Why it matters
- Board questions often hide a prevention task inside a chronic disease or acute complaint stem; the best answer depends on recognizing whether the patient is well, at risk, newly detected, or already living with disease.
- In primary care, prevention decisions drive screening selection, counseling priorities, vaccine timing, medication risk reduction, and follow-up intervals.
- FNP exams reward the safest outpatient action: reduce risk early, detect disease appropriately, avoid overtesting, and escalate only when red flags exceed office scope.
- Prevention frameworks organize hundreds of future topics, from immunizations and screening to diabetes, hypertension, tobacco cessation, and falls prevention.
Exam takeaway: Match the patient's position on the health-disease timeline to the correct prevention level before choosing the intervention.
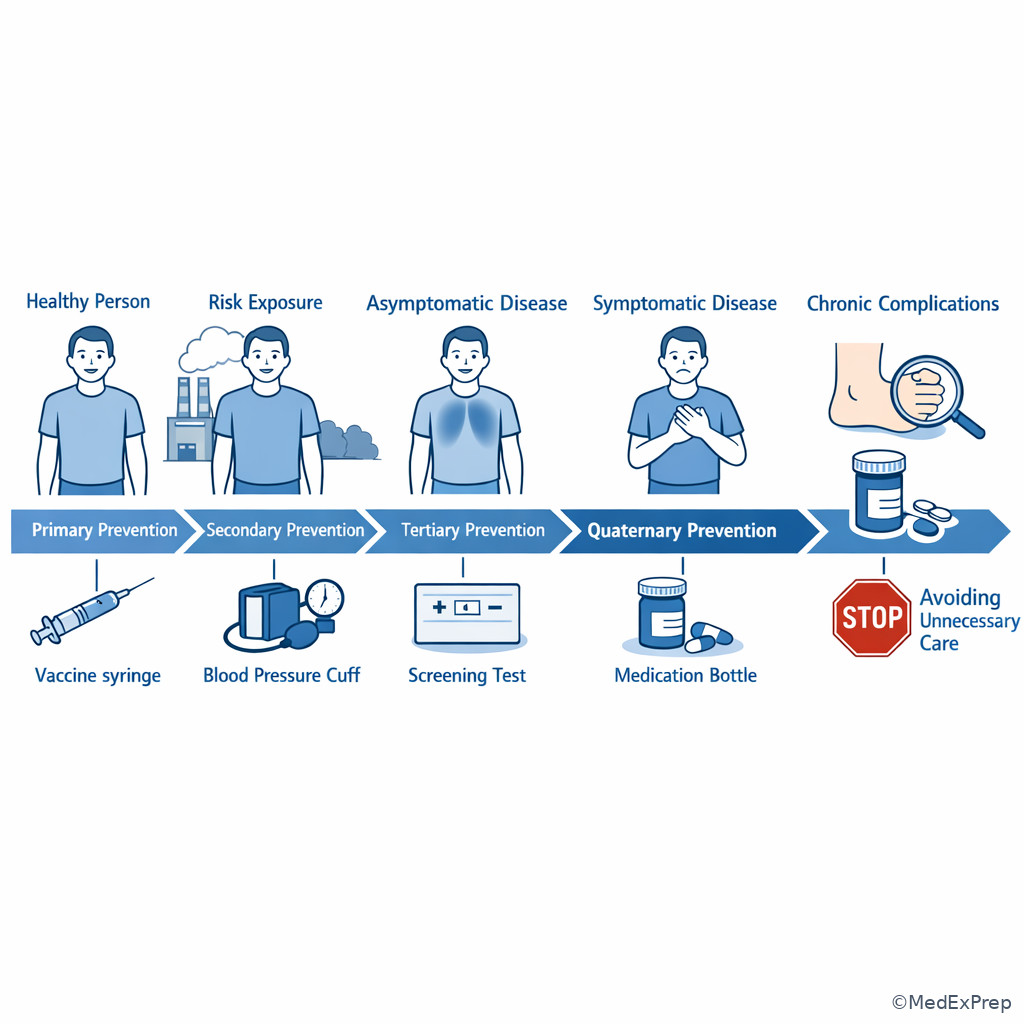
flowchart LR A[No disease yet] --> B[Risk exposure present] B --> C[Primary prevention] A --> D[Silent disease possible] D --> E[Secondary prevention] E --> F[Diagnosed disease] F --> G[Tertiary prevention] G --> H[Risk of overtreatment or unnecessary harm] H --> I[Quaternary prevention]
See Fig 1 for the core framework that separates prevention levels on exam stems.
Key Terms & Must-Know Facts
1.1.1.1 Key terms
- Primary prevention: action before disease occurs
- Secondary prevention: early detection of asymptomatic disease
- Tertiary prevention: reduce complications of established disease
- Quaternary prevention: avoid unnecessary medical harm
- Risk factor: characteristic associated with higher disease probability
- Modifiable risk factor: changeable exposure or behavior
- Nonmodifiable risk factor: age, sex, genetics, family history
- Absolute risk: probability an event occurs in a defined period
- Relative risk: comparison of risk between exposed and unexposed groups
- Risk stratification: sorting patients by likelihood of future disease or harm
- Health promotion: behaviors and systems that improve wellness
- Counseling intervention: structured advice to reduce risk
- Red flag: finding that requires urgent escalation rather than routine prevention
- Shared decision-making: patient-centered choice when benefits and harms must be weighed
1.1.1.2 Must-know facts
- Vaccines, smoking prevention, seat belts, and folic acid counseling are primary prevention.
- Screening tests are secondary prevention only when the patient is asymptomatic.
- A1c monitoring in known diabetes and foot exams in diabetic neuropathy prevention are tertiary prevention.
- Stopping unnecessary screening in a patient unlikely to benefit is quaternary prevention.
- Family history changes risk but does not itself mean disease is present.
- Board stems often tempt you to order tests when counseling or immunization is actually the best answer.
- If the patient is unstable, prevention is no longer the priority; emergency evaluation is.
- Risk reduction plans should include counseling, environment, medication safety, and follow-up.
- Primary care prevention is lifespan-based: pediatric, adolescent, adult, pregnant-capable, and older adult needs differ.
| Prevention level | When used | Typical FNP action | Common exam clue |
|---|---|---|---|
| Primary | Before disease develops | Immunize, counsel, reduce exposure | Patient has risk but no diagnosis |
| Secondary | Possible silent disease | Select indicated screening test | Asymptomatic patient due for screening |
| Tertiary | Known disease exists | Prevent complications, monitor control | Diagnosis already established |
| Quaternary | Risk of overmedicalization | Avoid unnecessary tests/treatments | Low-value or harmful intervention |
Exam takeaway: Use the patient’s timeline position to separate prevention from screening and disease management.
Core content
1.1.1.3 Foundational framework: choosing the correct prevention level
A Explanation
The decision conflict is simple but heavily tested: is the best outpatient action meant to prevent disease from occurring, detect silent disease early, limit complications of known disease, or avoid unnecessary medical harm? The single rule that resolves the conflict is the patient’s position on the health-disease timeline. If no disease exists yet, think primary prevention. If disease may exist but is asymptomatic, think secondary prevention. If the patient already carries the diagnosis, think tertiary prevention. If the stem pushes a low-value intervention with little benefit and real burden, think quaternary prevention.
WHY THIS IS TESTED: exam writers want to know whether you can choose counseling versus screening versus chronic disease management without being distracted by familiar buzzwords.
Choose primary prevention when the intervention reduces incidence: vaccines, healthy-weight counseling, tobacco prevention, folic acid before conception, sunscreen use, safer-sex education, and fall-proofing the home before an injury occurs. Reject secondary prevention if the patient has no indication for a screening test yet or if the stem is really about exposure reduction. Choose secondary prevention when the patient is asymptomatic but due for a recommended test, such as blood pressure measurement, colorectal screening, or depression screening. Reject tertiary prevention unless a diagnosis is already known. Choose tertiary prevention when the goal is minimizing disability or complications: diabetic retinal exams, statin use in established ASCVD risk management, pulmonary rehab in COPD, and blood pressure control after CKD is diagnosed. Quaternary prevention matters when overtesting, overtreatment, duplicate imaging, or low-yield screening is the trap.
Exam takeaway: Choose the intervention only after deciding where the patient sits on the disease timeline.
B Worked example
A 44-year-old woman presents for an annual visit. She has obesity and a strong family history of type 2 diabetes and premature myocardial infarction. She reports no polyuria, weight loss, chest pain, or dyspnea. She asks whether she should “start checking her sugars at home because diabetes runs in the family.” Her fasting lipid panel from a work fair last month was mildly abnormal, and she read online about coronary calcium scans. The task is to identify the most appropriate prevention category for counseling on weight loss, exercise, and nutrition.
Reasoning chain: identify task → classify intervention. She has risk factors but no diagnosis of diabetes or ASCVD. Extract key facts: asymptomatic, family history positive, obesity present, no disease established. Apply rule: lifestyle counseling to lower future disease incidence is primary prevention. Eliminate distractors: home glucose monitoring is not first-line prevention in an asymptomatic person without diabetes; coronary calcium scanning may be considered in selected risk discussions but is not the clearest initial prevention principle in this stem; lipid review may matter, but the question asks the category of counseling. Verify: primary prevention fits best.
C Exam trap
D Checkpoint
Question: A 62-year-old man with established type 2 diabetes, CKD stage 3a, and hypertension presents for follow-up. He denies symptoms. Which action is the best example of tertiary prevention?
- Administering an influenza vaccine
- Ordering a urine albumin-to-creatinine ratio and reinforcing blood pressure control
- Providing counseling on smoking avoidance to his teenage grandson
- Discussing whether screening should be discontinued after limited life expectancy
- A: Tempting because vaccines prevent morbidity in high-risk adults; wrong here because vaccination is primary prevention, even in a patient with chronic disease.
- B: Tempting because it sounds like routine monitoring; correct because the patient already has diabetes and CKD, so testing and BP control are aimed at reducing complications.
- C: Tempting because family-centered counseling is common in primary care; wrong because it refers to primary prevention in another person, not tertiary prevention for this patient.
- D: Tempting because preventing harm from overtesting is preventive care; wrong because this is quaternary prevention, not tertiary prevention.
Answer: B
1.1.1.4 Risk factors and risk stratification: what changes the plan?
A Explanation
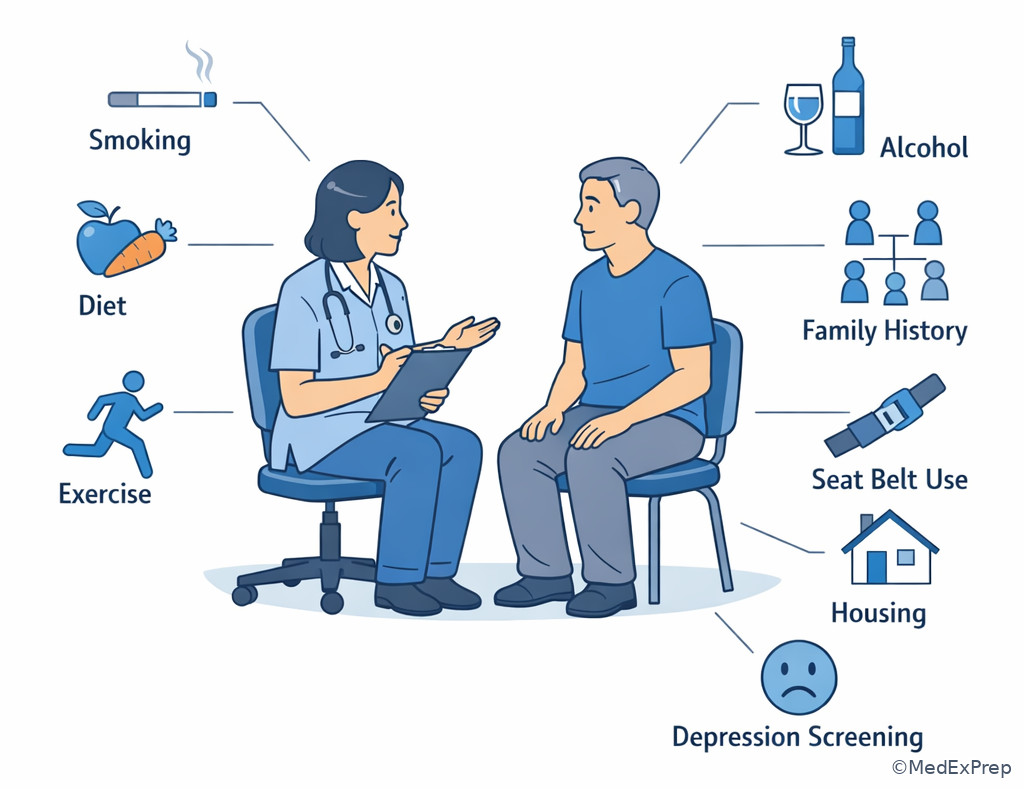
The decision conflict here is whether a stem is asking you to act on modifiable risk, recognize fixed risk, or identify a red flag that ends routine prevention and requires urgent evaluation. The single rule is this: modifiable risks change management directly; nonmodifiable risks change how strongly you screen, counsel, or monitor; red flags change setting and urgency. In outpatient FNP practice, risk assessment begins with age, sex-related risk, family history, personal history, medications, social drivers, behavior, occupation, and environment.
WHY THIS IS TESTED: prevention questions rarely present as pure definitions; they hide inside patient characteristics that alter what the best next step should be.
Modifiable risks include tobacco use, alcohol misuse, sedentary lifestyle, poor diet pattern, obesity, uncontrolled blood pressure, unsafe sex, occupational exposures, poor sleep, and medication nonadherence. Nonmodifiable risks include age, genetics, sex, race as a socialized risk marker within inequitable systems, and family history. These do not become treatment targets by themselves, but they do intensify counseling and influence screening thresholds. Environmental and social risks matter: housing instability, food insecurity, transportation barriers, and violence exposure may be the real drivers of poor outcomes. On exams, the best answer may be a practical risk-reduction step rather than simply labeling the patient “high risk.”
Do not confuse risk stratification with diagnosis. Elevated BMI plus family history does not equal diabetes. A sedentary smoker with hypertension does not automatically have coronary artery disease. Likewise, an asymptomatic patient with a strong family history may deserve earlier or more frequent risk-reduction counseling and indicated screening, but not indiscriminate testing. See Fig 2 for a compact comparison of how risk factors change action.
Exam takeaway: Separate modifiable, nonmodifiable, and urgent red-flag findings before choosing prevention counseling.
B Worked example
A 17-year-old adolescent presents for a sports physical. He has mild intermittent asthma, obesity, and a father who had an MI at age 46. He denies chest pain or syncope and uses his albuterol only a few times each month. His mother is worried because he drinks energy drinks and spends most evenings gaming. A school urine dipstick done months ago showed trace protein after practice. The task is to identify the most important modifiable risk factor to address now for long-term cardiometabolic risk reduction.
Reasoning chain: identify task → not diagnosing disease, but prioritizing risk reduction. Extract key facts: obesity, sedentary behavior, stimulant beverages, positive family history, but no alarm symptoms. Apply rule: family history raises risk but cannot be changed; behavior and weight-related habits are modifiable and therefore actionable. Eliminate distractors: trace protein after exercise is a distracting finding and does not define kidney disease in this scenario; mild asthma is present but not the dominant long-term cardiometabolic target. Verify: lifestyle counseling on activity, nutrition, and stimulant beverage reduction best matches modifiable risk reduction.
C Exam trap
D Checkpoint
Question: Which finding most directly changes prevention counseling because it is modifiable?
- Mother diagnosed with colon cancer at age 52
- Current cigarette smoking one pack daily
- Male sex
- Age 68 years
- A: Tempting because family history strongly alters risk; wrong because it is nonmodifiable, though it affects screening strategy.
- B: Tempting because it is common and obvious; correct because smoking is modifiable and directly targeted by risk-reduction counseling.
- C: Tempting because sex changes disease prevalence; wrong because it is not modifiable.
- D: Tempting because age shifts preventive priorities; wrong because age is nonmodifiable.
Answer: B
- The most common board clue for primary prevention is a patient with risk factors but no diagnosis.
- True or False: Family history is a modifiable risk factor. False.
- Name the 3 sorting buckets for risk findings: modifiable, nonmodifiable, red flag.
Exam takeaway: The correct answer often depends on whether the risk factor should trigger counseling, screening, or urgent escalation.
flowchart TD
A[Risk factor identified] --> B{Type?}
B -->|Behavior or exposure| C[Modifiable: counsel and intervene]
B -->|Age family history genetics| D[Nonmodifiable: stratify and screen appropriately]
B -->|Alarm symptom unstable finding| E[Red flag: urgent evaluation or transfer]
C --> F[Set follow-up plan]
D --> F
E --> G[Do not stay in routine prevention lane] Exam takeaway: Prevention questions often hinge on identifying behavioral and social risk drivers during routine visits.
1.1.1.5 Applying prevention across the lifespan
A Explanation
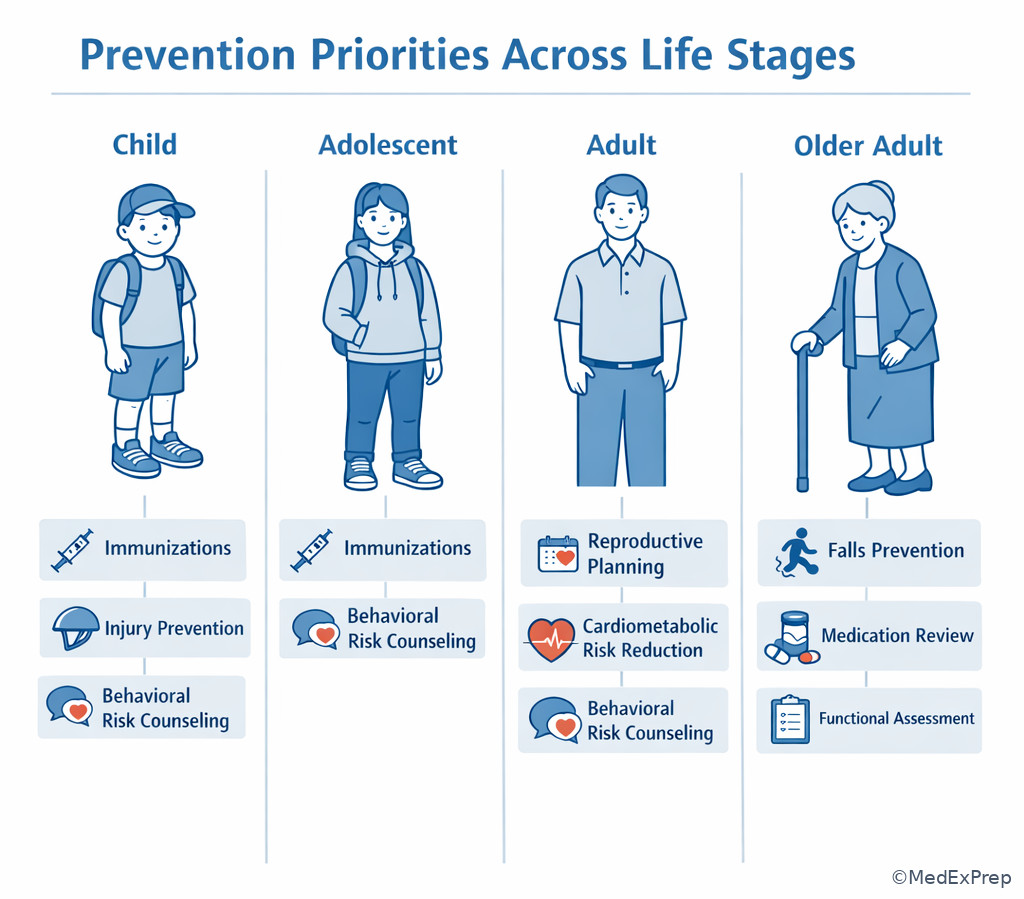
The decision conflict is whether prevention priorities should be selected by age alone, by risk alone, or by a combination of age, risk, and life stage. The single rule is that primary care prevention is lifespan-specific: age sets the baseline framework, while individual risk factors modify what you add or emphasize. A toddler’s prevention priorities are not an older adult’s. An adolescent’s risk reduction may center on confidentiality, sexual health, and substance counseling. A pregnant-capable adult may need folic acid, medication review, and contraception or preconception counseling. Older adults require falls prevention, medication review, vaccination review, functional assessment, and attention to polypharmacy.
WHY THIS IS TESTED: exam stems include age and life stage because they alter the prevention target, even when the disease process seems similar.
Choose the age-matched prevention action first, then layer on risk-based modifications. For children, immunizations, injury prevention, nutrition, developmental surveillance, and caregiver education dominate. For adolescents, confidentiality, depression screening, risky substance use, STI risk reduction, and injury prevention are common test targets. For adults, cardiometabolic risk, cancer screening readiness, tobacco and alcohol counseling, reproductive planning, and vaccine updates matter. For older adults, preventing falls, medication harm, functional decline, social isolation, and vaccine-preventable illness becomes more prominent.
Reject one-size-fits-all prevention. The same intervention can belong to different reasoning pathways depending on context. For example, exercise counseling in a healthy 30-year-old is primary prevention; exercise as part of osteoarthritis disability reduction in a 78-year-old may support tertiary prevention. See Fig 3 for the lifespan comparison framework.
Exam takeaway: Start with age group, then add the patient-specific risk factors that change priority.
B Worked example
A 76-year-old woman presents for a routine visit. She has osteopenia, hypertension, chronic insomnia, and takes diphenhydramine most nights. She reports one “near fall” in the bathroom last week but no injury. She asks whether she should start a detox supplement she saw online to improve energy. Her blood pressure is controlled, and she is due for vaccine review at a later visit. The task is to identify the highest-yield prevention focus for today.
Reasoning chain: identify task → prioritize age-appropriate risk reduction. Extract key facts: older adult, osteopenia, sedating anticholinergic use, near fall, bathroom setting. Apply rule: older adult prevention emphasizes falls, medication safety, and function. Eliminate distractors: supplements are a tempting counseling rabbit hole but are not the key morbidity risk in this stem; controlled BP is already addressed; vaccine review matters but the immediate high-yield prevention priority is falls risk reduction and medication review. Verify: counsel on removing hazards, review sedating medications, assess gait/home safety, and plan follow-up.
C Exam trap
D Checkpoint
Question: In a healthy 15-year-old presenting for a school physical, which prevention focus is most age-concordant?
- Counseling on STI risk, substance use, mood, and injury prevention
- Routine foot checks for diabetic neuropathy
- Home oxygen safety education
- Screening for abdominal aortic aneurysm
- A: Tempting because it sounds broad; correct because adolescent prevention commonly targets sexual health, mood, injury, and substance risk reduction.
- B: Tempting because complication monitoring is preventive; wrong because it applies to established diabetes, not a healthy adolescent.
- C: Tempting because safety counseling is prevention; wrong because it is not age- or condition-appropriate here.
- D: Tempting because screening is prevention; wrong because AAA screening is not relevant to a healthy 15-year-old.
Answer: A
Exam takeaway: Age establishes the prevention framework, then risk factors refine what gets emphasized at the visit.
- The most common prevention focus in older adults that exam writers pair with polypharmacy is falls prevention.
- True or False: A preventive plan should ignore life stage if risk factors are strong. False.
- Name the 3 key adolescent prevention domains commonly tested: mental health, substance use, sexual/injury risk.
1.1.1.6 Turning risk into an outpatient plan: counseling, environment, and follow-up
A Explanation
The decision conflict is whether the best answer is a general recommendation or a specific, realistic, follow-up-ready prevention plan. The single rule: board questions reward actions that can be implemented in primary care today. Good prevention answers are concrete, prioritized, and monitorable. They tell the patient what to change, how to reduce risk, what warning signs matter, and when to return.
WHY THIS IS TESTED: FNP board prep emphasizes practical ambulatory care decisions, not vague health education.
A high-yield prevention plan usually includes: one prioritized risk target, one behavior goal, one environmental or systems intervention, medication safety if relevant, and a follow-up interval. Example: for tobacco use, advise cessation, assess readiness, offer evidence-based support, and arrange follow-up. For falls risk, review sedating medications, recommend home hazard reduction, discuss footwear/assistive devices if appropriate, and schedule reassessment. For obesity-related risk, set a realistic diet/activity goal rather than saying “lose weight.”
Choose the smallest effective plan that addresses the highest-yield modifiable risk. Reject comprehensive but unfocused counseling bundles if one issue clearly dominates the patient’s near-term morbidity. Also reject overmedicalization: not every risk factor needs testing at the first visit. Use shared decision-making when benefits and burdens are closely balanced, and document risk discussion clearly.
Exam takeaway: The best answer usually includes a targeted intervention plus practical follow-up, not advice alone.
B Worked example
A 38-year-old man presents to establish care. He has obesity, untreated obstructive sleep apnea diagnosed years ago, daily vaping after quitting cigarettes, GERD, and a job that requires long overnight driving. His blood pressure today is 146/92 mm Hg, but he drank three energy drinks before the visit. He asks for “whatever test checks if I’m healthy.” The task is to choose the best immediate risk-reduction action in primary care.
Reasoning chain: identify task → not a broad screening panel, but a targeted plan. Extract key facts: multiple modifiable cardiometabolic and safety risks, OSA untreated, drowsy-driving occupation, nicotine exposure ongoing, elevated BP possibly confounded by stimulants. Apply rule: prioritize actionable risks with near-term harm and follow-up. Eliminate distractors: indiscriminate testing is lower value; one elevated BP does not confirm chronic hypertension yet; GERD is not the dominant risk issue. Verify: address sleep apnea adherence or re-evaluation, nicotine cessation counseling, BP recheck under proper conditions, weight/activity counseling, and structured follow-up.
C Exam trap
D Checkpoint
Question: Which outpatient prevention plan is most appropriate for a stable patient with repeated falls risk due to sedating medications and poor lighting at home?
- Advise the patient to be careful and return as needed
- Review medications, recommend home lighting and hazard changes, assess gait, and arrange follow-up
- Order MRI of the brain immediately
- Delay all intervention until a fracture occurs
- A: Tempting because simple counseling seems efficient; wrong because it lacks a concrete risk-reduction plan or follow-up.
- B: Tempting because it is multi-step; correct because it targets modifiable contributors and includes monitoring.
- C: Tempting because falls can reflect neurologic disease; wrong because no red flag suggests immediate neuroimaging in this stable scenario.
- D: Tempting because some learners wait for objective harm; wrong because prevention acts before the complication occurs.
Answer: B
Exam takeaway: Strong prevention answers combine a targeted intervention, practical support, and a follow-up checkpoint.
flowchart LR A[Identify highest-yield modifiable risk] --> B[Choose one priority intervention] B --> C[Add environmental or medication safety step] C --> D[Set measurable goal] D --> E[Arrange follow-up] E --> F[Escalate if red flags emerge]
1.1.1.7 Prevention boundaries: when not to stay in the routine lane
A Explanation
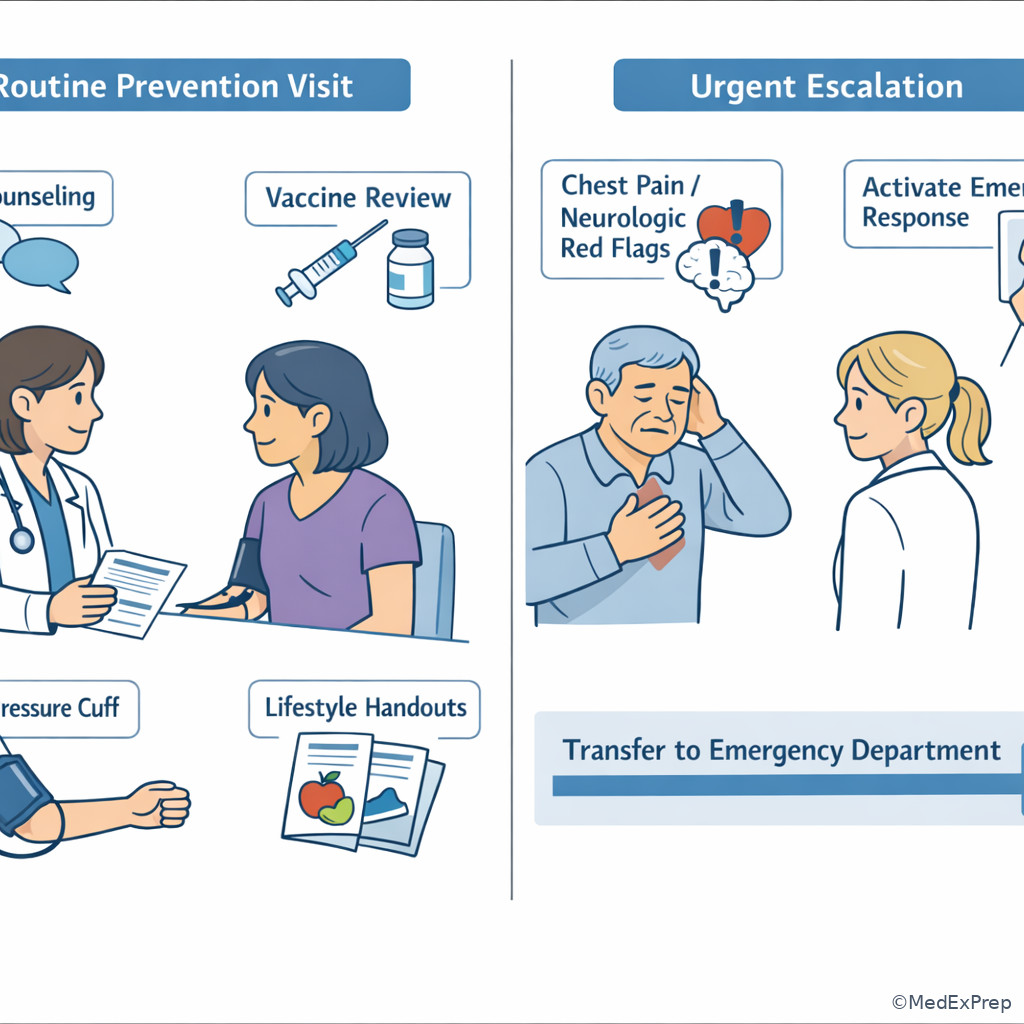
The decision conflict is whether the best answer remains a preventive outpatient intervention or whether the patient has crossed into urgent assessment, specialist referral, or emergency transfer. The single rule is that prevention applies to stable patients; instability, new focal deficits, severe symptoms, or time-sensitive threats override routine prevention priorities.
WHY THIS IS TESTED: board questions assess safe role boundaries. FNP candidates must recognize when the correct action is escalation, not office-based prevention.
Choose escalation over prevention when there are red flags such as chest pain concerning for ACS, stroke symptoms, severe dyspnea, suicidal intent, syncope with high-risk features, severe dehydration, anaphylaxis, sepsis concern, GI bleeding, or sudden neurologic deficit. In these cases, you are no longer mainly reducing long-term risk; you are preventing immediate harm by urgent triage. This still fits a prevention mindset broadly, but the board answer becomes transfer, ED referral, or same-day urgent evaluation. Reject low-priority counseling at the moment of instability.
Quaternary prevention also appears here: avoid unnecessary screening or counseling detours when a dangerous symptom needs action now. For example, do not spend the visit on smoking cessation alone if the patient has exertional chest pressure and diaphoresis. See Fig 5 for the escalation framework.
Exam takeaway: A red flag changes the setting and urgency before any routine prevention plan is considered.
B Worked example
A 59-year-old man presents for a wellness visit. He has tobacco use disorder, hyperlipidemia, obesity, and poor appointment adherence. While rooming, he mentions “heartburn” for two days that worsens when he walks from the parking lot and improves with rest. He is mildly diaphoretic and says he nearly canceled because he did not want another lecture about smoking. His pulse is 108/min and BP is 154/96 mm Hg. The task is to choose the most appropriate next step.
Reasoning chain: identify task → not routine prevention anymore. Extract key facts: exertional chest discomfort, diaphoresis, tachycardia, multiple ASCVD risks. Apply rule: red flag symptoms concerning for ACS override wellness counseling. Eliminate distractors: smoking cessation counseling and lipid management are important but not the priority; outpatient stress-test ordering delays urgent evaluation. Verify: immediate emergency referral/activation of emergency response is the safest FNP action.
C Exam trap
D Checkpoint
Question: Which presentation most clearly requires moving out of the routine prevention lane?
- Asymptomatic 52-year-old due for colorectal screening
- 17-year-old seeking counseling on vaping cessation
- 68-year-old with near-syncope, new unilateral weakness, and slurred speech in clinic
- 34-year-old asking about diet changes for migraine prevention
- A: Tempting because screening can feel urgent; wrong because this is stable preventive care.
- B: Tempting because nicotine use has real risks; wrong because this remains routine outpatient counseling.
- C: Tempting because prevention after stroke matters; correct because the patient has acute stroke red flags requiring emergency action now.
- D: Tempting because migraines can impair function; wrong because this is stable risk-reduction counseling.
Answer: C
Exam takeaway: When red flags appear during a preventive visit, the correct FNP action is triage and escalation, not routine counseling.
- The stem phrase that should trigger escalation over prevention is acute red flag.
- True or False: A wellness visit label means the answer must be a preventive action. False.
- Name 3 red-flag categories that end routine prevention: cardiopulmonary instability, acute neurologic deficit, severe safety/psychiatric risk.
1.1.1.8 Quaternary prevention: avoiding harm from overuse
A Explanation
The decision conflict is whether doing more helps the patient or whether the safer answer is to avoid unnecessary testing, treatment, or labeling. The single rule: quaternary prevention applies when an intervention is unlikely to benefit this patient and may create harm, anxiety, false positives, cost, or cascades of unnecessary care.
WHY THIS IS TESTED: FNP boards do not just reward action; they reward safe, evidence-informed restraint.
Choose quaternary prevention when the question pushes overscreening, duplicate testing, antibiotics for clearly viral illness, imaging without red flags, or continuing burdensome screening in patients unlikely to benefit. This is not “doing nothing.” It is doing the safer thing: counseling, observation, shared decision-making, or avoiding low-value care. Reject the instinct that more testing is always safer. In primary care, false positives create real downstream harm.
This concept will connect directly to the next topic on screening test selection. For now, remember the board rule: if the test is not indicated, the preventive act may be to decline it and explain why. See Fig 6.
Exam takeaway: When a test or treatment has low expected benefit and meaningful downside, the safest answer may be to avoid it.
B Worked example
A 29-year-old healthy woman requests a “full-body CT scan” because her coworker was recently diagnosed with cancer. She has no symptoms, no major family history, normal exam findings, and no known exposures. She also asks whether antibiotics can “prevent sinus infections” because she gets one cold most winters. The task is to choose the best preventive response.
Reasoning chain: identify task → avoid harm from low-value care. Extract key facts: asymptomatic, average risk, anxiety-driven request, no indication for broad imaging, no current bacterial infection. Apply rule: quaternary prevention avoids unnecessary testing and treatment that can cause false positives and adverse effects. Eliminate distractors: ordering imaging feels proactive but is not indicated; prophylactic antibiotics create risk without benefit in this scenario. Verify: provide reassurance, targeted counseling, and use evidence-based indicated preventive care only.
C Exam trap
D Checkpoint
Question: Which action best represents quaternary prevention?
- Administering HPV vaccine to an eligible adolescent
- Ordering a screening mammogram for an asymptomatic patient who meets criteria
- Avoiding unnecessary imaging for uncomplicated low back pain without red flags
- Performing annual retinal exams in a patient with diabetes
- A: Tempting because it prevents future disease; wrong because this is primary prevention.
- B: Tempting because it is preventive; wrong because this is secondary prevention.
- C: Tempting because it seems like withholding care; correct because it avoids low-value intervention and potential harm.
- D: Tempting because complication prevention is preventive; wrong because this is tertiary prevention.
Answer: C
Exam takeaway: Not every patient benefits from more testing; low-value care can become preventable harm.
flowchart TD
A[Patient requests test or treatment] --> B{Indicated for age/risk/symptoms?}
B -->|Yes| C[Proceed with evidence-based prevention]
B -->|No| D[Explain low benefit]
D --> E[Discuss harms: false positives side effects cost]
E --> F[Offer appropriate counseling or watchful waiting] Exam takeaway: Quaternary prevention often requires clear explanation of why an unnecessary test may do more harm than good.
Exam Traps & Differentiators
| Looks similar | Actually means | How to separate on the exam |
|---|---|---|
| Risk factor present | Primary prevention target | No diagnosis yet; counseling, vaccine, exposure reduction |
| Asymptomatic but due for test | Secondary prevention | Screen for silent disease, not for symptoms |
| Known chronic disease | Tertiary prevention | Prevent complications and disability |
| Requested low-yield test | Quaternary prevention | Avoid unnecessary harm, cost, and false positives |
| Acute severe symptom | Urgent escalation | Red flag overrides routine prevention |
If the stem says “strong family history but no symptoms,” think risk stratification, not diagnosis.
If the stem says “asymptomatic and due for age-based testing,” think screening and secondary prevention.
If the stem says “already has diabetes/COPD/CKD,” think tertiary prevention and complication reduction.
If the stem says “wants every test possible,” think quaternary prevention and evidence-based restraint.
If the stem says “chest pain, focal deficits, severe dyspnea, suicidality,” think triage and escalation, not routine health promotion.
If the stem says “annual wellness visit” but then adds an unstable finding, think the visit type is a distractor.
| Commonly confused pair | Tempting wrong choice | Single clue that breaks the tie |
|---|---|---|
| Primary vs Secondary prevention | Ordering a screening test instead of counseling | Question asks to lower future risk, not detect silent disease |
| Secondary vs Tertiary prevention | Calling routine monitoring “screening” in known disease | The diagnosis is already established |
| Tertiary vs urgent escalation | Outpatient chronic management during acute instability | Presence of red-flag symptoms |
| Patient-centered care vs overtesting | Ordering requested low-value imaging | Average-risk asymptomatic patient |
Forward link: in the upcoming topic Screening Principles and Test Selection, these traps become more specific: the stem will ask not just “which prevention level?” but “which test, for whom, and why.” Another upcoming confusable pair is from Behavioral Counseling in Primary Care: the right counseling target may be obvious, but the test will ask for the best interviewing approach or readiness-to-change step.
Algorithm / Approach
Exam takeaway: Classify the patient first, then choose counseling, screening, complication prevention, or escalation.
| Situation | Best FNP framing | What to do | What to avoid |
|---|---|---|---|
| Healthy patient with modifiable risk | Primary prevention | Counsel, immunize, reduce exposure | Jumping straight to broad testing |
| Asymptomatic patient due for test | Secondary prevention | Choose indicated screening | Using diagnostic workup language |
| Known chronic disease | Tertiary prevention | Monitor and prevent complications | Calling routine monitoring “screening” |
| Low-value requested test | Quaternary prevention | Explain harms and use shared decision-making | Testing for reassurance alone |
| Unstable or red-flag presentation | Escalation | Urgent referral or ED transfer | Continuing routine wellness agenda |
Rapid Review
- Primary prevention → lowers disease incidence before diagnosis exists
- Secondary prevention → detects silent disease in asymptomatic patients
- Tertiary prevention → limits complications after diagnosis is established
- Quaternary prevention → protects patients from low-value medical harm
- Family history → risk stratifier, not a modifiable target
- Smoking → classic modifiable risk requiring direct intervention
- Wellness visit with red flags → triage problem, not prevention problem
- Age-based priorities → start framework; individual risk factors refine it
- Older adult near fall + sedating medication → falls/medication safety focus
- Requested unnecessary test → patient-centered explanation, not automatic ordering
- Known diabetes + retinal exam → tertiary, not secondary prevention
- Asymptomatic due-for-test stem → screening principle likely coming next
- General advice alone → weaker than a measurable plan with follow-up
- Board trap → screening and prevention are related but not interchangeable
Self-check quiz
1. A 24-year-old healthy graduate student presents for a routine visit. She has no chronic conditions, takes no medications, and asks whether receiving an indicated vaccine at today’s visit is considered which level of prevention?
- Primary prevention
- Secondary prevention
- Tertiary prevention
- Quaternary prevention
2. A 57-year-old asymptomatic man with obesity and hypertension asks why he is being offered a recommended screening test even though he feels well. Which prevention level best fits this situation?
- Primary prevention
- Secondary prevention
- Tertiary prevention
- Quaternary prevention
3. A 46-year-old woman presents for an annual visit. She has obesity, PCOS, and a father with type 2 diabetes. She has no polyuria or weight loss. She asks what step is most appropriate to reduce her future diabetes risk. Which action is best?
- Begin home glucose checks four times daily
- Focus on nutrition, physical activity, and weight-related counseling with follow-up
- Manage her as if she already has diabetes because of family history
- Delay intervention until laboratory evidence of diabetes appears
4. A 73-year-old man with osteoarthritis, insomnia, and benign prostatic hyperplasia presents for follow-up. He takes diphenhydramine nightly and reports two recent near falls when getting up to use the bathroom. He also wants advice about “boosting immunity.” Which is the most appropriate preventive priority?
- Recommend a multivitamin first because he asked about immunity
- Review sedating medications, assess fall risk, and address home safety
- Wait for a documented fracture before changing the plan
- Order whole-body imaging to look for hidden causes of falls
5. A 31-year-old healthy man requests annual chest CT imaging because a coworker was recently diagnosed with lung cancer. He has never smoked, has no symptoms, and no major family history. Which response best reflects quaternary prevention?
- Order the CT because patient reassurance is the highest priority
- Explain that unnecessary imaging can cause harm and focus on indicated prevention instead
- Prescribe antibiotics in case a hidden infection is present
- Repeat imaging every year to establish a baseline
6. A 61-year-old woman comes for a wellness visit. She has type 2 diabetes, CKD stage 3, hyperlipidemia, and tobacco use disorder. While discussing diet, she reports new exertional chest pressure for three days and feels mildly nauseated. Which is the most appropriate next step?
- Intensify lipid counseling and arrange routine cardiology referral
- Provide smoking cessation counseling and schedule close follow-up next week
- Arrange urgent emergency evaluation because the visit has shifted out of preventive care
- Order outpatient screening tests and continue the wellness agenda
7. A 68-year-old man with known COPD, hypertension, and prior tobacco use presents for follow-up. He is stable and asks whether his inhaler review, vaccination update, and pulmonary rehabilitation discussion count as screening. Which prevention framing is best?
- Secondary prevention because COPD can worsen silently
- Tertiary prevention because the disease is already established and the goal is reducing complications
- Primary prevention because vaccines are always primary prevention no matter the overall plan
- Quaternary prevention because adding care always increases burden
8. A 52-year-old woman with obesity, family history of premature ASCVD, and controlled hypertension presents for preventive care. She is asymptomatic and asks for “every heart test available,” including coronary CT, stress testing, and carotid ultrasound. Which response is most appropriate?
- Order all requested tests because her family history makes any testing reasonable
- Decline all prevention since she is asymptomatic
- Use risk-based counseling and indicated preventive strategies while avoiding nonindicated tests
- Send her to the ED because premature family history is a cardiovascular emergency
Answer key
1.1.1.9 1. Answer: A
A. Primary prevention: Tempting because vaccines are the classic prevention example; correct because they act before disease occurs. Single stem clue: healthy patient receiving an indicated vaccine with no disease present.
B. Secondary prevention: Tempting because it is also preventive; incorrect because secondary prevention requires detection of silent disease, usually via screening. Single stem clue: no screening test is being performed.
C. Tertiary prevention: Tempting because prevention can still help people with disease; incorrect because there is no established diagnosis to manage. Single stem clue: patient is healthy and has no chronic condition mentioned.
D. Quaternary prevention: Tempting because avoiding harm is also preventive; incorrect because the intervention is clearly indicated and beneficial rather than low-value. Single stem clue: indicated vaccine, not unnecessary care.
1.1.1.10 2. Answer: B
A. Primary prevention: Tempting because obesity and hypertension are risk factors; incorrect because the question emphasizes a screening test in an asymptomatic person. Single stem clue: “feels well” but is being offered screening.
B. Secondary prevention: Tempting because many learners associate screening with prevention only generally; correct because recommended screening in an asymptomatic patient is secondary prevention. Single stem clue: asymptomatic patient due for testing.
C. Tertiary prevention: Tempting because hypertension is already present; incorrect because the stem asks specifically about the offered screening test, not management of known disease. Single stem clue: focus on screening, not complication management.
D. Quaternary prevention: Tempting because not all tests are useful; incorrect because the stem says recommended screening, implying it is indicated. Single stem clue: indicated rather than unnecessary test.
1.1.1.11 3. Answer: B
A. Begin home glucose checks four times daily: Tempting because diabetes risk is high and monitoring sounds proactive; incorrect because she has no diagnosis of diabetes and no indication for intensive self-monitoring. Single stem clue: no symptoms or confirmed disease.
B. Focus on nutrition, physical activity, and weight-related counseling with follow-up: Tempting because it sounds basic; correct because primary prevention targets modifiable risk before disease develops. Single stem clue: risk factors present without diabetes diagnosis.
C. Manage her as if she already has diabetes because of family history: Tempting because PCOS and family history raise risk; incorrect because risk does not equal diagnosis. Single stem clue: no polyuria, no weight loss, no confirmed diabetes.
D. Delay intervention until laboratory evidence of diabetes appears: Tempting because definitive diagnosis matters; incorrect because prevention should occur before disease is established. Single stem clue: question asks how to reduce future risk now.
1.1.1.12 4. Answer: B
A. Recommend a multivitamin first because he asked about immunity: Tempting because patient agenda matters and vitamins sound preventive; incorrect because the dominant immediate preventable harm is falls risk. Single stem clue: recent near falls plus nightly diphenhydramine.
B. Review sedating medications, assess fall risk, and address home safety: Tempting because it is more involved; correct because older adult prevention prioritizes function, falls, and medication safety. Single stem clue: sedating medication and near falls.
C. Wait for a documented fracture before changing the plan: Tempting because objective injury would confirm severity; incorrect because prevention acts before harm occurs. Single stem clue: near falls already signal modifiable risk.
D. Order whole-body imaging to look for hidden causes of falls: Tempting because falls can have serious etiologies; incorrect because no focal neurologic red flags or acute trauma justify broad imaging. Single stem clue: clear modifiable contributors are already present.
1.1.1.13 5. Answer: B
A. Order the CT because patient reassurance is the highest priority: Tempting because patient-centered care includes addressing anxiety; incorrect because unnecessary imaging exposes the patient to potential harm without clear benefit. Single stem clue: asymptomatic average-risk nonsmoker.
B. Explain that unnecessary imaging can cause harm and focus on indicated prevention instead: Tempting because it may feel less satisfying than ordering a test; correct because this is quaternary prevention. Single stem clue: requested nonindicated imaging.
C. Prescribe antibiotics in case a hidden infection is present: Tempting because some patients equate treatment with prevention; incorrect because there is no evidence of infection, and antibiotics can cause harm. Single stem clue: healthy, asymptomatic patient.
D. Repeat imaging every year to establish a baseline: Tempting because baselines sound prudent; incorrect because repeated nonindicated testing amplifies harm and cost. Single stem clue: no clinical indication exists even once.
1.1.1.14 6. Answer: C
A. Intensify lipid counseling and arrange routine cardiology referral: Tempting because she is high-risk and cardiology involvement may be reasonable later; incorrect because routine referral is too slow when new exertional chest pressure and nausea raise concern for ACS. Single stem clue: new exertional chest symptoms during the visit.
B. Provide smoking cessation counseling and schedule close follow-up next week: Tempting because tobacco use is a key modifiable risk and counseling belongs in prevention; incorrect because acute symptoms override long-term counseling priorities. Single stem clue: possible unstable cardiac presentation now.
C. Arrange urgent emergency evaluation because the visit has shifted out of preventive care: Tempting because it may seem aggressive in a wellness visit; correct because red flags change the setting and urgency. Single stem clue: exertional chest pressure plus nausea in a high-risk patient.
D. Order outpatient screening tests and continue the wellness agenda: Tempting because preventive visits often involve testing; incorrect because screening is inappropriate when the patient may have an acute symptomatic condition. Single stem clue: symptomatic, not asymptomatic.
1.1.1.15 7. Answer: B
A. Secondary prevention because COPD can worsen silently: Tempting because monitoring often happens before severe symptoms worsen; incorrect because the disease is already known, so the task is not screening for hidden disease. Single stem clue: known COPD.
B. Tertiary prevention because the disease is already established and the goal is reducing complications: Tempting because multiple services are being discussed; correct because inhaler review, vaccination in context of chronic disease management, and pulmonary rehabilitation all reduce morbidity in established disease. Single stem clue: diagnosed COPD with stable follow-up care.
C. Primary prevention because vaccines are always primary prevention no matter the overall plan: Tempting because vaccines are classically primary prevention; incorrect for the overall framing of the visit because the central plan is complication reduction in known disease. Single stem clue: comprehensive COPD follow-up rather than isolated vaccine counseling.
D. Quaternary prevention because adding care always increases burden: Tempting because overuse is a real concern; incorrect because these interventions are indicated and high-value. Single stem clue: evidence-based care in established disease, not low-value excess.
1.1.1.16 8. Answer: C
A. Order all requested tests because her family history makes any testing reasonable: Tempting because family history increases concern and the patient is anxious; incorrect because risk stratification does not justify every possible test. Single stem clue: asymptomatic patient requesting broad nonindicated testing.
B. Decline all prevention since she is asymptomatic: Tempting because unnecessary testing should be avoided; incorrect because she still needs risk-based counseling and indicated preventive care. Single stem clue: asymptomatic does not mean prevention stops.
C. Use risk-based counseling and indicated preventive strategies while avoiding nonindicated tests: Tempting because it requires nuance rather than a simple yes/no answer; correct because it combines primary prevention and quaternary prevention appropriately. Single stem clue: risk factors present without symptoms, alongside requests for excessive testing.
D. Send her to the ED because premature family history is a cardiovascular emergency: Tempting because premature ASCVD family history is serious; incorrect because family history alone without symptoms is not an emergency. Single stem clue: asymptomatic and stable presentation.