Why it matters
- ExCPT questions often test the safest next step, not just a fact. Scope boundaries decide when you continue workflow and when you stop.
- Many realistic distractors are tasks a technician can help with operationally but cannot decide independently.
- Boundary mistakes create patient-safety, legal, and audit problems even when the data entry itself is accurate.
- Knowing scope protects both the patient and the technician: when clinical judgment appears, escalate.
Key Terms & Must-Know Facts
1.1.1.1 Key terms
- Scope of practice: tasks legally and professionally allowed for the technician role.
- Pharmacist verification: final check performed by the pharmacist before dispensing.
- Prospective drug review: pharmacist assessment for interactions, allergies, duplication, dose concerns, and appropriateness.
- Escalation: routing an issue to the pharmacist rather than resolving it independently.
- Data entry: entering prescription information exactly as authorized.
- Clarification: obtaining correction of missing, conflicting, or unclear order details through proper channels.
- Counseling: patient education about use, effects, precautions, and expectations; pharmacist role.
- Therapeutic substitution: changing one drug to another based on clinical reasoning or policy; not a technician decision.
- Refill authorization: approval to dispense additional fills; limited by law, prescriber instructions, and workflow rules.
- Controlled substance: medication regulated under federal and state controlled substance law.
- Audit trail: documented record of who entered, changed, prepared, or handled an order.
- Red flag: a clue that requires stopping and routing to the pharmacist.
1.1.1.2 Must-know facts
- Technicians may support workflow; they do not make independent clinical judgments.
- When the question asks about allergies, interactions, contraindications, unusual dosing, or counseling, escalate to the pharmacist.
- Technicians can enter routine prescription information, prepare products, label, package, and document under supervision.
- Technicians do not perform final prescription verification.
- If order details conflict with product selection or labeling, stop and route the issue.
- State law and site policy may vary; exam-safe action is to choose the safest compliant action and defer pharmacist-only decisions.
- Being “familiar” with the medication does not expand technician scope.
- A patient asking a clinical question is an escalation cue, not a customer-service exception.
Core content
1.1.1.3 Foundational boundary: support the process, not the clinical decision
A Explanation
The first technician-vs-pharmacist conflict is simple: Can I carry out the workflow step, or does this step require clinical or legal judgment? The resolving rule is: if the task is operational and based on authorized information, the technician may usually assist; if the task requires deciding whether therapy is appropriate, safe, substituted, counseled, or finally verified, the technician must stop and refer.
WHY THIS IS TESTED: Exam writers like to present routine workflow details that make the technician feel “close enough” to the decision. The tested pattern is whether you can separate handling information from interpreting it clinically.
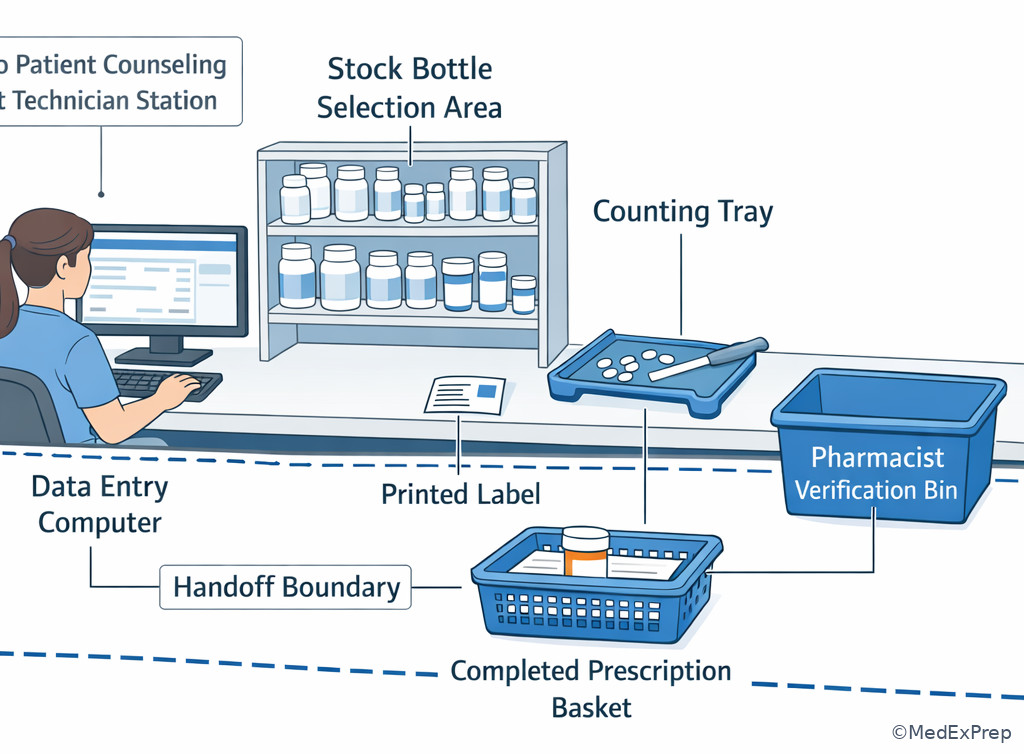
Examples of technician-permitted support tasks include receiving routine written information for processing, entering patient and prescriber data, typing the sig exactly as authorized, calculating quantity or days' supply, selecting the matched stock bottle for pharmacist check, printing labels, packaging, documenting, and managing inventory steps. Examples to reject as technician decisions include changing a drug because one product is out of stock, deciding whether a dose is appropriate, telling the patient how to use a medication clinically, deciding whether an interaction matters, or releasing a prescription after your own final check.
The key exam move is choose process, reject judgment. See Fig 1.
Exam takeaway: Separate operational workflow tasks from any step requiring clinical judgment, counseling, or final verification.
flowchart TD
A[Task appears in workflow] --> B{Operational or judgment-based?}
B -->|Operational| C[Enter, prepare, label, document]
B -->|Judgment-based| D[Pause and refer]
D --> E[Pharmacist evaluates safety legality appropriateness]
C --> F[Present for pharmacist verification] B Worked example
A 67-year-old patient with diabetes and chronic kidney disease drops off lisinopril 40 mg tablets, 1 tablet by mouth daily, quantity 90. The patient also says, “I used to take losartan, but this probably does the same thing, right?” The profile shows an old cough note, and the technician notices the patient is also picking up metformin. The question asks for the most appropriate technician action.
Identify task: The task is not to compare ACE inhibitors and ARBs; it is to decide what the technician may do. Extract key facts: Valid medication context is present; the patient is asking a counseling/therapy-comparison question; the cough note is a distracting clue that may matter clinically but is not for technician resolution. Apply rule: A technician may enter the prescription and prepare it for review, but must refer the patient’s therapeutic question to the pharmacist. Eliminate distractors: Reject any option that says to reassure the patient that lisinopril and losartan are equivalent, to explain cough risk, or to change the product based on prior therapy. Verify: Continue permitted processing and route the counseling question.
C Exam trap
D Checkpoint
Question: A technician receives a prescription for amoxicillin 500 mg capsules, take 1 capsule by mouth three times daily for 10 days, quantity 30. The patient asks whether it is safe to take with warfarin. Which action is most appropriate?
- Enter the prescription, tell the patient it is usually fine, and offer to call if a problem appears later.
- Enter the prescription and refer the interaction question to the pharmacist before completion.
- Refuse to process the prescription until the patient contacts the prescriber independently.
- Change the sig to twice daily because that schedule is easier for adherence.
Answer: B
- A: Tempting because technicians often field first-line patient questions; wrong because interaction assessment and counseling are pharmacist tasks.
- B: Tempting because it may feel slower; right because routine processing may continue while the pharmacist addresses the clinical question.
- C: Tempting because escalation is needed; wrong because the technician should route the issue through pharmacy workflow, not abandon processing without reason.
- D: Tempting because adherence concerns sound practical; wrong because changing directions is unauthorized and outside technician scope.
1.1.1.4 Workflow permissions: what a technician may do before pharmacist verification
A Explanation
Another tested conflict is “I touched the prescription, so did I also approve it?” No. The resolving rule is that technicians can perform many preparatory steps, but the pharmacist performs final verification and clinical review. The exam will often place data entry, counting, label printing, or stock selection next to language like “release,” “verify,” or “approve.” The single clue is whether the step is a support step or a final authorization step.
WHY THIS IS TESTED: This pattern mirrors real workflow. Many errors happen when someone treats a preparatory check as if it replaces pharmacist verification.
Technician tasks before verification commonly include receiving the written or electronic order for processing, entering drug/strength/dosage form/quantity/refills as written, pulling the correct stock bottle by NDC match, counting or measuring, affixing labels, packaging, and staging the filled prescription. None of those actions equal final verification. A technician may catch a problem, but the technician does not resolve pharmacist-only concerns independently. See Fig 2.
Exam takeaway: Technician work can move the prescription forward, but final verification remains a pharmacist-only checkpoint.
flowchart LR A[Receive order] --> B[Enter data] B --> C[Select product] C --> D[Prepare and label] D --> E[Stage for check] E --> F[Pharmacist verifies] F --> G[Dispense per workflow]
Exam takeaway: Visualize where technician preparation ends and pharmacist verification begins in the dispensing workflow.
B Worked example
In a busy outpatient setting, a 44-year-old patient with asthma and hypertension is waiting for albuterol HFA 90 mcg/actuation, inhale 2 puffs every 4 to 6 hours as needed, quantity 1 inhaler. The technician has entered the data, selected the correct inhaler, and printed the label. A coworker says, “You already checked the NDC and quantity, so go ahead and hand it out.” The patient also asks whether a spacer is required.
Identify task: Decide whether the technician can release the medication and answer the device-use question. Extract key facts: The technician completed preparation tasks; final verification has not been mentioned; the spacer question is counseling noise. Apply rule: Technician preparation is not final verification, and inhaler-use counseling belongs to the pharmacist. Eliminate distractors: Reject any option allowing direct release because the “hard part is done.” Reject options allowing device counseling because it sounds basic. Verify: Stage for pharmacist check and refer the patient’s use question.
C Exam trap
D Checkpoint
Question: A technician has counted metformin 500 mg tablets, labeled the bottle, and placed it in a will-call bin before pharmacist review during a rush. Which statement best identifies the problem?
- This is acceptable because metformin is not a controlled substance.
- This is acceptable if the patient has filled it before.
- This is not acceptable because final verification cannot be bypassed.
- This is not acceptable only if the quantity exceeds 30 tablets.
Answer: C
- A: Tempting because controlled-substance rules are strict; wrong because verification rules apply beyond controlled drugs.
- B: Tempting because refill familiarity lowers perceived risk; wrong because prior use does not replace final verification.
- C: Tempting because it sounds absolute; right because the issue is bypassing pharmacist review.
- D: Tempting because quantity checks matter operationally; wrong because the error is the skipped handoff, not tablet count.
- True or False: A correct NDC match allows the technician to bypass pharmacist verification. False.
- The final step before dispensing that a technician cannot perform is pharmacist verification.
- Name 3 technician support tasks before verification: data entry, product selection, labeling.
1.1.1.5 Escalation triggers: when the safest action is to pause and route
A Explanation
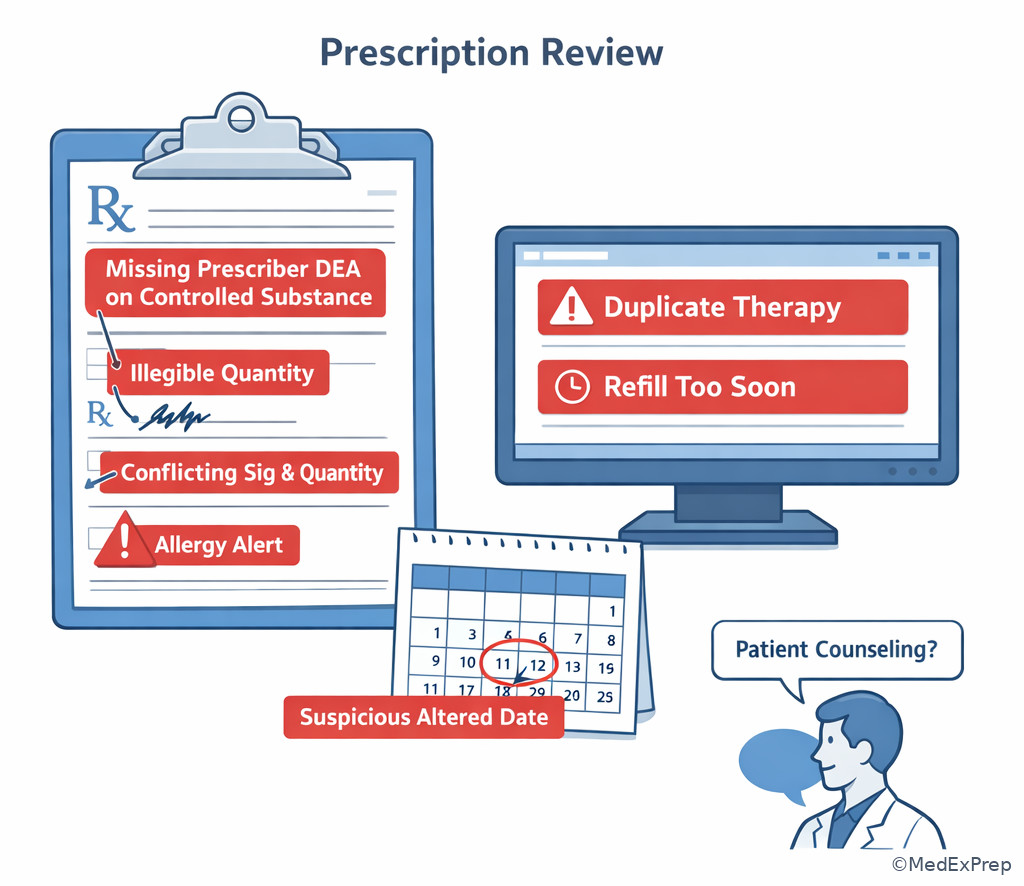
The next boundary question is not “what can I do?” but “when must I stop?” The resolving rule is that a technician should pause and escalate when the order or patient interaction introduces ambiguity, conflict, suspiciousness, missing required information, clinical risk signals, or a request that exceeds technician authority. The most tested categories are allergies, interactions, contraindications, odd doses, unclear directions, suspicious prescriptions, refill irregularities, and requests for counseling.
WHY THIS IS TESTED: ExCPT emphasizes patient safety and legality. The exam often builds a scenario where much of the order looks normal, but one clue flips the correct answer from “continue” to “pause.”
Use a red-flag mindset: if there is conflict, missing information, or a request for interpretation, do not improvise. A technician may notice and document the problem; the technician should not independently decide whether the problem is harmless. See Fig 3. In the next topic, Escalation Trigger Recognition, you will build a more detailed red-flag checklist; here, the goal is to know that recognizing the trigger is part of scope boundaries.
Exam takeaway: One red-flag clue such as ambiguity, clinical concern, or suspicious details changes the technician action from process to pause and refer.
flowchart TD
A[Prescription or patient request] --> B{Any red flag?}
B -->|No| C[Continue routine processing]
B -->|Yes| D{What kind of red flag?}
D --> E[Clinical concern]
D --> F[Legal or documentation concern]
D --> G[Counseling request]
E --> H[Refer to pharmacist]
F --> H
G --> H Exam takeaway: Learn to spot missing, conflicting, and suspicious order elements before product preparation continues.
B Worked example
A 29-year-old patient in urgent care follow-up presents an electronic prescription for sulfamethoxazole/trimethoprim DS 800 mg/160 mg tablets, take 1 tablet by mouth twice daily for 7 days, quantity 14. The profile lists a sulfonamide allergy entered years ago, and the patient says, “It was probably just nausea.” She also asks whether she can drink alcohol while taking it. Her medication profile includes oral contraceptives and ibuprofen.
Identify task: Determine the technician’s next step, not whether the allergy is true or whether the antibiotic is clinically appropriate. Extract key facts: Allergy note exists; patient minimizes it; alcohol-use question is counseling; other medications are distracting. Apply rule: Allergy concerns and counseling requests are pharmacist-review issues. Eliminate distractors: Reject options that instruct the technician to remove the allergy note, decide it is intolerance rather than allergy, or counsel on alcohol use. Verify: Pause dispensing progression as needed and route to the pharmacist.
C Exam trap
D Checkpoint
Question: During data entry for clarithromycin 500 mg tablets, take 1 tablet by mouth twice daily for 10 days, a patient asks whether it will interfere with her heart medication. Which technician action is most appropriate?
- Answer if the technician has seen the combination before.
- Complete data entry and refer the interaction question to the pharmacist.
- Delete the order from the queue until the prescriber calls back.
- Tell the patient to skip the heart medication until the antibiotic is finished.
Answer: B
- A: Tempting because experience may create false confidence; wrong because interaction evaluation is a pharmacist function.
- B: Tempting because it balances workflow and safety; right because technicians can process routine information while routing the clinical concern.
- C: Tempting because stopping feels safe; wrong because technician escalation is to the pharmacist, not unilateral deletion.
- D: Tempting because it appears cautious; wrong because medication management advice is outside technician scope.
1.1.1.6 Communication boundaries: customer service is not counseling
A Explanation
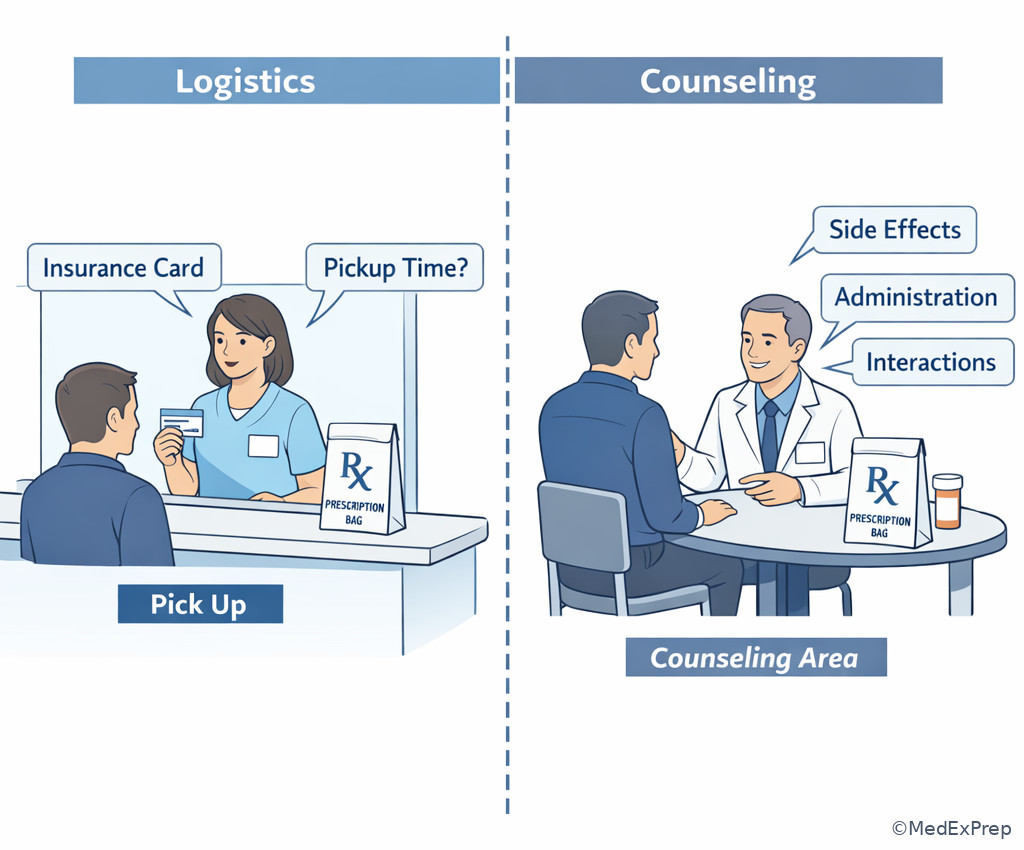
A common exam conflict is deciding whether the technician is doing normal communication or crossing into counseling. The resolving rule is: technicians may communicate nonclinical information for workflow coordination, but they may not explain therapeutic effect, side effects, administration strategy, interactions, warnings, or “whether it is okay” to use a medication in a clinical sense.
WHY THIS IS TESTED: Many stems disguise counseling as simple customer service. The testable pattern is whether the content of the conversation changes from logistics to clinical advice.
Technicians may ask for demographic updates, insurance cards, refill preferences, pickup timing, and nonclinical clarifications such as spelling of a name or whether an address changed. Technicians may tell a patient that the pharmacist will speak with them. Technicians may not tell a patient how to adjust insulin, whether drowsiness is expected, whether a rash is serious, how to use an inhaler properly in a clinical teaching sense, or whether a drug can be taken with another medication. See Fig 4.
Exam takeaway: Workflow communication stays with the technician, but medication-use advice and clinical interpretation go to the pharmacist.
flowchart TD
A[Patient asks question] --> B{Logistics or clinical?}
B -->|Logistics| C[Technician may assist]
B -->|Clinical use safety effect| D[Refer to pharmacist]
C --> E[Insurance pickup status demographics]
D --> F[Side effects interactions administration warnings] Exam takeaway: Distinguish nonclinical front-counter communication from pharmacist-only counseling topics.
B Worked example
A 58-year-old patient with COPD and osteoarthritis picks up tiotropium inhalation capsules, inhale contents of 1 capsule daily using device, quantity 30. While the technician is confirming address and copay, the patient says, “Do I swallow the capsule or put it in the inhaler? Also, will it make me shaky like albuterol?” The profile also shows a new discount card entry and a note about preferred language.
Identify task: Decide which parts of the interaction stay with the technician. Extract key facts: Address and copay are logistics; medication-use instructions and effect comparison are counseling; language preference is workflow-relevant but not the tested issue. Apply rule: Handle demographics/payment, then refer device-use and side-effect questions to the pharmacist. Eliminate distractors: Reject options that give inhaler instructions because the technician has seen the device before. Verify: Ensure a real handoff occurs rather than a vague suggestion.
C Exam trap
D Checkpoint
Question: Which patient request can the technician handle without escalating to the pharmacist?
- “Can I take this prednisone with ibuprofen?”
- “What side effects should I expect from sertraline 50 mg daily?”
- “Has my insurance claim for atorvastatin 20 mg once daily gone through yet?”
- “How should I adjust my insulin glargine dose if my sugars are low?”
Answer: C
- A: Tempting because it sounds like a common question; wrong because it asks about combined medication use.
- B: Tempting because common side effects may seem routine; wrong because side-effect counseling is pharmacist-only.
- C: Tempting because it sounds administrative; right because insurance status is nonclinical workflow communication.
- D: Tempting because insulin questions are common at pickup; wrong because dose adjustment is clearly beyond technician scope.
- True or False: A technician may answer whether a medication causes drowsiness if it is a common side effect. False.
- The technician may communicate pickup, payment, demographics, and claim status.
- Name the boundary line: logistics = technician; medication advice = pharmacist.
1.1.1.7 Legal and safety edges: refills, substitutions, and controlled-substance boundaries
A Explanation
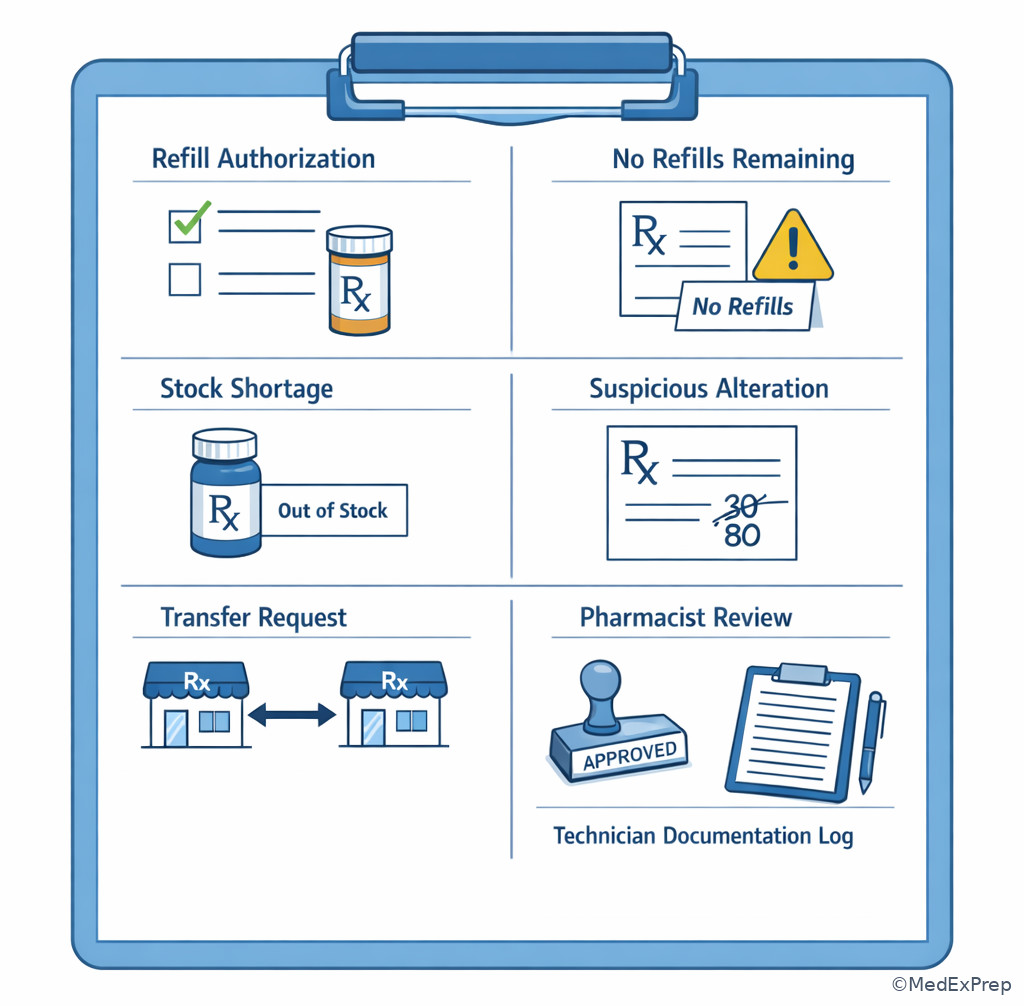
The highest-yield integration questions combine scope with legal restrictions. The conflict is often between keeping workflow moving and crossing a legal line. The resolving rule is: technicians may process according to authorized refills, documented policy, and pharmacist supervision, but may not independently authorize refills beyond what is permitted, accept or alter prohibited controlled-substance information, perform therapeutic substitution, or override documentation requirements for convenience.
WHY THIS IS TESTED: These are realistic pressure points in practice. Stems often create time pressure or patient urgency to tempt an unsafe shortcut.
Examples: if there are no refills remaining, the technician should not “lend a few tablets” unless a compliant policy and pharmacist authorization exist. If a patient asks for a different strength because the usual one is out of stock, the technician cannot select an alternative strength or dosage form independently. If a controlled prescription appears altered or missing required information, the technician should stop and route it. If a transfer, refill, or verbal order raises legal questions, choose the safest technician-level action: document, hold, and refer. See Fig 5.
Exam takeaway: Urgency, stock shortages, or refill requests do not allow technicians to bypass refill limits, substitution rules, or controlled-substance safeguards.
flowchart TD
A[Patient or order request] --> B{Refill? substitution? controlled issue?}
B --> C[Authorized routine processing]
B --> D[Outside authorization or suspicious]
D --> E[Do not modify or approve]
E --> F[Escalate and document]
C --> G[Continue within policy] Exam takeaway: Use legal checkpoints for refill limits, suspicious changes, stock shortages, and documentation gaps.
B Worked example
A 73-year-old patient with chronic pain and insomnia requests an early refill of zolpidem 10 mg tablets, take 1 tablet by mouth at bedtime, quantity 30. The system shows no refills remaining. The patient says she is traveling for a family emergency and asks the technician to “just give three tablets to cover the weekend.” She also mentions she has used the same pharmacy for years and offers to pay cash. The office is closed.
Identify task: Decide the technician’s most appropriate next step. Extract key facts: No refills remain; patient urgency and loyalty are noise; cash payment does not solve authorization; the medication is controlled in many settings and is legally sensitive. Apply rule: The technician cannot independently authorize additional tablets or override refill restrictions. Eliminate distractors: Reject “give a few tablets,” “change quantity,” or “switch to a lower strength temporarily.” Verify: Route to the pharmacist and document the request per workflow.
C Exam trap
D Checkpoint
Question: A patient presents a prescription for oxycodone/acetaminophen 5 mg/325 mg, 1 tablet by mouth every 6 hours as needed, quantity 20. The written quantity appears overwritten from “10” to “20.” What is the most appropriate technician action?
- Process it as 20 because the larger number is easier to read.
- Ask the patient which quantity the prescriber intended.
- Pause processing and route the suspicious alteration to the pharmacist.
- Process it as 10 to be conservative.
Answer: C
- A: Tempting because readability seems practical; wrong because suspicious controlled details require review.
- B: Tempting because the patient may know the plan; wrong because patient preference cannot resolve a suspicious prescription issue.
- C: Tempting because it slows the line; right because altered or suspicious information is a stop-and-escalate event.
- D: Tempting because smaller quantity seems safer; wrong because guessing still exceeds technician authority.
1.1.1.8 Best-answer strategy: how ExCPT tests scope boundaries
A Explanation
The final integration skill is test-taking under scope pressure. The conflict is between a technically possible action and the safest technician-level action. The resolving rule is to scan the stem for boundary words: counsel, verify, change, recommend, determine appropriateness, clarify unusual dose, interaction, allergy, suspicious, no refills remaining. If the action asks you to decide rather than process, escalate.
WHY THIS IS TESTED: ExCPT rewards safe judgment within technician scope. The best answer is often not the fastest workflow move, but the one that preserves safety, legality, and chain of responsibility.
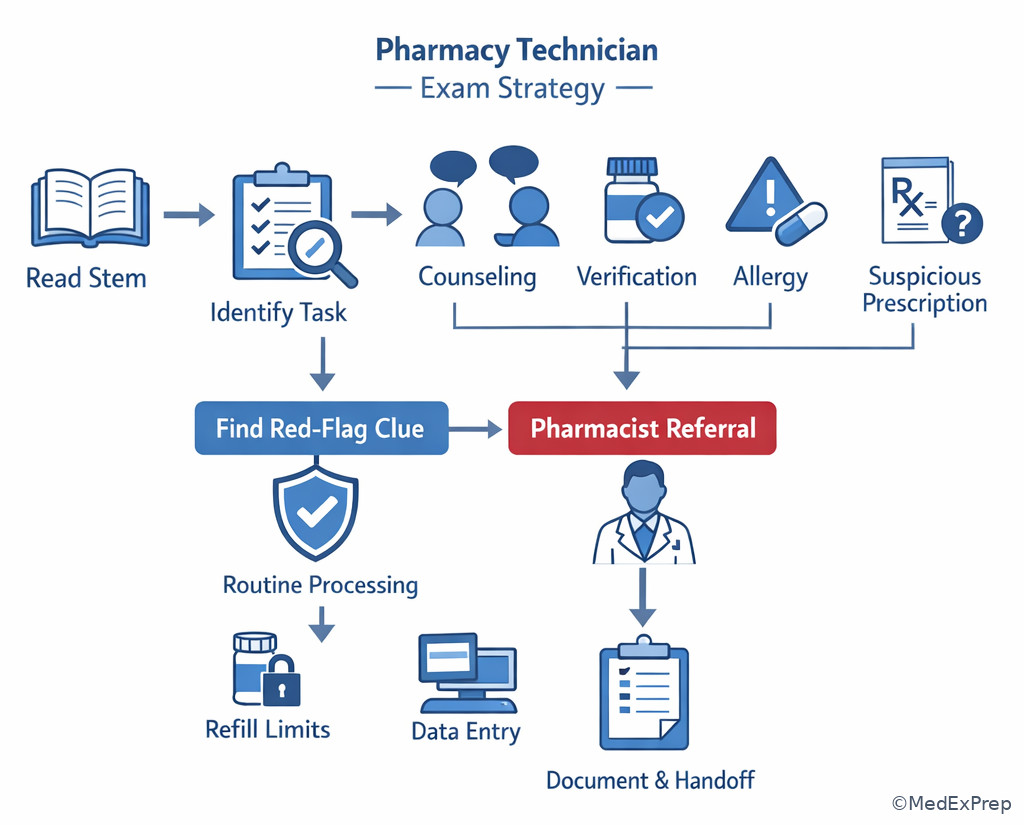
Use this exam sequence: identify the task, strip out noise, find the single red-flag clue, choose process vs pause, then select the option that preserves pharmacist review where required. See Fig 6. This section connects directly to the upcoming topics on workflow sequence and escalation recognition.
Exam takeaway: In technician-scope questions, identify the one clue that turns a routine workflow step into a required pharmacist referral.
flowchart LR
A[Read stem] --> B[Identify exact task]
B --> C[Find red flag or judgment word]
C --> D{Routine processing?}
D -->|Yes| E[Continue within policy]
D -->|No| F[Pause refer document]
F --> G[Choose safest next step] Exam takeaway: Reduce technician-boundary questions to a consistent identify-process-escalate framework.
B Worked example
A 51-year-old patient with hypertension and GERD presents a refill request for levothyroxine 75 mcg tablets, 1 tablet by mouth every morning, quantity 30. The system shows one fill remaining but the patient says the tablets look different from last month and asks if the new manufacturer will “work the same.” The label has been generated, and the product selected matches the NDC on file for the current stock. The question asks for the best next step for the technician.
Identify task: Determine whether the technician may explain therapeutic equivalence concerns. Extract key facts: Refill is authorized; product selection is routine; patient asks about whether the product will work the same, which is a clinical-use reassurance question. Apply rule: Technician may continue processing and route the equivalence/counseling question to the pharmacist. Eliminate distractors: Reject options stating that same active ingredient always means the technician should reassure the patient. Reject options to delay all processing without reason. Verify: Continue permitted steps and ensure pharmacist counseling handoff.
C Exam trap
D Checkpoint
Question: Which option best reflects the technician's role when a prescription question contains both routine processing and a clinical concern?
- Resolve the clinical concern if the medication is commonly dispensed in the pharmacy.
- Stop all workflow immediately even when routine data entry can still be completed safely.
- Complete permitted processing steps and refer the clinical concern to the pharmacist.
- Ask the patient to search online and return if still concerned.
Answer: C
- A: Tempting because familiarity may feel like competence; wrong because common use does not create authority.
- B: Tempting because escalation is safe; wrong because the best answer often allows routine processing to continue while the pharmacist addresses the issue.
- C: Tempting because it sounds balanced; right because it preserves workflow without crossing into clinical judgment.
- D: Tempting because it avoids giving advice directly; wrong because the pharmacy must route appropriate questions to the pharmacist, not dismiss them.
Exam Traps & Differentiators
| Looks acceptable | Why it tempts | Why it is wrong | Single clue that eliminates it |
|---|---|---|---|
| Answering a side-effect question for a common drug | Feels like basic customer service | It is counseling | Patient asks about expected effects or risks |
| Releasing a prepared prescription after matching NDC | Preparation feels complete | Final verification is pharmacist-only | No pharmacist check has occurred |
| Changing to an available strength because stock is low | Seems operational and efficient | It changes therapy details | Any substitution or strength change needs authorization |
| Giving a few tablets when no refills remain | Patient urgency creates pressure | Technician cannot authorize supply beyond authorization | No refill remains |
| Explaining inhaler or insulin administration steps | Device use seems mechanical | Medication-use instruction is counseling | Question asks how the patient should administer it |
| Deciding an allergy entry is not serious | Patient minimizes the reaction | Clinical interpretation is not technician work | Allergy-related concern is present |
1.1.1.9 Most common wrong answer and why
The most common wrong answer is the one where the technician gives a small amount of clinical help because it seems efficient, familiar, or compassionate. The exam rewards the technician who protects the boundary, documents appropriately, and routes the issue to the pharmacist instead of improvising.
1.1.1.10 Looks similar but isn't
| Situation | Technician may do | Technician must not do | Related future topic |
|---|---|---|---|
| Prescription entry | Type drug, strength, sig, quantity, refills as authorized | Rewrite unclear sig based on assumption | Prescription Data Entry |
| Patient question | Provide claim status and pickup timing | Advise on side effects or interactions | Patient Communication Boundaries |
| Product shortage | Notify pharmacist of stock issue | Choose an alternative strength or drug | Inventory Management Basics |
| Early refill request | Check profile and route request | Approve emergency quantity independently | Refill Processing Rules |
| Suspicious controlled prescription | Hold and escalate | Guess intended quantity or accept patient explanation alone | Controlled Substance Rules |
1.1.1.11 If the stem says ___, think ___
- If the stem says “patient asks whether it is safe”, think pharmacist counseling/interactions review.
- If the stem says “out of stock, can you switch?”, think no independent substitution.
- If the stem says “already counted and labeled”, think still needs pharmacist verification.
- If the stem says “no refills remaining”, think do not authorize supply independently.
- If the stem says “allergy,” “contraindication,” or “unusual dose”, think pause and route.
- If the stem says “busy shift” or “patient is in a hurry”, think pressure is a distractor, not permission.
Tables
| Key fact/value | High-yield takeaway |
|---|---|
| Routine processing | Usually technician-permitted under supervision |
| Final verification | Pharmacist-only |
| Patient counseling | Pharmacist-only |
| Therapy selection/substitution | Not a technician decision |
| Allergy/interaction assessment | Escalate to pharmacist |
| Unclear or conflicting directions | Hold and clarify through proper workflow |
| No refills remaining | Do not authorize additional supply independently |
| Suspicious prescription change | Do not guess; route immediately |
| Comparison point | Technician action | Pharmacist action |
|---|---|---|
| Enter routine order data | Allowed | Oversees and reviews as required |
| Select product matching order | Allowed for preparation | Verifies final match |
| Answer “How do I take this?” | Not allowed | Provides counseling |
| Decide whether dose is appropriate | Not allowed | Performs clinical assessment |
| Approve early refill without authorization | Not allowed | Handles according to law/policy and prescriber authorization |
| Perform final prescription verification | Not allowed | Required pharmacist duty |
| Differential cue in stem | Routine process issue | Boundary/escalation issue |
|---|---|---|
| “Insurance rejected claim” | Check demographics, BIN/PCN, coverage workflow | Only if patient asks clinical substitute choice |
| “Patient asks if medication is safe with another drug” | None | Interaction review and counseling |
| “Sig missing frequency” | Data entry cannot be completed as-is | Requires clarification pathway |
| “Medication out of stock” | Notify team, check inventory procedures | Cannot independently change therapy or strength |
| “Prescription already counted and labeled” | Preparation complete | Still not verified for dispensing |
| “Patient says allergy was probably nothing” | Document concern and route | Cannot reclassify or override allergy significance |
Algorithm / Approach
Rapid Review
- Routine data entry → allowed when entered exactly as authorized.
- Final verification → always pharmacist-only.
- Patient asks “is this safe with...” → think interaction/counseling referral.
- Product shortage → notify and escalate, not substitute independently.
- No refills remaining → do not authorize extra supply.
- Suspicious alteration → hold and route, never guess conservatively.
- Device-use explanation → counseling boundary, not just demonstration.
- Claim status question → technician can answer.
- Allergy note minimized by patient → still route to pharmacist.
- Common drug familiarity → does not expand scope.
- Urgent travel story → pressure distractor, not permission.
- NDC matched and counted → still not ready without pharmacist verification.
- Changing directions for convenience → unauthorized alteration.
- Safest next step → usually process routine parts, escalate judgment parts.
Self-check quiz
1. A technician is processing atorvastatin 20 mg tablets, take 1 tablet by mouth daily, quantity 30, for a 62-year-old patient with hypertension and type 2 diabetes. The patient asks whether the medication should be taken in the morning or at night and says he also takes aspirin daily. Which action is most appropriate?
- Advise the patient to take it at night because statins usually work best then.
- Refer the administration question to the pharmacist while continuing routine processing.
- Tell the patient to stop aspirin until speaking with the prescriber.
- Change the directions on the label to “take at bedtime.”
2. A technician has entered and labeled amlodipine 5 mg tablets, take 1 tablet by mouth daily, quantity 90, for a 54-year-old patient with hypertension and hyperlipidemia. The NDC matches the intended product, and the patient is waiting at pickup. Which step still requires pharmacist involvement?
- Final verification before dispensing
- Printing the receipt
- Placing the bottle in the pickup bag
- Confirming the patient’s address
3. A 38-year-old patient with asthma and seasonal allergies presents a new prescription for azithromycin 250 mg tablets: take 2 tablets by mouth on day 1, then 1 tablet daily on days 2-5, quantity 6. During intake, the patient asks whether it will interfere with her oral contraceptive and mentions mild nausea with antibiotics in the past. What is the most appropriate technician action?
- Explain that nausea is common and oral contraceptives should still work.
- Process the prescription and refer the medication-use question to the pharmacist.
- Tell the patient to use backup contraception for a month without involving the pharmacist.
- Refuse to enter the prescription until the prescriber confirms no interaction.
4. A 71-year-old patient with chronic pain and constipation brings in hydrocodone/acetaminophen 5 mg/325 mg tablets, 1 tablet by mouth every 6 hours as needed, quantity 12. The written date appears changed, and the patient says the prescriber “fixed it in the office.” Which action is most appropriate for the technician?
- Process it if the patient has filled the medication before.
- Ask the patient to initial the corrected date and continue processing.
- Pause and route the suspicious prescription detail to the pharmacist.
- Rewrite the date in the computer based on the patient’s explanation.
5. A technician is working on metoprolol tartrate 50 mg tablets, take 1 tablet by mouth twice daily, quantity 60, for a 66-year-old patient with coronary artery disease and GERD. The exact strength on the shelf is temporarily out of stock, but metoprolol tartrate 25 mg tablets are available. Which action is most appropriate?
- Dispense 25 mg tablets and instruct the patient to take 2 tablets twice daily.
- Change the order to metoprolol succinate 50 mg once daily because it is similar.
- Notify the pharmacist of the stock issue and do not substitute independently.
- Contact the patient and ask which alternative they prefer.
6. A 47-year-old patient with hypothyroidism and iron-deficiency anemia requests a refill of levothyroxine 100 mcg tablets, take 1 tablet by mouth every morning, quantity 30. The system shows 0 refills remaining. The patient says she missed a physician appointment, is leaving town tonight, and only needs “a few tablets.” She also asks whether taking iron with levothyroxine is a problem. Which action is most appropriate?
- Provide 3 tablets as a courtesy and tell her to separate iron from levothyroxine.
- Tell her to skip iron for now and come back after travel.
- Refer the refill and medication-use questions to the pharmacist; do not authorize supply independently.
- Transfer the prescription to another pharmacy without pharmacist involvement.
7. A 59-year-old patient with COPD and glaucoma is picking up tiotropium inhalation capsules, inhale contents of 1 capsule daily using the device, quantity 30. The technician has already entered the order, selected the correct product, and printed the label. The patient asks whether the capsule should be swallowed and whether blurry vision would be normal. Which is the best next step?
- Explain device use because the technician has seen this inhaler frequently.
- Hand out the product because preparation is complete, then ask the pharmacist if needed.
- Continue permitted workflow tasks and refer administration and adverse-effect questions to the pharmacist before completion.
- Tell the patient to search the package insert and call later with questions.
8. A 65-year-old patient with atrial fibrillation and osteoarthritis presents a new prescription for sulfamethoxazole/trimethoprim DS 800 mg/160 mg tablets, take 1 tablet by mouth twice daily for 7 days, quantity 14. The profile lists warfarin 5 mg daily and a sulfa allergy entered years ago, though the patient says it was “just an upset stomach.” The patient also wants to know whether ibuprofen is okay for pain during treatment. Which technician action is most appropriate?
- Tell the patient upset stomach is not a real allergy and that ibuprofen is fine short-term.
- Enter the prescription and route the allergy, interaction, and counseling concerns to the pharmacist.
- Delete the antibiotic from the queue and tell the patient to contact the prescriber directly.
- Advise the patient to hold warfarin until the antibiotic course is complete.
Answer key
1. Correct answer: B
- A: Tempting because some students remember timing differences among statins; incorrect for this scenario because the technician is being asked to counsel on administration. Single clue: “Should be taken in the morning or at night” is a medication-use question. Source: FDA labeling; AHFS Drug Information.
- B: Tempting because it preserves workflow instead of stopping everything; correct because routine processing may continue while the pharmacist addresses administration counseling. Single clue: The task asks for the most appropriate technician action, not the best clinical timing. Source: ASHP technician role standards; ExCPT-safe scope guidance.
- C: Tempting because aspirin often appears in interaction-style stems; incorrect because telling the patient to stop another medication is pharmacist/prescriber territory. Single clue: It gives independent therapeutic advice. Source: AHFS; ASHP scope principles.
- D: Tempting because bedtime dosing may sound helpful; incorrect because changing directions without authorization is not allowed. Single clue: It alters the prescription label. Source: FDA labeling; pharmacy operations standards.
2. Correct answer: A
- A: Tempting because all preparation work seems done; correct because pharmacist final verification is the required checkpoint before dispensing. Single clue: The stem says entry, labeling, and NDC match are already complete. Source: ASHP pharmacy workflow standards; technician scope guidance.
- B: Tempting because it occurs near the end of the process; incorrect because printing a receipt is clerical. Single clue: It does not involve clinical or legal approval. Source: Pharmacy operations workflow practice standards.
- C: Tempting because bagging happens near pickup; incorrect because bagging is still preparatory. Single clue: It is not an authorization step. Source: ASHP workflow guidance.
- D: Tempting because identity confirmation is important; incorrect because confirming address is a nonclinical administrative task. Single clue: Demographic verification is within technician workflow. Source: HIPAA/operations guidance; technician role resources.
3. Correct answer: B
- A: Tempting because nausea and contraceptive questions are common; incorrect because this option gives counseling and interaction advice. Single clue: The patient asks whether the medication will interfere with another therapy. Source: AHFS Drug Information; FDA labeling.
- B: Tempting because it allows the workflow to continue; correct because technicians can process authorized order details while routing medication-use concerns to the pharmacist. Single clue: The issue is a clinical-use question, not a data-entry defect. Source: ASHP technician role guidance.
- C: Tempting because backup contraception sounds cautious; incorrect because it is independent clinical advice. Single clue: The technician is making a risk-management recommendation. Source: FDA labeling; pharmacist counseling standards.
- D: Tempting because referral is needed; incorrect because the technician does not have to stop all entry when the pharmacist can review the concern within workflow. Single clue: The prescription itself is processable as written. Source: ASHP workflow guidance.
4. Correct answer: C
- A: Tempting because prior fills reduce suspicion in some learners’ minds; incorrect because a suspicious prescription detail still requires review. Single clue: The written date appears changed. Source: DEA/federal controlled substance handling principles; pharmacy compliance standards.
- B: Tempting because it attempts documentation; incorrect because the patient cannot legitimize a suspicious altered prescription through initials. Single clue: The legal concern is with the prescription itself. Source: Controlled substance compliance guidance.
- C: Tempting because it is the safest operational action; correct because suspicious altered information must be routed to the pharmacist. Single clue: Controlled medication plus altered date. Source: DEA compliance concepts; ASHP legal-safety workflow guidance.
- D: Tempting because entering data feels procedural; incorrect because guessing from the patient’s explanation is not authorized. Single clue: Technician cannot resolve suspicious legal ambiguity independently. Source: Compliance and audit-trail standards.
5. Correct answer: C
- A: Tempting because 25 mg times 2 equals 50 mg, making it a dose-adjustment trap; incorrect because the technician cannot independently change dosage instructions or quantity strategy. Single clue: The available strength differs from the authorized product. Source: FDA labeling; ASHP workflow/scope guidance.
- B: Tempting because succinate and tartrate are related products, making it a close-call formulation trap; incorrect because changing formulation and regimen is a therapeutic substitution decision. Single clue: Different dosage form/release pattern and schedule. Source: AHFS Drug Information; product labeling.
- C: Tempting because it feels slower; correct because the technician should notify the pharmacist and avoid independent substitution when stock is short. Single clue: Stock issue does not expand scope. Source: ASHP operations guidance.
- D: Tempting because it sounds patient-centered; incorrect because the patient cannot authorize an alternative product choice. Single clue: Product selection alternatives require authorized decision-making. Source: Pharmacy operations and legal scope standards.
6. Correct answer: C
- A: Tempting because it addresses both urgency and the iron interaction in one move; incorrect because it combines unauthorized refill approval with counseling. Single clue: “0 refills remaining” plus medication-use question. Source: ASHP technician role guidance; FDA labeling for levothyroxine administration interactions.
- B: Tempting because separating iron and levothyroxine is a known counseling pearl; incorrect because the technician still cannot provide independent administration advice or solve the refill issue. Single clue: It gives clinical instruction. Source: AHFS; FDA labeling.
- C: Tempting because it may feel less helpful than an immediate fix; correct because both the refill authorization problem and medication-use question require pharmacist handling. Single clue: No refills remain, and the patient asks about concomitant use. Source: ASHP workflow and scope standards; FDA labeling.
- D: Tempting because transfer workflows exist; incorrect because transfer handling depends on law/policy and pharmacist involvement, and it does not solve the counseling issue. Single clue: The option bypasses the central authorization problem. Source: Pharmacy law/operations standards.
7. Correct answer: C
- A: Tempting because tiotropium device questions are common and familiar; incorrect because instructing the patient how to administer it is counseling. Single clue: “Should the capsule be swallowed” asks for administration instruction. Source: FDA labeling; pharmacist counseling standards.
- B: Tempting because product preparation is complete; incorrect because neither final verification nor patient counseling handoff has been addressed. Single clue: The patient has unresolved clinical-use questions before completion. Source: ASHP workflow guidance.
- C: Tempting because it is a two-part action; correct because the technician can continue permitted workflow tasks while routing administration and adverse-effect questions to the pharmacist. Single clue: The stem mixes routine preparation with counseling issues. Source: ASHP scope guidance; FDA labeling.
- D: Tempting because it avoids giving advice; incorrect because it fails to provide the required pharmacist handoff. Single clue: The patient asked legitimate medication questions at pickup. Source: Pharmacy communication standards.
8. Correct answer: B
- A: Tempting because upset stomach may suggest intolerance and ibuprofen is common OTC therapy; incorrect because this option reclassifies the allergy concern and gives interaction advice. Single clue: Allergy history, warfarin, and pain-medication counseling are all clinical concerns. Source: AHFS Drug Information; FDA labeling.
- B: Tempting because it may feel incomplete to not resolve anything directly; correct because entry of the authorized prescription can occur while the allergy, warfarin interaction, and ibuprofen counseling questions are referred to the pharmacist. Single clue: Multiple clinical red flags are present, but the technician role is still process-and-route. Source: ASHP technician scope guidance; FDA labeling.
- C: Tempting because the situation is high risk; incorrect because the technician should not unilaterally delete the order and send the patient away without pharmacist review. Single clue: Proper escalation is internal to the pharmacist, not independent cancellation. Source: Workflow safety standards.
- D: Tempting because students may know the combination can be concerning, creating a drug-interaction trap; incorrect because instructing the patient to hold warfarin is a major clinical management decision. Single clue: It changes current therapy. Source: AHFS; anticoagulation medication labeling.