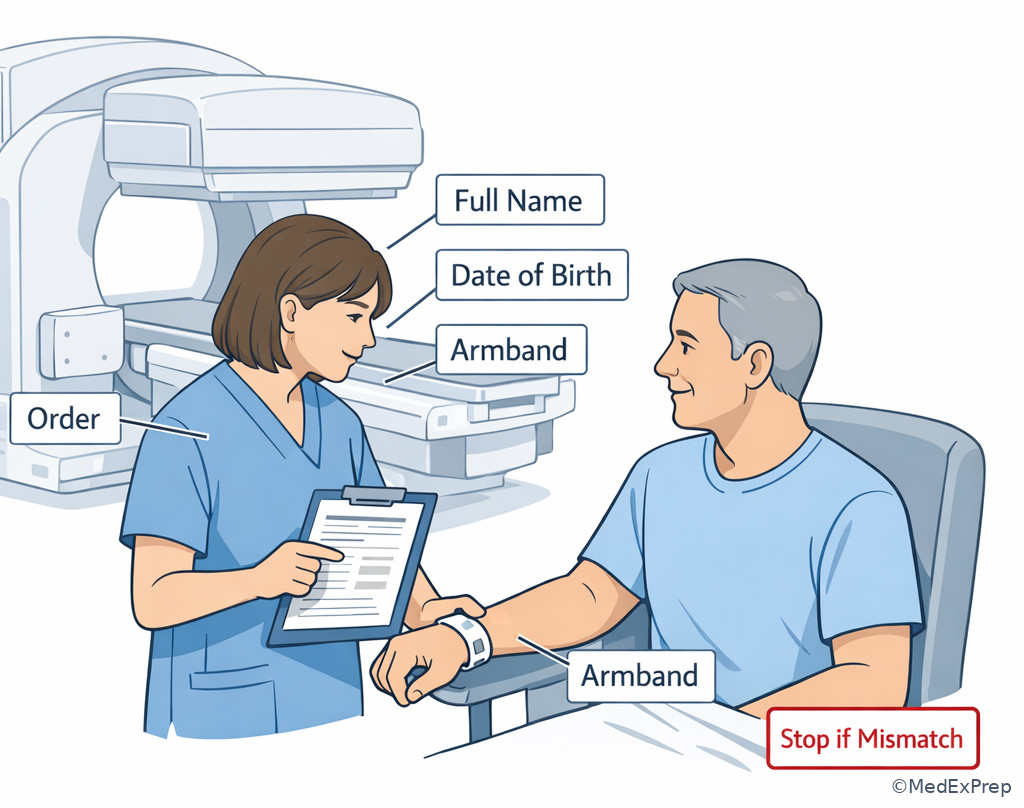
Exam takeaway: Visualize the verbal-plus-armband check before dose preparation and administration.
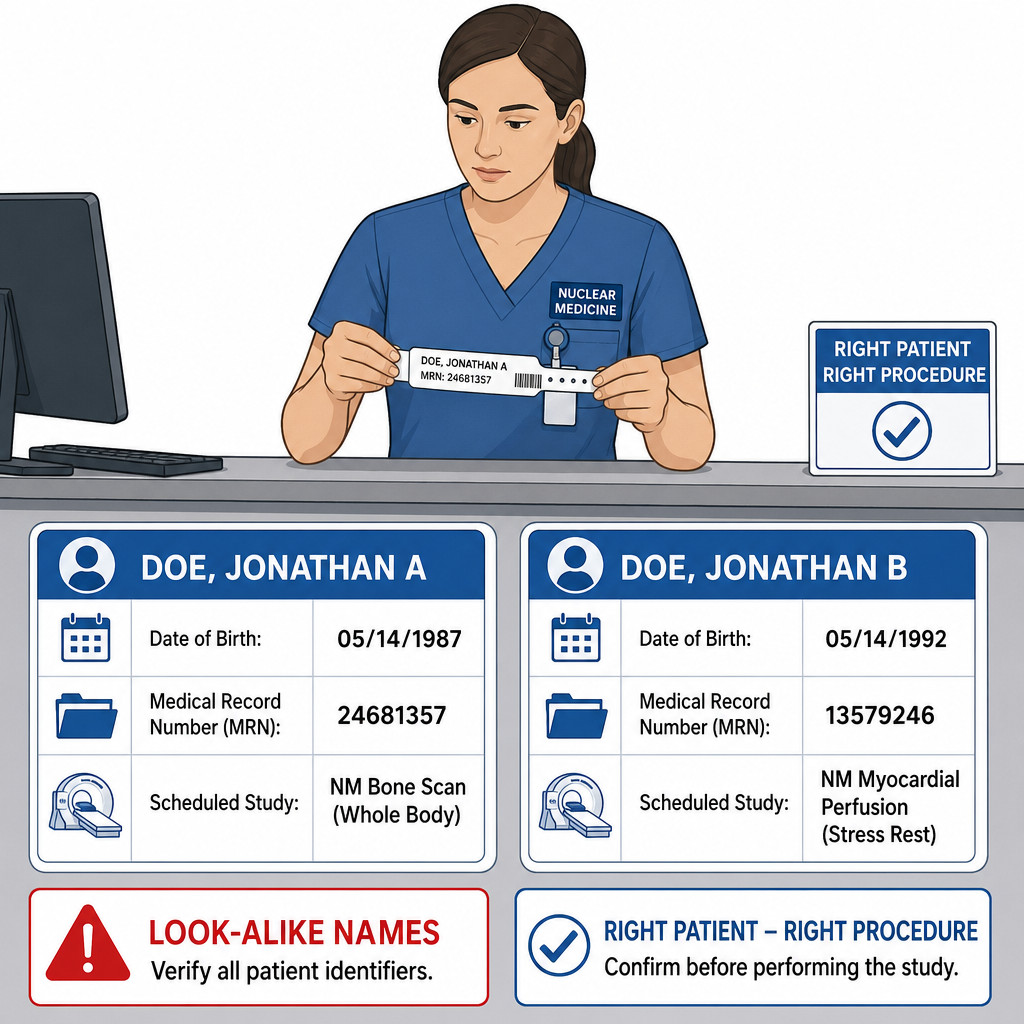
Exam takeaway: Similar names should trigger a deliberate pause, not a faster guess.
Core content
1.1.1.3 Foundations: what counts as correct patient identification
A Explanation
The decision conflict here is simple but highly testable: Do you proceed because the patient appears to fit the appointment, or do you require formal identity confirmation first? The rule that resolves it is the two-identifier standard plus procedure match. In practice, the technologist should ask the patient to state identifiers such as full name and date of birth, then compare those to the armband and the order. The workflow is not complete until the patient, procedure, and documentation all align. See Fig 1.
WHY THIS IS TESTED: Exam stems often include a familiar patient, a busy schedule, or a confident family member to tempt you into accepting a shortcut. The tested pattern is whether you can distinguish a true identifier from a convenience cue. A room number, diagnosis, age estimate, or staff recognition is not enough. See Fig 2.
Choose verbal confirmation when the patient is alert and able. Reject yes/no prompting such as, “Are you Mrs. Smith?” because it can produce false agreement. Choose direct questioning: “Please tell me your full name and date of birth.” When a patient is unable to answer, the single finding that changes the workflow is loss of reliable self-identification. At that point, use institution-approved alternatives: wristband, chart, caregiver or legal representative, and staff cross-checks, then escalate if uncertainty remains.
Key rule: The strongest routine verification pattern is patient-stated identifiers plus independent document match plus correct scheduled procedure.
Recall: This is the first topic in the course, so it sets the base layer for all later screening. In the upcoming topic on Pregnancy And Breastfeeding Screening, identity must already be confirmed before you ask exposure-sensitive questions.
B Worked example
A 67-year-old outpatient arrives for a scheduled bone scan. He has diabetes, chronic kidney disease, and hearing loss. The schedule shows “Robert J. Martin,” and the waiting room clipboard says “Bob Martin.” His armband from a same-day lab visit reads “Robert Martin.” A transporter says, “That’s the bone scan patient from room 12.” The patient nods when asked, “Are you Mr. Martin?” The most appropriate next step is to stop the yes/no approach and obtain active verbal confirmation using full name and date of birth, then compare those to the order and armband before any dose-related action.
Reasoning chain: Identify the task: right-patient verification before procedure workflow. Extract key facts: similar naming forms, hearing impairment, transporter using room number, and the patient only nodding to a leading question. Apply the rule: two accepted identifiers must be actively confirmed, not guessed. Eliminate distractors: room number is weak; a nod to a suggested name is unsafe; a partially matching armband does not settle identity without verbal or approved alternate confirmation. Verify: if full identifiers and procedure match, proceed; if not, resolve discrepancy and document.
C Exam trap
Common wrong answer: Proceed because the wristband and schedule are “close enough.”
Why it is tempting: In real workflow, partial matches plus staff familiarity feel efficient, especially when the patient appears cooperative.
Single clue that eliminates it: The patient was identified with a leading yes/no prompt rather than stating identifiers independently.
D Checkpoint
Question: A technologist brings an alert patient into the injection room for a thyroid uptake study. Which action is the most appropriate identity verification step before proceeding?
- A. Ask, “Are you here for the thyroid test?”
- B. Match the room number on the schedule to the patient in the chair.
- C. Ask the patient to state full name and date of birth, then compare with the order and armband.
- D. Accept the transporter’s confirmation because the patient came from the correct clinic.
Answer: C
- A: Tempting because it sounds like confirmation, but it checks the procedure nickname rather than identity and uses a leading prompt.
- B: Tempting because room assignment seems concrete, but room number is not an accepted unique identifier.
- C: Correct because it uses patient-stated identifiers plus independent source comparison.
- D: Tempting because transport staff often know the destination, but destination is not proof of right patient.
If you missed this: Review 1.1.1.1 Foundations: what counts as correct patient identification — focus on the difference between accepted identifiers and convenience cues.
Practitioner Action: Assess whether the patient can self-identify reliably. Intervene by using two approved identifiers and procedure match before continuing. Refer unresolved mismatches to the supervising technologist, nurse, or authorized provider per protocol. Document what identifiers were used and any discrepancy resolution.
1.1.1.4 Applied verification: matching the patient to the right order and procedure
A Explanation
The next decision conflict is Should you treat identity verification as separate from order review, or must they be reconciled together? On the NMTCB exam, the correct approach is integrated. Right patient and right procedure are linked safety checks. A patient may correctly identify themselves and still have the wrong study queued, the wrong protocol selected, or a dose prepared for a similarly named patient. The single rule that resolves this is: do not proceed until patient identifiers, ordered study, indication, and scheduled workflow all agree.
This is especially important in nuclear medicine because doses may be patient-specific by timing, activity, or preparation. A mismatch can lead to wrong-patient administration, wrong-procedure imaging, or mislabeled image data. See Fig 1. The testable pattern is often a stem where the patient says, “I’m here for my heart test,” but the order is for a bone scan, or where two outpatients have similar names on the same morning list. The correct technologist move is not to reinterpret the order independently; it is to stop and reconcile with protocol and the authorized team.
Key rule: Correct identity does not rescue an incorrect order match. You need the right patient and the right procedure.
High-Yield Connection: This concept is tested alongside Procedure Documentation Essentials and later with Administration Routes And Verification. Know both patient-order matching and dose-route matching for exam day; they are frequently paired in stems.
B Worked example
A 58-year-old woman with breast cancer history and chronic back pain arrives for “the scan my doctor ordered.” She also has hypertension and anxiety. Her chart has a valid name and date of birth match. The electronic order lists a whole-body bone scan, but she says her oncologist told her she was getting a cardiac stress test because of chest tightness. A recent troponin in the chart is normal, which is distracting but not determinative here. The most appropriate technologist action is to stop and reconcile the discrepancy with the ordering team or supervising provider before preparation or administration.
Reasoning chain: Identify the task: reconcile patient identity with the correct intended procedure. Extract key facts: identity itself matches, but the expected exam and order do not. Apply the rule: right patient plus right study must both be confirmed; the technologist cannot independently decide which order is intended. Eliminate distractors: normal troponin does not authorize changing the study; history of cancer does not automatically prove the bone scan is correct today; anxiety does not explain away a procedure mismatch. Verify: only once the order discrepancy is resolved should workflow resume.
C Exam trap
Common wrong answer: Continue with the ordered study because the patient was correctly identified.
Why it is tempting: Learners may separate identity and order into two unrelated tasks and think the order alone controls workflow.
Single clue that eliminates it: The patient’s understanding of the intended study conflicts with the documented order, creating an unresolved right-procedure problem.
D Checkpoint
Question: A patient correctly states name and date of birth. The order is for a ventilation-perfusion study, but the patient says, “I’m here for my gastric emptying test.” What is the most appropriate next step?
- A. Proceed with the ventilation-perfusion study because the electronic order is present.
- B. Continue intake and plan to clarify after radiopharmaceutical administration.
- C. Stop and reconcile the discrepancy before any dose preparation or administration.
- D. Ask the patient which test they would prefer and update the workflow accordingly.
Answer: C
- A: Tempting because the order appears official, but unresolved study mismatch makes proceeding unsafe.
- B: Tempting because it seems efficient, but once administration occurs the error risk becomes larger and potentially irreversible.
- C: Correct because right patient alone is not sufficient when the right procedure is uncertain.
- D: Tempting because the patient supplies useful information, but selecting the study is not the technologist’s independent decision.
If you missed this: Review 1.1.1.2 Applied verification: matching the patient to the right order and procedure — focus on the rule that identity verification and order reconciliation must both be satisfied.
- The most dangerous shortcut after a correct name/DOB match is skipping the procedure match.
- True or False: A valid order always overrides patient-reported mismatch. False.
- Name the 3 linked checks before proceeding: right patient, right procedure, right documentation.
Memory anchor: Think ID-PRO-DOC = IDentity, PROcedure, DOCuments. If one fails, the workflow fails.
Practitioner Action: Assess whether the order, schedule, and patient expectation align. Intervene by pausing the workflow when any mismatch appears. Refer unresolved order questions to the authorized provider or supervising team. Document the discrepancy, who was notified, and the disposition.
Exam takeaway: The safest checkpoint is before dose preparation, before administration, and before image labeling.
flowchart TB A[Schedule review] --> B[Patient arrives] B --> C[Identity confirmation] C --> D[Order and procedure match] D --> E[Dose prepared for correct patient] E --> F[Pre-administration pause] F --> G[Acquisition and image label check]
Exam takeaway: Match the patient, order, and intended study before the dose workflow advances.
1.1.1.5 Special situations: patients who cannot reliably self-identify
A Explanation
The decision conflict here is Do you lower the standard because the patient cannot answer, or do you change the method while keeping the standard? The correct move is to change the method, not the standard. Inpatients who are sedated, confused, intubated, cognitively impaired, pediatric, aphasic, or hard of hearing may not provide reliable verbal identification. The single finding that changes your process is inability to provide dependable self-identification. That does not permit guessing. It requires institution-approved alternate verification and, if uncertainty remains, escalation before proceeding.
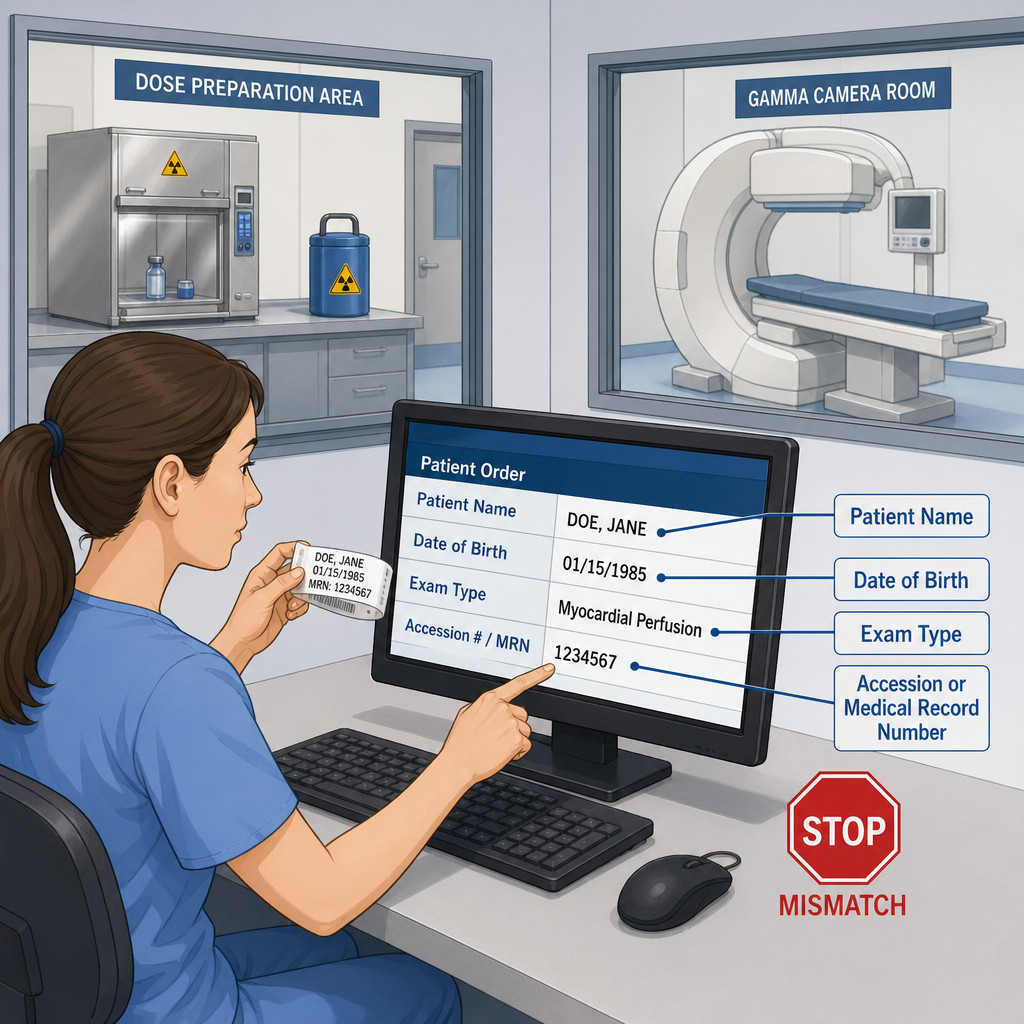
Typical alternate checks include the armband, electronic record, requisition, caregiver or legal representative input, transport documentation, and staff handoff verification. The exam often tests whether you can avoid overtrusting one source. An armband may be incorrect; a family member may be mistaken; transport paperwork may follow the wrong patient. The safe answer is a multi-source match, not a single-source assumption. See Fig 3.
Key rule: When the patient cannot self-identify, increase redundancy. The inability to answer is a reason to strengthen verification, not bypass it.
High-Yield Connection: This concept overlaps with Patient Positioning And Comfort and Vital Signs And Distress Response. Patients who are unstable or impaired may also be poor historians, so safety checks must shift toward team-based verification.
B Worked example
An 81-year-old inpatient is brought for a hepatobiliary scan. He has dementia, atrial fibrillation, and recent opioid analgesia after a fall. He is drowsy and says a different first name than the chart. His wristband matches the requisition, and his daughter at bedside confirms his full name and date of birth. The transporter insists he is the correct patient because he came from the right unit. A low hemoglobin in the chart is distracting but unrelated to the identity task. The most appropriate next step is to verify using the wristband, chart, and caregiver confirmation per protocol, then proceed only if all approved sources agree; if the verbal inconsistency remains unexplained or any source conflicts, stop and escalate.
Reasoning chain: Identify the task: determine whether alternate verification is sufficient. Extract key facts: unreliable self-report due to cognitive impairment and sedation; armband and requisition match; caregiver confirmation supports identity; transporter statement is weak. Apply the rule: strengthen verification using approved alternate sources. Eliminate distractors: the transporter’s confidence is not enough; the patient’s incorrect self-report alone does not automatically prove a mismatch when cognition is impaired; the hemoglobin does not resolve identity. Verify: document why alternate identification was used.
C Exam trap
Common wrong answer: Cancel or delay automatically because the patient cannot state name and date of birth.
Why it is tempting: Learners may overcorrect and think verbal confirmation is the only acceptable method.
Single clue that eliminates it: The patient is not a reliable historian, so institution-approved alternate verification methods become the proper pathway.
D Checkpoint
Question: A nonverbal pediatric patient arrives for a renal scan with a parent. Which approach is most appropriate?
- A. Use the parent’s statement alone because the child cannot speak.
- B. Verify the armband, compare with the order, confirm with the parent, and follow pediatric protocol documentation.
- C. Skip identity verification because the patient is a minor accompanied by a guardian.
- D. Ask the child to nod yes when you say the name printed on the order.
Answer: B
- A: Tempting because the parent is a key source, but one source alone is weaker than multi-source verification.
- B: Correct because it uses alternate approved verification while maintaining redundancy.
- C: Tempting only if someone confuses guardianship with identity proof, but minors still require formal verification.
- D: Tempting because it attempts participation, but nodding to a suggested answer is unreliable.
If you missed this: Review 1.1.1.3 Special situations: patients who cannot reliably self-identify — focus on when to switch from verbal confirmation to multi-source alternate verification.
Practitioner Action: Assess cognition, hearing, language, and consciousness to determine whether self-identification is reliable. Intervene with alternate approved verification methods when needed. Refer unresolved uncertainty to the supervising physician, nurse, or department lead per protocol. Document the reason verbal identification could not be used and the sources that confirmed identity.
1.1.1.6 High-risk moments: before dose preparation, administration, and imaging
A Explanation
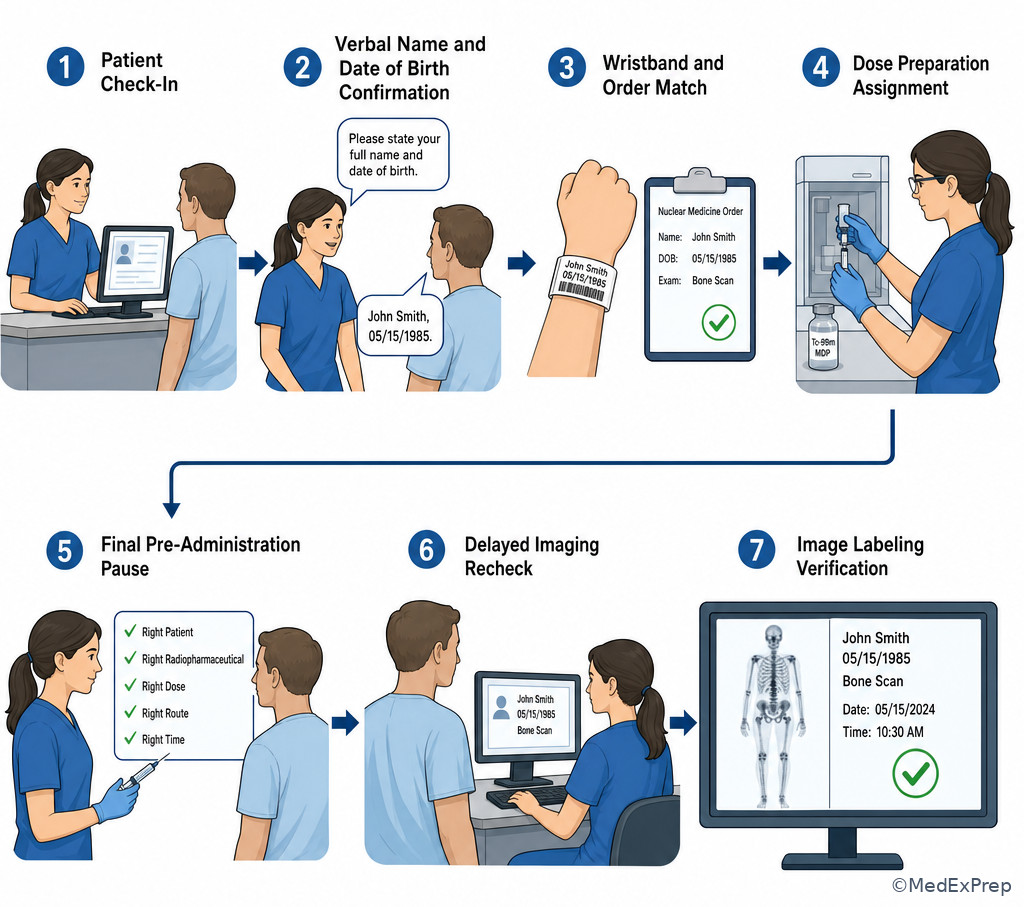
The central decision conflict is Is one identification check at arrival enough, or do high-risk workflow transitions require another pause? The NMTCB-safe answer is that identity must be confirmed at critical steps, especially before dose preparation assignment, before administration, and before image labeling/acquisition. The single rule is: repeat or re-anchor identity when the workflow changes in a way that could separate the patient from the correct dose or data.
This matters because nuclear medicine workflows are staggered. A patient may be checked in, then wait, then move to injection, then return for delayed imaging. Similar names, multiple doses on the hot lab bench, schedule reshuffling, or room transfers create risk. See Fig 3. The exam often frames this as a busy department with two bone scans and one thyroid uptake patient arriving close together. The correct answer is rarely “work faster.” It is to use deliberate checkpoints.
Choose an additional confirmation when the dose is drawn up for a specific patient, when another staff member hands off the patient, when a delayed image is started hours later, or when the image label/import screen is opened. Reject the idea that once the patient was verified at registration, the rest of the process can run on assumption. In nuclear medicine, data mismatch can be as serious as dose mismatch because the study can be attributed to the wrong record.
Key rule: Every handoff or delay is a chance for patient-dose-data separation; add a checkpoint before the irreversible step.
B Worked example
A 46-year-old outpatient with obesity and osteoarthritis is scheduled for a three-phase bone scan. She also has hypothyroidism. At check-in, her name and date of birth were correctly verified. Two hours later she returns from the restroom for delayed images, and another technologist is now covering the camera room. A second patient with a similar last name is also waiting for a thyroid scan. The tempting wrong move is to rely on the earlier check-in and the fact that the patient is already in the department. The most appropriate next step is to re-verify identity and confirm the correct study before starting delayed acquisition and image labeling.
Reasoning chain: Identify the task: determine whether re-verification is necessary after a delay and staff handoff. Extract key facts: time gap, covering technologist, similar-name patient nearby, and transition to another critical step. Apply the rule: high-risk transitions require renewed confirmation. Eliminate distractors: prior verification does not cover current risk; patient familiarity is weak; the presence of a recent injection does not guarantee the right person is at the camera now. Verify: once identity and accession match, proceed with imaging.
C Exam trap
Common wrong answer: Skip re-identification because the patient never left the department.
Why it is tempting: Learners often undervalue handoffs, time delays, and similar-name risk when no obvious error has occurred.
Single clue that eliminates it: There was a workflow transition to delayed imaging with another technologist and a similar-name patient present.
D Checkpoint
Question: Which scenario most clearly requires an additional patient identification check?
- A. An alert patient remains seated in the injection chair for two minutes while supplies are opened.
- B. A patient returns hours later for delayed imaging after check-in and injection were performed earlier.
- C. The same technologist re-enters the room to adjust a pillow before acquisition begins.
- D. A patient asks one clarifying question about the camera time after initial verification.
Answer: B
- A: Tempting because the dose step is important, but there is no major separation event in this brief interval.
- B: Correct because delayed return creates a new high-risk transition where patient-dose-data matching must be re-established.
- C: Tempting because any room re-entry feels like a new step, but this is not the strongest example of workflow separation.
- D: Tempting because patient interaction is ongoing, but a question alone does not create the same misidentification risk as a delayed return.
If you missed this: Review 1.1.1.4 High-risk moments: before dose preparation, administration, and imaging — focus on which workflow transitions create separation risk.
- The safest time for an extra identity pause is immediately before the irreversible step.
- True or False: Initial registration check covers delayed imaging later the same day. False.
- Name 3 separation risks: handoff, time delay, similar-name overlap.
Practitioner Action: Assess whether the patient has moved through a handoff, delay, or room change. Intervene with renewed identity confirmation before dose administration or imaging. Refer unresolved discrepancies to the authorized team before proceeding. Document repeat verification at critical transitions according to protocol.
Exam takeaway: A mismatch triggers stop-verify-escalate-document, not guess-and-proceed.
flowchart TD
A[Discrepancy noted] --> B[Stop dose or imaging workflow]
B --> C[Recheck identifiers, order, schedule]
C --> D{Resolved?}
D -- Yes --> E[Proceed with documented correction]
D -- No --> F[Notify supervisor or authorized provider]
F --> G[Hold procedure until cleared] Exam takeaway: The last identity check should occur immediately before the dose reaches the patient.
1.1.1.7 Discrepancies, documentation, and scope-safe escalation
A Explanation
The final integration conflict is When a mismatch appears, do you solve it yourself by choosing the most likely explanation, or do you stop and escalate within scope? For the NMTCB exam, the correct action is technologist-level resolution only when the discrepancy is straightforward and authorized by protocol; otherwise, stop and escalate. The single finding that resolves this choice is whether identity can be reliably confirmed without independent reinterpretation or unauthorized change. If not, do not proceed.
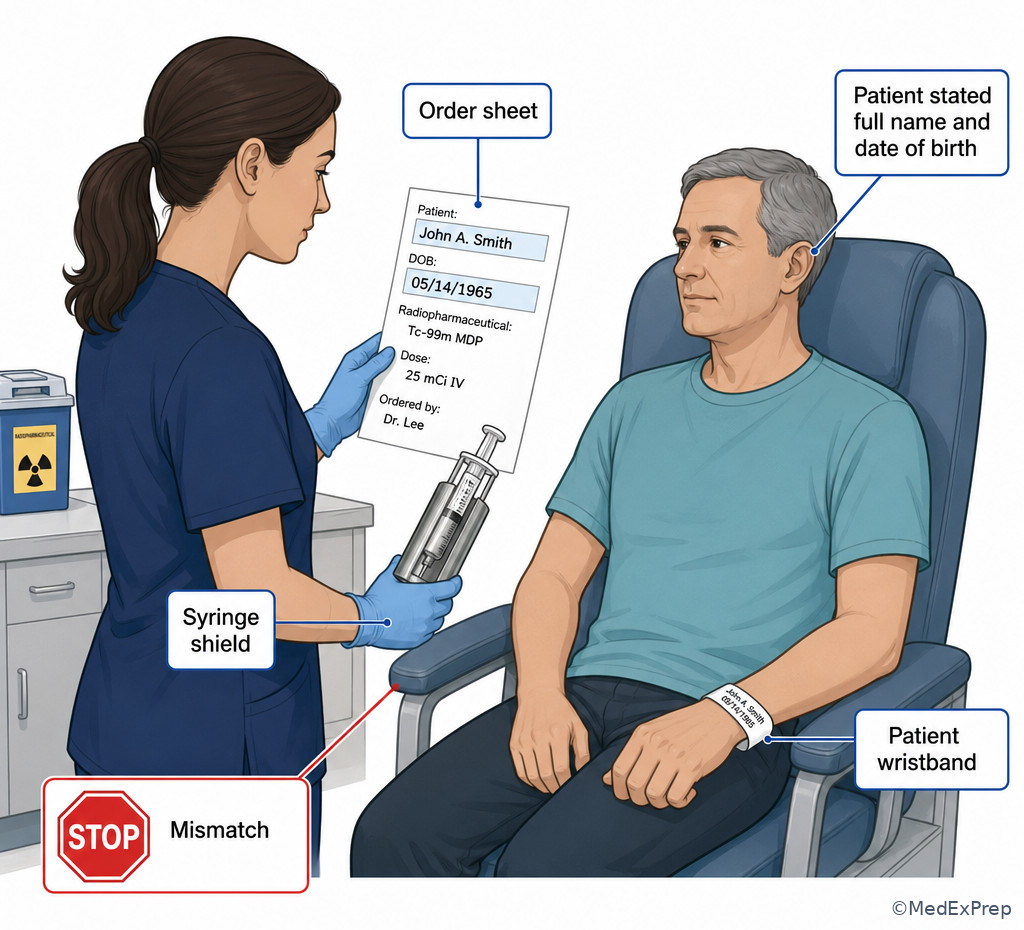
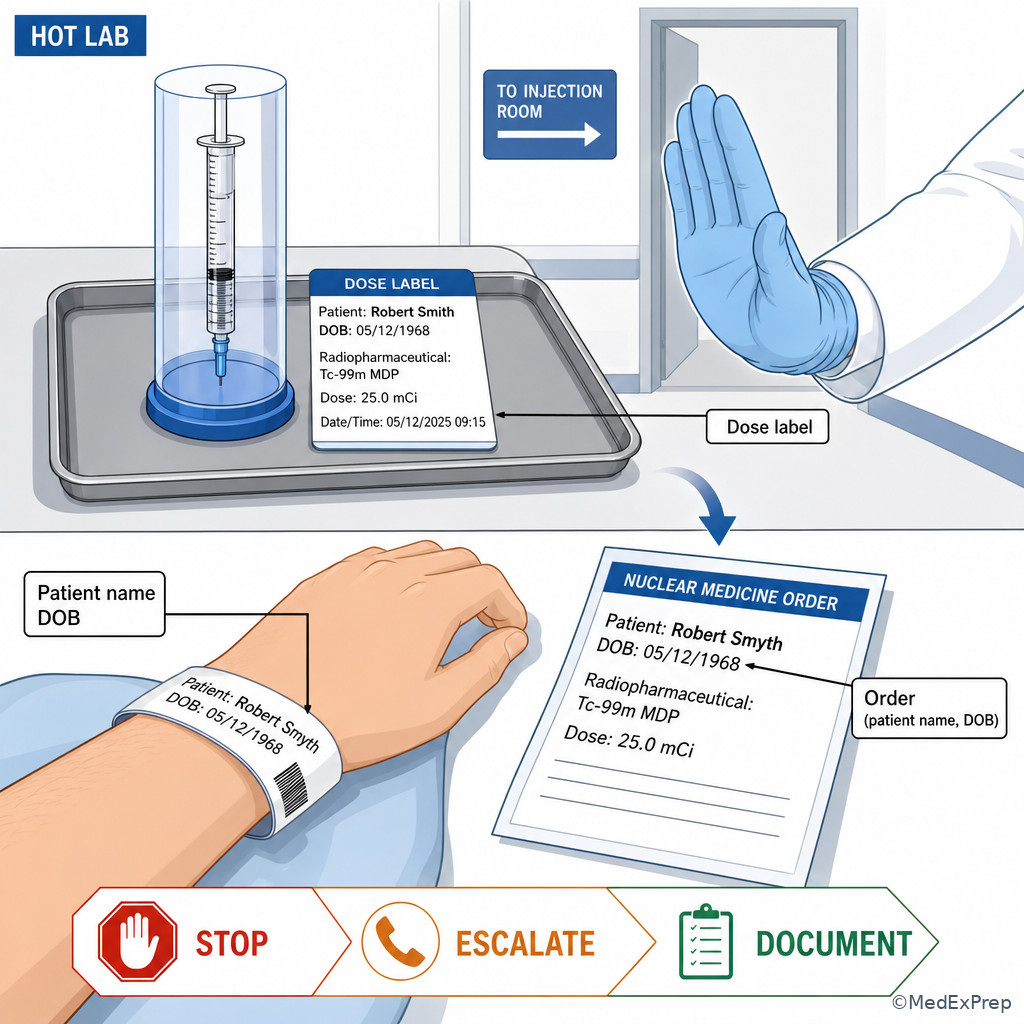
Examples of scope-safe technologist action include rechecking the armband, re-asking identifiers, comparing the electronic order, confirming the schedule, and contacting the appropriate supervising team member. Out-of-scope actions include independently changing the ordered study, selecting another radiopharmaceutical because the patient says something different, or deciding to ignore a mismatch because the imaging slot is tight. See Fig 4.
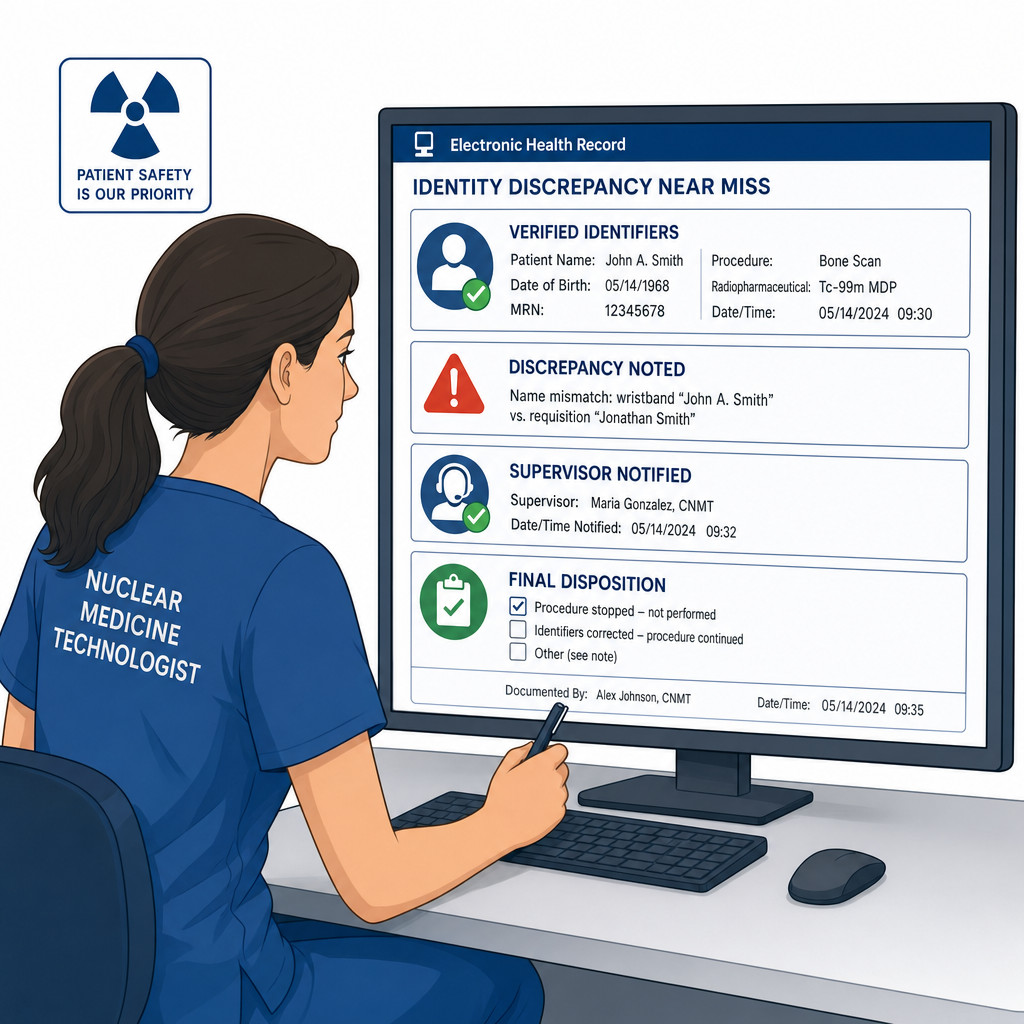
Documentation is part of the safety action, not an afterthought. Record what identifiers were used, what discrepancy was found, who was notified, what instructions were received, and whether the procedure proceeded, was delayed, or was rescheduled. Near misses matter because they reveal system weaknesses such as duplicate names, poor handoff, or incomplete labels. On exam questions, the most appropriate next step often includes both safety action and documentation.
Key rule: Stop first, clarify second, document third, and proceed only after authorized resolution.
Recall: In the upcoming topic Allergies Contraindications And Escalation, the same principle applies: the technologist screens and identifies risk, but does not independently override provider-level decisions.
B Worked example
A 62-year-old inpatient with COPD and metastatic prostate cancer is scheduled for a bone scan. He also has mild confusion after overnight benzodiazepines. The wristband matches the electronic order, but the syringe label on the prepared dose tray contains a similar last name with one different letter. A nurse says, “It’s probably just a spelling issue—we use the same room every week.” His oxygen saturation is mildly low, which is distracting but not the key issue here. The most appropriate technologist action is to stop the administration workflow, reconcile the label against the verified patient and order, and escalate per protocol before any dose is given.
Reasoning chain: Identify the task: prevent a wrong-patient or wrong-dose event. Extract key facts: dose label mismatch, unreliable convenience explanation, and a prepared radiopharmaceutical awaiting administration. Apply the rule: any unresolved identity discrepancy at the dose-label stage requires stop-verify-escalate. Eliminate distractors: room familiarity is not an identifier; low oxygen saturation may matter clinically but does not resolve the labeling problem; the technologist cannot simply relabel or assume the intended patient. Verify: only proceed after an authorized, documented correction.
C Exam trap
Common wrong answer: Correct the label yourself and continue because the intended patient seems obvious.
Why it is tempting: The mismatch may look minor, and workflow pressure pushes learners toward a quick fix.
Single clue that eliminates it: The dose label itself does not match the verified patient, creating a traceability and safety failure that requires formal resolution.
D Checkpoint
Question: Which action is most appropriate when a verified patient’s wristband matches the order, but the prepared dose label appears to belong to a similarly named patient?
- A. Administer the dose if the procedure room and time slot are correct.
- B. Handwrite a quick correction on the label and continue.
- C. Stop the workflow, reconcile the discrepancy, notify the appropriate supervising personnel, and document.
- D. Ask the patient whether the alternate last name has ever been used in the family.
Answer: C
- A: Tempting because room/time fit the schedule, but those are not sufficient to override a dose-label mismatch.
- B: Tempting because it seems efficient, but self-correcting a traceability problem without formal resolution is unsafe and potentially out of policy.
- C: Correct because dose-to-patient traceability must be re-established before administration.
- D: Tempting because it seeks more information, but patient speculation does not resolve a labeling control failure.
If you missed this: Review 1.1.1.5 Discrepancies, documentation, and scope-safe escalation — focus on stop-verify-escalate-document when traceability breaks.
Memory anchor: For any mismatch, remember STOP = Suspend workflow, Trace identifiers, Obtain authorized clarification, Paper the event with documentation.
Practitioner Action: Assess whether the mismatch involves identity, order, dose label, or image data. Intervene by halting the next irreversible step and performing protocol-based reconciliation. Refer beyond-scope or unresolved issues to the supervising physician, pharmacist, nurse, or department lead as appropriate. Document the discrepancy, near-miss or event details, communications, and final outcome.
Exam takeaway: If the dose label, order, and patient do not align, no administration should occur until formal reconciliation is complete.
Exam takeaway: Near-miss documentation is part of prevention, not optional paperwork.
Exam Traps & Differentiators
The most common wrong answer in this topic is proceeding on a weak cue because the workflow feels routine. The exam rewards the learner who notices the single unsafe detail that breaks the chain: a leading yes/no question, a mismatch between patient expectation and order, a nonverbal patient verified by only one source, or a mislabeled prepared dose.
| Looks acceptable | Why it tempts you | Why it fails | What to do instead |
|---|---|---|---|
| Patient nods yes to stated name | Feels like confirmation | It is a suggested answer, not patient-generated identification | Ask the patient to state full name and DOB |
| Correct room number and transporter report | Seems operationally specific | Room and destination are not accepted identifiers | Use two approved identifiers and order match |
| Order present in EHR | Feels authoritative | Does not resolve right-procedure mismatch by itself | Pause and reconcile with the authorized team |
| Armband matches but dose label differs | Tempts quick relabeling | Traceability failure creates administration risk | Stop, reconcile, escalate, document |
| Patient cannot self-identify, so family speaks | Family often knows the patient well | Single-source verification is weaker than multi-source confirmation | Use caregiver plus armband plus record per protocol |
| Commonly confused pair | If the stem says... | Think... |
|---|---|---|
| Correct patient vs correct order | “She states the right name and DOB, but says she expected a different exam” | Right-procedure mismatch; do not proceed yet |
| Unable to answer vs identity uncertain | “Sedated, confused, pediatric, or nonverbal” | Switch to approved alternate verification, not abandonment of verification |
| Busy workflow vs safe workflow | “Two similar names, delayed images, covering technologist” | Add another identity checkpoint |
| Minor label issue vs major traceability issue | “Prepared dose has a similar but not identical name” | Stop the dose workflow immediately |
| Technologist verification vs provider decision | “Patient says the order seems wrong” | Reconcile and escalate; do not independently substitute the study |
- If the stem says “Are you Mr. X?”, think leading prompt and weak verification.
- If the stem says “the patient expected a different exam”, think order reconciliation before any dose action.
- If the stem says “similar names”, think slow down and compare multiple unique identifiers.
- If the stem says “nonverbal, sedated, pediatric, confused”, think alternate approved verification pathway.
- If the stem says “dose label mismatch”, think traceability failure; stop and escalate.
- If the stem says “delayed imaging later the same day”, think repeat identity check at the new critical step.
Related traps from upcoming topics can overlap. For example, once identity is confirmed, the next challenge may be pregnancy screening or contraindication review. A common confusable pattern is thinking a patient-prep issue can be addressed before identity is settled. It cannot; identification comes first, then screening.
Review connection: The traps above test workflow control under uncertainty. If any felt unfamiliar, revisit 1.1.1.2 Applied verification: matching the patient to the right order and procedure and 1.1.1.5 Discrepancies, documentation, and scope-safe escalation before attempting the Self-check quiz.
Tables
| Verification element | High-yield rule | Proceed / stop trigger |
|---|---|---|
| Full name | Use as one accepted identifier when institution-approved | Proceed only if it matches all records used |
| Date of birth | Preferred second identifier in routine workflows | Stop if verbal DOB conflicts with record and cannot be explained |
| Medical record number | Useful unique identifier, especially for similar names | Proceed when aligned with patient/order/armband |
| Armband | Important but not sufficient alone if other mismatch exists | Stop if absent, unreadable, or conflicting |
| Scheduled procedure | Must match patient and order before dose workflow | Stop if the patient expectation and order conflict |
| Dose label | Must trace directly to the verified patient and study | Stop if the label differs in any meaningful way |
| Image accession/label | Check before acquisition and processing | Stop if data are loading under another patient record |
| Accepted or weak? | Item | Why |
|---|---|---|
| Accepted | Patient states full name | Direct patient-generated identifier |
| Accepted | Patient states date of birth | Common institution-approved second identifier |
| Accepted | Medical record number on verified sources | Useful unique match point |
| Weak / not sufficient | Room number | Location can be wrong or changed |
| Weak / not sufficient | “Bone scan patient” | Procedure label is not identity |
| Weak / not sufficient | Physical appearance | Subjective and error-prone |
| Weak / not sufficient | Transporter recognition alone | Single convenience source, not formal verification |
| Differential situation | What the stem gives you | Best technologist action | Discriminator |
|---|---|---|---|
| Alert adult, routine intake | Can answer questions clearly | Ask for patient-stated full name and DOB; match to order/armband | Reliable self-identification is available |
| Confused or sedated inpatient | Incorrect or inconsistent self-report | Use alternate approved verification sources | Self-identification is unreliable |
| Identity matches, study differs | Patient expected another exam | Stop and reconcile order/procedure mismatch | Right-procedure problem, not right-patient problem alone |
| Dose label mismatch | Prepared dose linked to similar name | Stop administration workflow and escalate | Traceability failure |
| Delayed imaging after prior check-in | Hours later, possibly new staff handoff | Repeat identity verification before acquisition | Workflow separation increases risk |
Algorithm / Approach
Exam takeaway: The safest approach links intake verification, order match, dose match, and acquisition labeling into one continuous chain.
Use this approach whenever the question asks for the most appropriate next step after an identity concern. The decision hierarchy is consistent: verify, compare, stop if mismatch, escalate within scope, document. See Fig 4, Fig 5, and Fig 6.
Rapid Review
- Patient-stated identifiers -> stronger than yes/no confirmation
- Room number -> location cue, not identity proof
- Correct patient but wrong exam expectation -> order reconciliation problem
- Nonverbal patient -> switch to alternate approved verification, not assumption
- Similar names -> add unique identifier comparison and slow down
- Armband alone -> insufficient if another source conflicts
- Dose label mismatch -> traceability failure requiring stop
- Delayed images later same day -> repeat identity check before acquisition
- Transporter confirmation -> supportive at most, never sole determinant
- Patient familiarity -> dangerous shortcut in repeat-visit departments
- Procedure nickname -> not an accepted identifier
- Identity discrepancy -> stop, verify, escalate, document
- Technologist scope -> verify and notify, do not independently change the ordered study
- Near miss -> document because prevention data improve workflow safety
Self-check quiz
1. An alert outpatient arrives for a scheduled bone scan. He is wearing a wristband and says, “I come here all the time.” Which action is the most appropriate next step before continuing the workflow?
- A. Ask him to state his full name and date of birth, then compare them with the order and wristband.
- B. Accept the wristband as sufficient because he is a returning patient.
- C. Ask whether he is the bone scan patient and proceed if he says yes.
- D. Confirm his room assignment and use that as the second identifier.
2. A patient is awake and cooperative for a thyroid study. Which item is the weakest identifier and should not be used as one of the two primary identifiers?
- A. Date of birth
- B. Medical record number
- C. Room number
- D. Full name
3. A 54-year-old woman with hypertension and osteoarthritis arrives for a scheduled lung scan. She correctly states her name and date of birth, but says her pulmonologist told her she was coming for a gastric emptying study. She is mildly anxious and mentions she skipped breakfast, which makes the gastric study sound plausible. What is the most appropriate next step?
- A. Proceed with the lung scan because the electronic order is active.
- B. Stop and reconcile the discrepancy between the patient expectation and the order before any dose action.
- C. Ask the patient which study she would prefer and update the schedule accordingly.
- D. Continue intake and clarify only after radiopharmaceutical administration.
4. A 79-year-old inpatient with dementia, hearing impairment, and recent opioid sedation is brought for a hepatobiliary scan. He gives an incorrect birth month when asked. His wristband matches the order, and his daughter confirms his full name and date of birth. The transporter says he came from the correct room. What is the most appropriate technologist action?
- A. Cancel the procedure because the patient cannot self-identify accurately.
- B. Use the daughter’s statement alone because family is usually most accurate.
- C. Use alternate approved verification with wristband, order, and caregiver confirmation, then document the method used.
- D. Proceed based on the transporter’s confirmation because the unit and room match.
5. A 44-year-old outpatient with rheumatoid arthritis and obesity was verified at check-in and injected for a bone scan. She returns 3 hours later for delayed images, and a different technologist is now covering the camera. Another patient with a similar last name is waiting nearby. What is the most appropriate next step?
- A. Re-verify the patient’s identity and accession before starting acquisition.
- B. Proceed because the earlier injection confirms who she is.
- C. Ask the waiting room clerk whether this is the same patient from earlier.
- D. Start imaging first and correct the record later if needed.
6. A 63-year-old man with prostate cancer, COPD, and chronic pain arrives for a bone scan injection. He is mildly somnolent after previsit medication. His wristband and electronic order match, but the prepared syringe label shows a similar last name with one different letter. A nurse says the patients are often mixed up on paper and this is probably the intended dose. What is the most appropriate technologist action?
- A. Administer the dose because the wristband and order match the patient.
- B. Correct the label manually and continue to avoid wasting the dose.
- C. Stop the workflow, reconcile the dose label discrepancy, notify appropriate supervising personnel, and document.
- D. Ask the patient whether the alternate surname spelling has ever appeared in his records.
7. A 32-year-old inpatient with sickle cell disease, pregnancy status not yet reviewed, and severe pain is sent for a ventilation-perfusion study. She correctly states her name and date of birth, but the requisition printed in the camera room carries another patient’s accession number while the wristband and electronic chart match. A respiratory therapist is waiting to begin the ventilation portion. What is the most appropriate next step?
- A. Proceed because patient identity is correct and the accession can be fixed during processing.
- B. Pause the workflow and correct the record-link mismatch before imaging begins.
- C. Ask the respiratory therapist to decide whether imaging should continue.
- D. Begin the ventilation portion but hold perfusion until the paperwork is clarified.
8. A 6-year-old child with a seizure disorder and developmental delay arrives for a renal scan with both parents. The child cannot reliably answer questions. The armband matches the order, but one parent states the child is scheduled for a gastric emptying study because of nausea, while the other parent says it is the kidney test ordered by nephrology. The schedule and electronic order list a renal scan. What is the most appropriate next step?
- A. Proceed with the renal scan because the order and armband match, and parent disagreement is not relevant.
- B. Ask the child to point to where it hurts and use that to infer the correct study.
- C. Stop and reconcile the procedure discrepancy with the authorized team before dose preparation or administration.
- D. Let the parents decide which study is more important today.
Answer key
1. Correct answer: A
- A: Tempting because it is the formal workflow, and it is correct for that exact reason: the patient is alert and can self-identify, so the safest action is patient-stated name and DOB matched to independent records. Single stem clue: the patient is alert and cooperative. Source: Joint Commission patient identification goals; SNMMI practice expectations for safe patient care and documentation.
- B: Tempting because the wristband feels official and the patient is familiar, but returning-patient familiarity does not replace active verification. Single stem clue: “I come here all the time” is a shortcut trap, not proof. Source: Joint Commission.
- C: Tempting because it mentions the study, but asking whether he is the bone scan patient uses a leading prompt and procedure label rather than identity. Single stem clue: the question is yes/no and study-based. Source: Joint Commission.
- D: Tempting because it adds a second data point, but room assignment is not an accepted primary identifier. Single stem clue: room location is logistical, not unique identity. Source: Joint Commission.
If you missed this: Review 1.1.1.1 Foundations: what counts as correct patient identification — focus on patient-stated identifiers versus leading prompts and location-based cues.
2. Correct answer: C
- A: Tempting because learners may think DOB is common and therefore weak, but it remains a standard accepted identifier when used correctly. Single stem clue: the question asks for the weakest identifier. Source: Joint Commission.
- B: Tempting because medical record numbers may feel abstract, but they are often highly useful unique identifiers. Single stem clue: MRN is unique, unlike a room number. Source: Joint Commission.
- C: Correct because room number identifies location, not the individual patient, and can change. Single stem clue: it is a location field rather than patient identity. Source: Joint Commission.
- D: Tempting because full name can be duplicated, but as part of a two-identifier process it remains a standard accepted identifier. Single stem clue: full name is still person-specific, unlike room number. Source: Joint Commission.
If you missed this: Review 1.1.1.1 Foundations: what counts as correct patient identification — focus on why room number is never a primary patient identifier.
3. Correct answer: B
- A: Tempting because the order is active and present, but the patient’s expectation conflicts with the ordered exam, creating a right-procedure issue that must be reconciled before any dose action. Single stem clue: she expected a different study. Source: Joint Commission; SNMMI procedure quality and patient care principles.
- B: Correct because patient identity and correct procedure must both be verified before progression to dose handling or administration. Single stem clue: mismatch between patient expectation and documented order. Source: Joint Commission; SNMMI.
- C: Tempting because the patient is an important information source, but choosing the study is outside technologist autonomy; it requires formal reconciliation. Single stem clue: asks the patient to decide the exam. Source: NMTCB scope expectations; SNMMI.
- D: Tempting because it seems efficient, but after administration the error can be much harder to reverse and may already constitute wrong-procedure care. Single stem clue: “after radiopharmaceutical administration” is too late. Source: Joint Commission; radiation safety principles.
If you missed this: Review 1.1.1.2 Applied verification: matching the patient to the right order and procedure — focus on why the correct patient is still unsafe if the correct study is uncertain.
4. Correct answer: C
- A: Tempting because verbal inaccuracy feels disqualifying, but inability to self-identify reliably means you switch methods rather than automatically cancel. Single stem clue: dementia, hearing impairment, and sedation. Source: Joint Commission; patient care safety standards.
- B: Tempting because family often helps, but one source alone is weaker than combined approved sources. Single stem clue: wristband and order are also available and should be used. Source: Joint Commission.
- C: Correct because alternate verification is the proper approach when self-identification is unreliable, and documenting the alternate method preserves traceability. Single stem clue: the patient cannot reliably answer, but multiple confirming sources are present. Source: Joint Commission; SNMMI practice standards.
- D: Tempting because transport staff know the route, but transport location is not a formal identity method. Single stem clue: “correct room” is a location cue only. Source: Joint Commission.
If you missed this: Review 1.1.1.3 Special situations: patients who cannot reliably self-identify — focus on the discriminator that unreliable self-report changes the method, not the safety standard.
5. Correct answer: A
- A: Correct because delayed imaging, staff handoff, and a similar-name patient create a new high-risk transition requiring renewed identity confirmation. Single stem clue: 3-hour delay plus different technologist. Source: Joint Commission; workflow safety principles in nuclear medicine.
- B: Tempting because prior injection seems to anchor the patient, but it does not protect against delayed-step misidentification. Single stem clue: she returned later for a new critical step. Source: Joint Commission.
- C: Tempting because it uses another staff member, but clerk recognition is weaker than direct re-verification against patient records. Single stem clue: waiting room confirmation is not formal identity verification. Source: Joint Commission.
- D: Tempting because data can be edited in some systems, but starting acquisition under uncertain identity risks wrong-patient labeling and workflow error. Single stem clue: similar last name nearby makes later correction unsafe. Source: Joint Commission; data integrity principles.
If you missed this: Review 1.1.1.4 High-risk moments: before dose preparation, administration, and imaging — focus on why handoffs and delayed returns trigger repeat identification.
6. Correct answer: C
- A: Tempting because the patient and order match, but administration still requires the dose label to trace correctly to that patient. Single stem clue: syringe label name mismatch. Source: Joint Commission; nuclear medicine dose traceability standards.
- B: Tempting because it avoids waste and seems practical, but informal relabeling bypasses controlled reconciliation and documentation. Single stem clue: prepared dose already has a discrepant label. Source: SNMMI radiopharmacy handling principles; institutional traceability expectations.
- C: Correct because a dose-label mismatch creates a wrong-patient risk and must trigger stop-verify-escalate-document before administration. Single stem clue: one-letter last-name difference on the syringe label. Source: Joint Commission; radiation safety practice standards.
- D: Tempting because it seeks clarification, but patient speculation cannot resolve a controlled labeling discrepancy. Single stem clue: this is a dose traceability problem, not a nickname question. Source: Joint Commission.
If you missed this: Review 1.1.1.5 Discrepancies, documentation, and scope-safe escalation — focus on the rule that dose-label mismatch breaks traceability and requires formal resolution.
7. Correct answer: B
- A: Tempting because the patient herself is correctly identified, but the wrong accession number can attach images to the wrong record and is therefore a serious identity-data mismatch. Single stem clue: requisition carries another patient’s accession number. Source: Joint Commission; data integrity expectations in imaging workflows.
- B: Correct because patient verification must extend to the record link used for imaging and processing; accession mismatch must be corrected before imaging begins. Single stem clue: another patient’s accession number is already in the workflow. Source: Joint Commission; SNMMI quality and documentation standards.
- C: Tempting because another clinician is involved in the procedure, but deciding whether to proceed without correcting the identity-data mismatch is not delegated to the therapist. Single stem clue: the problem is record linkage, not ventilation technique. Source: NMTCB scope expectations.
- D: Tempting because it partially delays the study, but beginning any portion under mismatched data still risks wrong-record documentation and workflow confusion. Single stem clue: the error exists before the first image is acquired. Source: Joint Commission.
If you missed this: Review 1.1.1.4 High-risk moments: before dose preparation, administration, and imaging — focus on why identity checks also include accession and image-label verification.
8. Correct answer: C
- A: Tempting because the armband and order match, but parent disagreement about the intended study creates a right-procedure discrepancy that must be reconciled before dose preparation. Single stem clue: conflicting expectations about which exam was intended. Source: Joint Commission; patient care workflow standards.
- B: Tempting because symptoms may feel helpful, but using a child’s gesture to infer the correct exam is not a valid substitute for order reconciliation. Single stem clue: the issue is procedure mismatch, not symptom localization. Source: NMTCB scope expectations.
- C: Correct because in a nonverbal pediatric patient, identity can be verified through alternate methods, but the procedure discrepancy still requires formal reconciliation before any dose step. Single stem clue: the child cannot self-identify and the adults disagree about the planned study. Source: Joint Commission; SNMMI pediatric care and workflow principles.
- D: Tempting because guardians are central to pediatric care, but they do not independently choose which ordered nuclear medicine study proceeds. Single stem clue: parent preference is not provider authorization. Source: NMTCB scope expectations.
If you missed this: Review 1.1.1.2 Applied verification: matching the patient to the right order and procedure and 1.1.1.3 Special situations: patients who cannot reliably self-identify — focus on the difference between alternate patient identification and unresolved procedure mismatch.