Why it matters
- Many EOR surgery questions are not asking for the operation; they are asking whether it is safe to get to the operation.
- The highest-yield discriminator is often not the diagnosis itself, but whether the patient has an active unstable condition that changes timing.
- Risk stratification prevents two common errors: overtesting low-risk patients and missing major red flags in high-risk patients.
- On exam stems, the safest next step is often optimize and escalate, not “clear for surgery.”
Key Terms & Must-Know Facts
1.1.1.1 Key terms
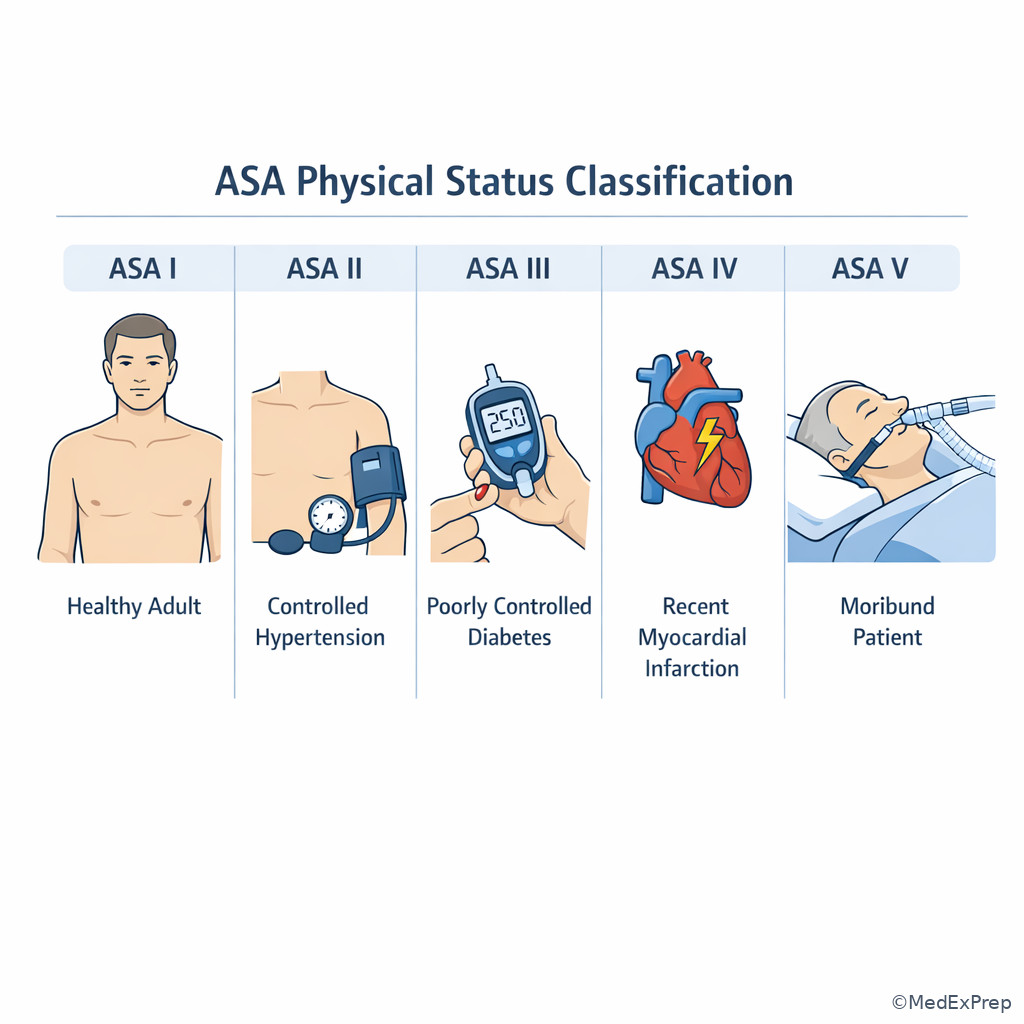
- ASA class: global preoperative physical-status grading system
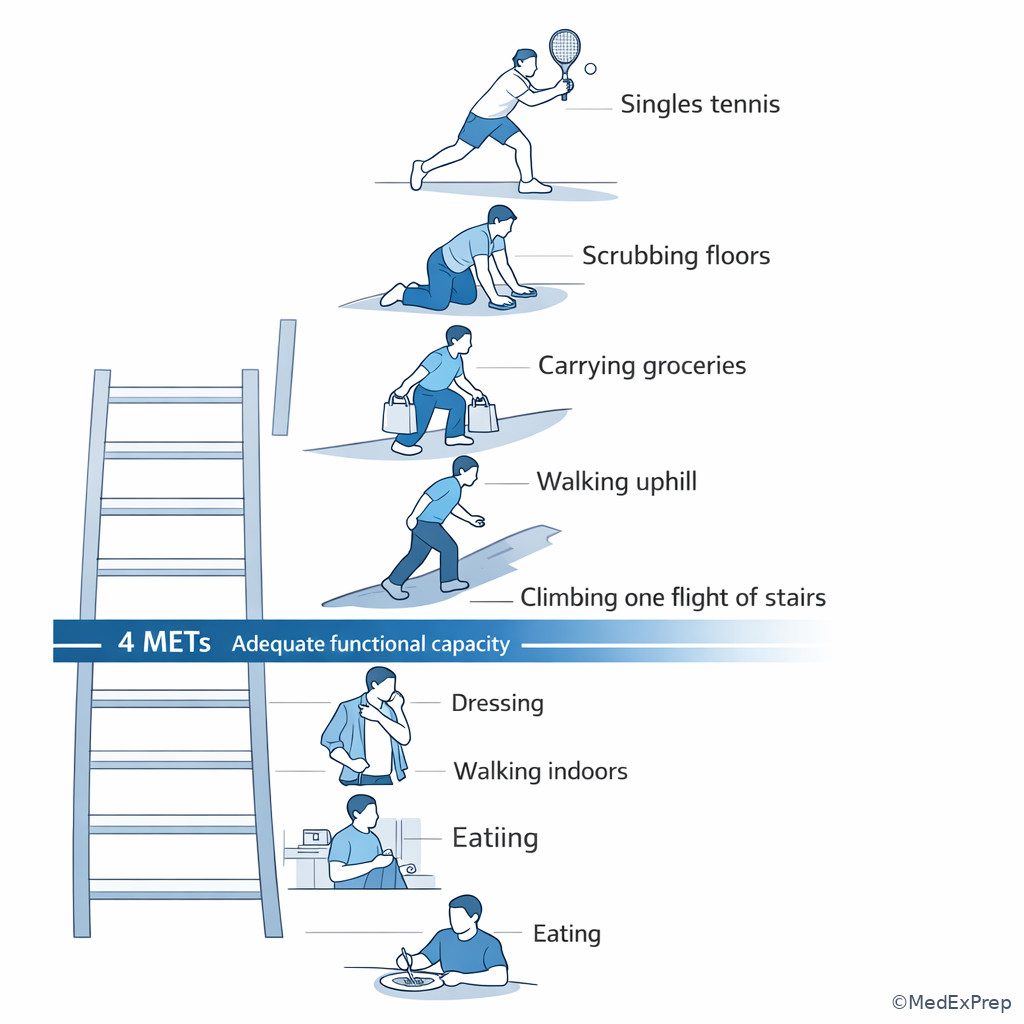
- Functional capacity: ability to perform exertion, often estimated in METs
- MET: metabolic equivalent; 4 METs is the common exam threshold for adequate capacity
- Active cardiac condition: unstable problem that can justify delaying elective surgery
- Major adverse cardiac event (MACE): perioperative cardiac complication outcome used in risk tools
- Low-risk surgery: procedure with low expected perioperative cardiac event rate
- Elevated-risk surgery: procedure with higher physiologic/cardiac stress
- Elective surgery: can be delayed for optimization
- Urgent/emergent surgery: limited ability to delay; stabilize and escalate
- Revised Cardiac Risk Index (RCRI): common perioperative cardiac risk tool
- Decompensated heart failure: symptomatic/unstable HF that raises perioperative risk sharply
- Unstable angina: active ischemic symptoms, not routine stable CAD
- Severe valvular disease: valve lesion with major hemodynamic consequence
- Optimization: correcting modifiable risks before elective surgery
1.1.1.2 Must-know facts
- A patient with an active cardiac condition is not a routine “proceed to OR” patient for elective surgery.
- Functional capacity ≥ 4 METs usually supports proceeding without further cardiac testing if no major red flags exist.
- Do not confuse procedure risk with patient risk; both matter, but unstable patient factors dominate.
- Routine preoperative testing is not indicated for every low-risk patient.
- Urgent or emergent surgery changes the frame: stabilize ABCs, communicate risk, and escalate rather than chase exhaustive testing.
- ASA class predicts overall perioperative risk but does not replace focused history and exam.
- Poorly controlled comorbidities matter more than merely having a diagnosis on the problem list.
- The exam often hides the key clue in exertional symptoms, recent cardiac events, or decompensated heart failure.
Exam takeaway: Use this sequence to decide whether to proceed, optimize, or delay for unstable conditions.
flowchart TD
A[Need for surgery] --> B{Urgent or emergent?}
B -->|Yes| C[Stabilize ABCs and notify supervising team]
C --> D[Proceed with focused risk mitigation]
B -->|No elective| E{Active cardiac condition?}
E -->|Yes| F[Delay elective surgery and evaluate]
E -->|No| G{Low-risk procedure or good functional capacity?}
G -->|Yes| H[Usually proceed without additional cardiac testing]
G -->|No| I[Consider targeted evaluation based on comorbidities] Exam takeaway: Estimate METs from real activities because 4 METs is the common threshold that changes next steps.
Exam takeaway: Separate mild stable disease from severe systemic disease because ASA class affects global perioperative risk framing.
Exam takeaway: Red-flag symptoms and unstable cardiac disease should trigger delay of elective cases and escalation.
flowchart LR A[Chest pain at rest] --> E[Active cardiac condition] B[Decompensated heart failure] --> E C[Significant arrhythmia with symptoms] --> E D[Severe symptomatic valve disease] --> E E --> F[Do not treat as routine clearance question]
Core content
1.1.1.3 Foundational framework: procedure risk versus patient risk
A Explanation
The first decision conflict in surgical risk stratification is simple but highly testable: Are you being asked about the operation’s baseline risk, the patient’s medical risk, or both? Many wrong answers come from focusing on only one side. A healthy patient having a high-stress vascular operation is not the same as a frail patient having cataract surgery. The rule that resolves this conflict is: start with timing and instability, then layer procedure risk, then patient-specific risk. If the surgery is emergent, you do not build an exhaustive elective workup; you stabilize and escalate. If the surgery is elective, then active unstable conditions dominate whether the case should proceed.
WHY THIS IS TESTED: exam stems force you to choose between “routine proceed,” “delay and optimize,” and “obtain targeted evaluation.” The testable pattern is that low-risk procedures rarely need extensive cardiac workup, while unstable patient findings can override even a minor procedure.
Think in three buckets: timing (emergent, urgent, elective), procedure stress (low-risk versus elevated-risk surgery), and patient reserve (cardiopulmonary disease, functional capacity, frailty, renal disease, diabetes, prior cardiac events). See Fig 1 for the decision sequence. When the stem includes words like “elective hernia repair,” “cataract surgery,” or “outpatient excision,” low procedural stress lowers the threshold to proceed. When it says “major intraperitoneal surgery,” “vascular surgery,” or “prolonged operation with fluid shifts,” procedure-related stress matters more.
B Worked example
A 63-year-old man is scheduled for elective inguinal hernia repair. He has hypertension, stage 3 CKD, and remote tobacco use. He says he gets “a little winded” when carrying groceries but can climb two flights of stairs without stopping. BP is 146/86 mm Hg. Creatinine is 1.5 mg/dL, unchanged from baseline. He mentions an episode of atypical chest discomfort six months ago after a large meal; prior ED evaluation was negative. The question asks for the most appropriate next step in perioperative assessment.
Reasoning chain: Identify the task: decide whether he needs more preop cardiac workup. Extract key facts: elective surgery, low-intermediate stress procedure, no active chest pain, no decompensated HF, functional capacity likely at least 4 METs because he climbs stairs. Apply rule: in the absence of active cardiac conditions, adequate functional capacity usually supports proceeding without additional cardiac stress testing. Eliminate distractors: the remote atypical chest discomfort is tempting noise but not active ischemia; stable CKD alone does not mandate cardiac testing. Verify: safest next step is to proceed with routine targeted preop evaluation rather than delay for stress testing.
C Exam trap
D Checkpoint
Question: A 58-year-old woman with controlled type 2 diabetes and well-controlled hypertension is preparing for elective carpal tunnel release. She walks 2 miles daily and denies chest pain, orthopnea, or syncope. Which is the most appropriate next step?
- Proceed without additional cardiac testing
- Order exercise stress testing before surgery
- Delay surgery for coronary angiography
- Obtain transthoracic echocardiography solely because of diabetes
- A. Tempting because the patient appears low risk; right because low-risk surgery plus good functional capacity and no active cardiac condition does not require further cardiac testing.
- B. Tempting because diabetes increases long-term cardiovascular risk; wrong because routine stress testing is not indicated when results are unlikely to change management.
- C. Tempting if you overreact to age and diabetes; wrong because there is no unstable ischemic syndrome or indication for invasive evaluation.
- D. Tempting because echocardiography feels “safe” and informative; wrong because diabetes alone is not an indication without symptoms or suspected structural disease.
1.1.1.4 Foundational framework: functional capacity, ASA class, and the 4-MET threshold
A Explanation
The next decision conflict is whether the stem is asking for a global risk label or a functional decision. ASA class gives a broad severity label, but functional capacity answers whether the patient can likely tolerate physiologic stress. The single rule that resolves many board items is: ≥ 4 METs with no active cardiac condition often supports proceeding. Examples around 4 METs include climbing a flight of stairs, walking uphill, or doing moderate housework. See Fig 2.
ASA class is still useful. An ASA II patient has mild systemic disease without major functional limitation. An ASA III patient has severe systemic disease with substantive functional impact. On test questions, a patient with controlled hypertension alone often sits lower risk than one with poorly controlled COPD on home oxygen or recurrent HF admissions. But ASA class by itself does not tell you what to order next. It is a framing tool, not a substitute for targeted preop reasoning.
Why do students miss this? Because they remember the names of ASA categories but not the practical question: Can this patient perform moderate activity without symptoms? Functional capacity matters most when the patient is undergoing elevated-risk surgery and you are deciding whether additional cardiac evaluation may help. Poor or unknown functional capacity does not automatically mean “stress test everyone”; it means the rest of the context becomes important.
B Worked example
A 72-year-old woman is scheduled for elective colectomy for colon cancer. She has COPD, CKD, and insulin-treated diabetes. She denies chest pain but says she must stop after walking one block because of dyspnea. She also reports chronic knee pain, making activity assessment less clear. Oxygen saturation is 95% on room air; lungs have mild wheezing. A tempting clue is that her ECG from last year was “normal.” The question asks for the best way to interpret her perioperative functional status.
Reasoning chain: Identify task: assess whether functional capacity reduces concern. Extract key facts: elevated-risk intra-abdominal surgery, poor or uncertain functional capacity, multiple comorbidities, no active ischemia but limited reserve. Apply rule: the normal old ECG does not answer current physiologic capacity. Eliminate distractors: “normal ECG means low cardiac risk” is false; “COPD explains everything” is too narrow because multimorbidity still matters. Verify: she has poor/uncertain functional capacity, so risk assessment cannot rely on the 4-MET reassurance shortcut.
C Exam trap
D Checkpoint
Question: Which patient most clearly demonstrates functional capacity of at least 4 METs for preoperative assessment?
- A 67-year-old man who can dress himself and walk inside his home only
- A 59-year-old woman who can climb one flight of stairs without symptoms
- A 74-year-old man who becomes dyspneic while bathing
- A 65-year-old woman who needs help carrying groceries across one room
- A. Tempting because independence sounds reassuring; wrong because basic self-care reflects much lower exertion.
- B. Tempting because stairs are a classic benchmark; right because stair climbing approximates the 4-MET threshold used in preop assessment.
- C. Tempting if you focus only on age; wrong because dyspnea with bathing indicates poor reserve.
- D. Tempting because grocery carrying sounds active; wrong because needing assistance suggests limited exertional capacity.
- The common functional-capacity threshold used in preop decision-making is ___ METs.
- True or False: ASA class alone determines whether cardiac testing is needed.
- Name one everyday activity that suggests adequate functional capacity.
| Activity clue | Approximate interpretation | Exam use |
|---|---|---|
| Eating, dressing, toileting | < 2 METs | Poor reserve; do not call this adequate capacity |
| Walking around house, light office work | About 2–3 METs | Still below common reassurance threshold |
| Climbing one flight of stairs | About 4 METs | Classic threshold supporting proceed-if-stable |
| Walking uphill, heavy housework | > 4 METs | Generally reassuring when no active cardiac condition |
| Strenuous sports | > 10 METs | Very good reserve; rarely the issue on EOR stems |
1.1.1.5 Application: recognize active cardiac conditions that delay elective surgery
A Explanation
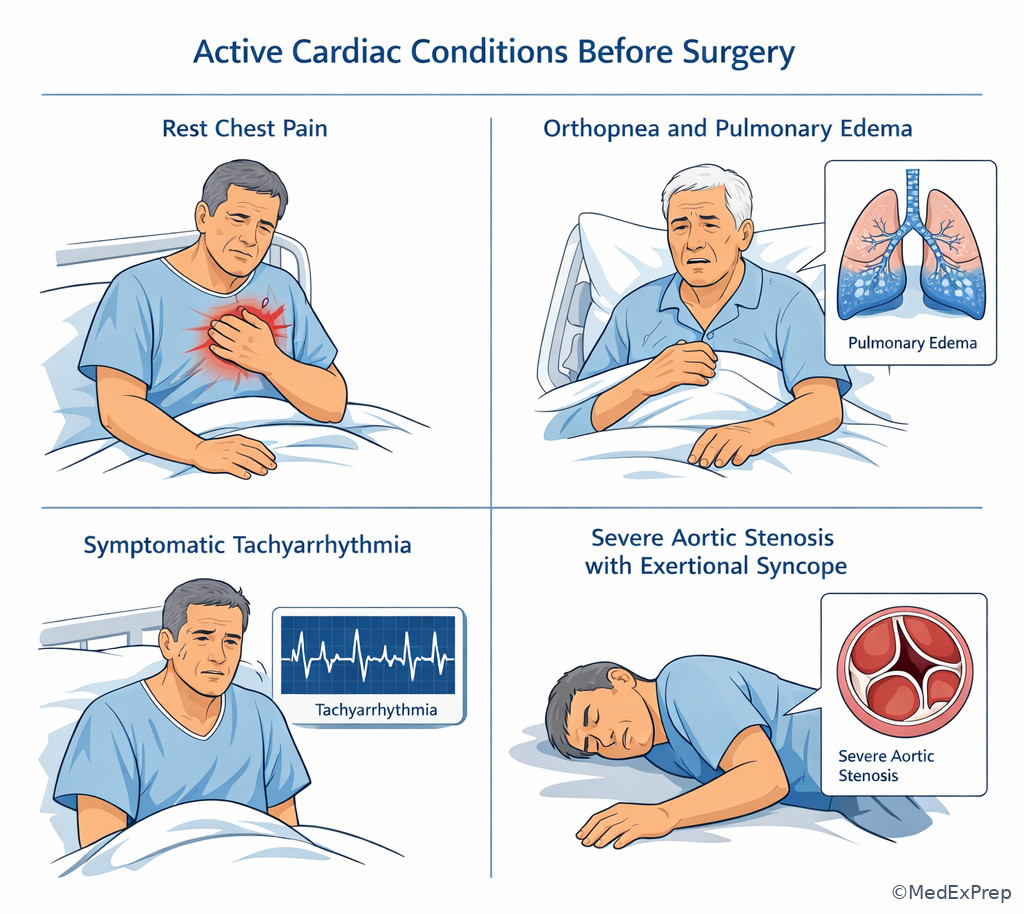
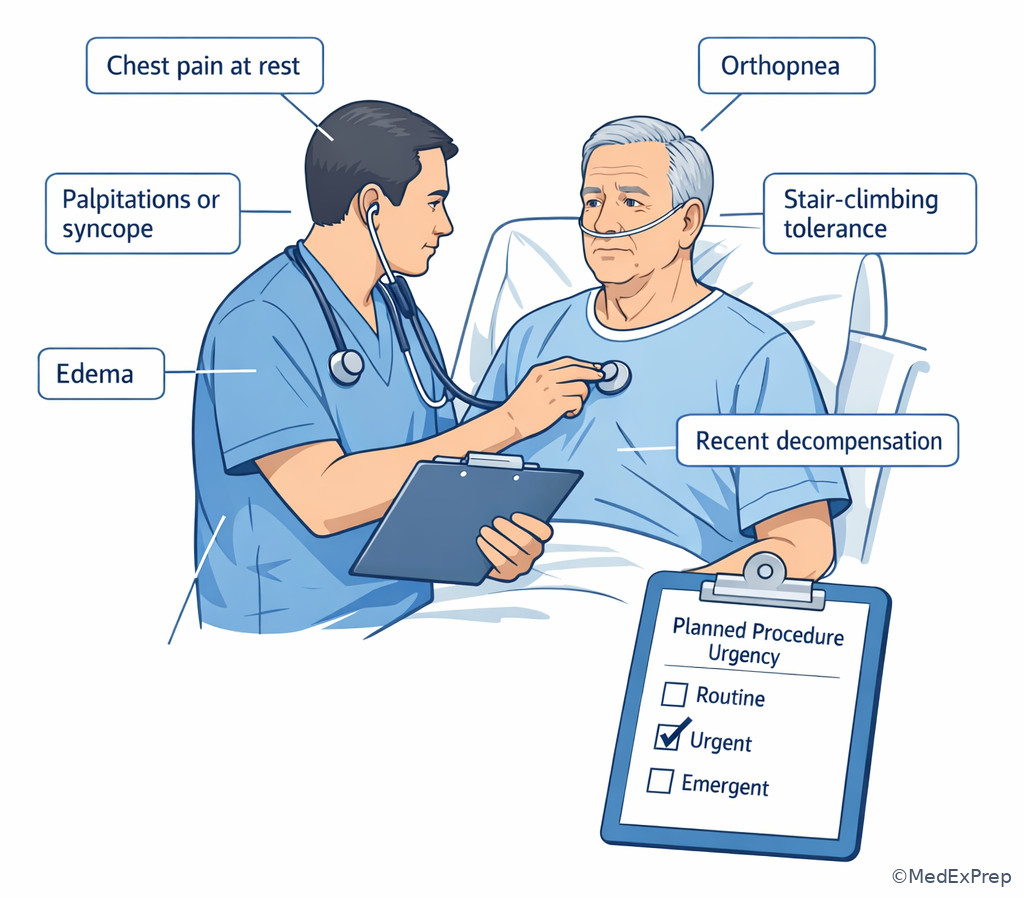
This is the most exam-relevant “do not miss” section. The decision conflict is whether the patient has stable chronic disease or an active cardiac condition that should delay elective surgery. The single finding/rule that resolves it is instability: new or worsening ischemia, decompensated heart failure, significant symptomatic arrhythmia, or severe symptomatic valvular disease means this is no longer a routine preop clearance question. See Fig 1 and the cardiac filter diagram above.
Classic clues include chest pain at rest, recent MI or unstable angina history, orthopnea/PND with volume overload, new edema with pulmonary congestion, syncope from severe aortic stenosis, rapid atrial arrhythmia causing symptoms, or high-grade conduction disease. The exam may disguise these with mild wording such as “increasing pillows at night,” “stopped halfway up stairs due to chest tightness,” or “lightheadedness with exertion.” Those details are the hinge. A patient with stable CAD who gardens daily is not the same as one with escalating angina last week.
For a PA student on a surgery service, the correct move is not to independently redesign the operation. It is to recognize the red flag, delay elective surgery if appropriate, stabilize what you can, and notify the supervising team for urgent evaluation. On emergent operations, you may not have the luxury of delay, but you still document and communicate the risk while helping optimize hemodynamics and monitoring.
Exam takeaway: Elective surgery should be delayed when instability signals an active cardiac condition.
flowchart TD
A[Elective surgery planned] --> B{Any active cardiac features?}
B -->|Rest chest pain or unstable angina| C[Delay and urgent evaluation]
B -->|Decompensated heart failure| C
B -->|Symptomatic significant arrhythmia| C
B -->|Severe symptomatic valve disease| C
B -->|None of these| D[Continue risk stratification pathway] Exam takeaway: Symptoms such as orthopnea, rest chest pain, syncope, or rapid symptomatic arrhythmia are more important than a long medication list.
B Worked example
A 69-year-old man is scheduled for elective ventral hernia repair. He has known coronary artery disease, HFrEF, and chronic kidney disease. He reports two weeks of worsening dyspnea, now needs three pillows to sleep, and gained 8 lb. He denies active fever. BNP is elevated; troponin is negative. A distractor is that his last stress test 10 months ago showed no inducible ischemia. The question asks for the most appropriate next step.
Reasoning chain: Identify task: proceed vs delay. Extract key facts: elective surgery, worsening HF symptoms, orthopnea, fluid retention. Apply rule: decompensated heart failure is an active cardiac condition requiring optimization and further evaluation before elective surgery. Eliminate distractors: negative troponin does not make him low risk; an old stress test does not erase new decompensation. Verify: delay elective surgery, notify the supervising team, and initiate evaluation/management for decompensated HF.
C Exam trap
D Checkpoint
Question: Which finding most strongly requires delaying an elective operation for further evaluation?
- Controlled hypertension with BP 148/88 mm Hg
- Ability to mow the lawn without symptoms
- Worsening orthopnea and new lower-extremity edema over 1 week
- Remote myocardial infarction 8 years ago without current symptoms
- A. Tempting because abnormal vitals attract attention; wrong because mild controlled hypertension alone is not the key delay trigger here.
- B. Tempting because exertion clues matter; wrong because this is actually reassuring functional capacity.
- C. Tempting because it sounds like fluid overload; right because worsening HF symptoms suggest decompensated heart failure, an active cardiac condition.
- D. Tempting because prior MI raises baseline risk; wrong because remote stable disease is not the same as current instability.
1.1.1.6 Application: use comorbidities and risk tools without overtesting
A Explanation
Once active red flags are excluded, the next conflict is whether chronic comorbidities justify targeted testing or whether the stem is baiting you into routine low-value testing. The single rule is: order tests when they are likely to change perioperative management. This is where comorbidities, procedure stress, and tools such as the RCRI help. RCRI elements classically include high-risk surgery, ischemic heart disease, heart failure, cerebrovascular disease, insulin-treated diabetes, and elevated creatinine. The test is not asking you to memorize a calculator output; it is asking whether the cluster of comorbidities meaningfully increases perioperative cardiac risk.
For foundational-level EOR prep, use risk tools as a supporting framework, not as a substitute for clinical judgment. Low-risk surgery in a stable patient with good functional capacity usually does not become a stress-test case just because one risk factor is present. On the other hand, elevated-risk surgery plus several risk markers and poor/unknown functional capacity may justify further evaluation if it would alter management.
The most common overtesting error is this sequence: older patient + diabetes + \(surgery = ECG\), echo, stress test, chest x-ray, coagulation panel “just because.” The exam expects more discipline. A stable patient with controlled comorbidities undergoing minor surgery does not need an indiscriminate battery. Forward-looking point: in the next lesson on Preoperative Testing Indications, you will decide exactly which tests are warranted and when.
B Worked example
A 66-year-old woman is preparing for elective laparoscopic cholecystectomy. She has prior stroke without residual deficit, insulin-treated diabetes, and CKD with creatinine 2.1 mg/dL. She can perform light housework but cannot reliably estimate stair tolerance due to severe hip osteoarthritis. She denies chest pain, orthopnea, or palpitations. A distracting note says her last chest x-ray “showed mild chronic hyperinflation.” The question asks whether her comorbidities should change risk estimation.
Reasoning chain: Identify task: integrate risk tools and capacity. Extract key facts: elevated comorbidity burden, poor/uncertain functional capacity, no active cardiac symptoms, nontrivial surgery. Apply rule: multiple RCRI-style risk factors increase perioperative cardiac risk and may justify more targeted assessment depending on whether results would change management. Eliminate distractors: chronic hyperinflation on old imaging is not the central issue; absence of chest pain does not erase all risk. Verify: her risk is meaningfully increased by cerebrovascular disease, insulin-treated diabetes, CKD, and uncertain capacity.
C Exam trap
D Checkpoint
Question: Which statement best matches perioperative use of chronic comorbidities in a stable elective patient?
- Any history of diabetes automatically requires preop stress testing
- Risk tools help estimate cardiac risk, but testing should be ordered only if it could change management
- A normal chest x-ray is sufficient to rule out perioperative cardiac complications
- Stable chronic kidney disease has no role in perioperative risk estimation
- A. Tempting because diabetes is high yield; wrong because not all diabetic patients need stress testing.
- B. Tempting because it sounds nuanced; right because risk tools support, rather than replace, case-specific decision-making.
- C. Tempting because normal imaging feels reassuring; wrong because chest x-ray does not rule out cardiac risk.
- D. Tempting if you narrow risk to the heart alone; wrong because CKD is a meaningful perioperative risk marker.
- True or False: A low-risk procedure plus good functional capacity usually requires routine cardiac stress testing.
- Name two chronic conditions commonly included in perioperative cardiac risk tools.
- The key question before ordering a preop test is whether the result will ___ management.
| Risk element | Why it matters | Common exam misuse |
|---|---|---|
| High-risk surgery | Greater hemodynamic stress and event rate | Treating minor ambulatory procedures as equivalent |
| Ischemic heart disease | Raises cardiac complication risk | Assuming all CAD is “active” even when stable |
| Heart failure | Especially important if decompensated | Ignoring worsening orthopnea or edema |
| Cerebrovascular disease | Marker of vascular burden | Overlooking it because current neuro exam is normal |
| Insulin-treated diabetes | Signals higher perioperative risk | Using diabetes alone to justify indiscriminate testing |
| Elevated creatinine/CKD | Associated with higher perioperative complications | Ignoring renal disease if cardiac symptoms are absent |
1.1.1.7 Integration: proceed, optimize, or delay in board-style scenarios
A Explanation
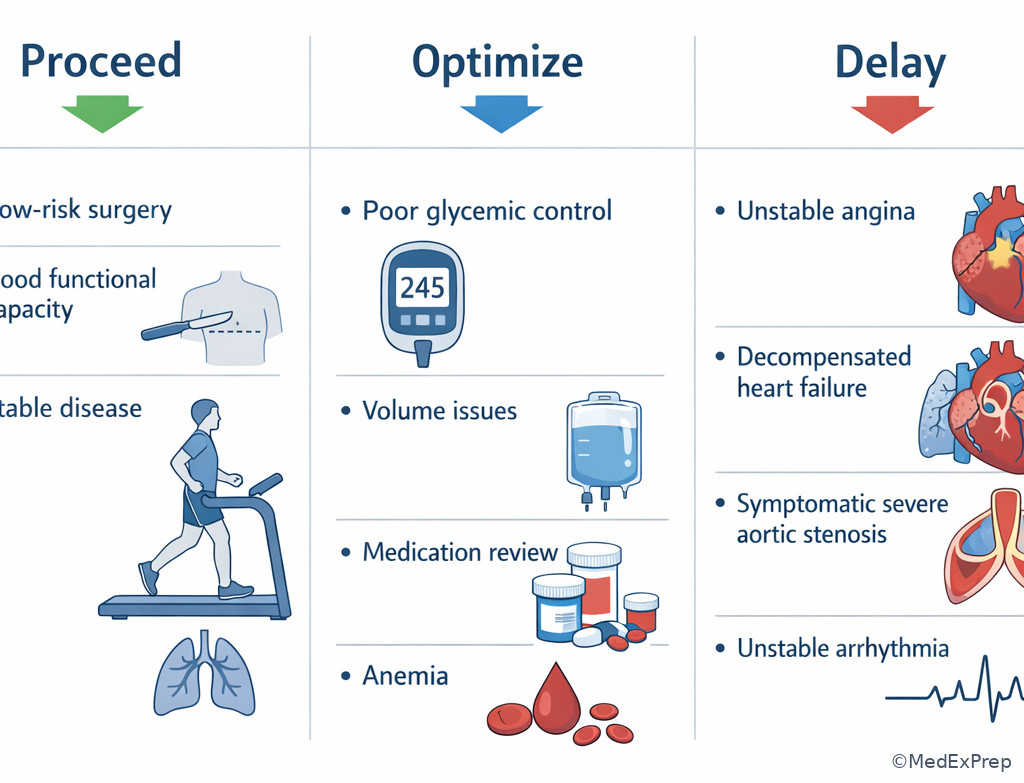
The final integration task is choosing among three actions: proceed, optimize, or delay. The decision conflict is not “what is the sickest diagnosis?” but “what is the safest next step within a supervised PA student role?” The resolving rule is hierarchical: emergency surgery proceeds with rapid stabilization; elective surgery with active unstable disease is delayed; elective surgery without active instability proceeds or receives selective optimization depending on risk and modifiable factors.
Optimization includes improving volume status, addressing infection, controlling severe hyperglycemia, evaluating recent cardiopulmonary change, clarifying anticoagulant management, and coordinating needed specialty input. Delay is appropriate when proceeding would expose the patient to avoidable harm and the surgery is not time-critical. Proceed means no unstable condition is present and additional testing is unlikely to change management. See Fig 3 for the unstable-cardiac branch and see Fig 4 below for a compare-and-choose image summary.
For the EOR exam, language matters. If a question says “elective” and gives worsening chest pain, syncope, or heart failure symptoms, the answer is usually not “obtain routine clearance paperwork.” If it says “urgent bowel obstruction” with significant comorbidity, the answer is not “delay until full outpatient cardiac workup”; instead, stabilize, communicate risk, and move within the urgency of the problem.
Exam takeaway: Match timing and instability to the action choice rather than reflexively ordering more tests.
Exam takeaway: The safest answer usually comes from identifying whether the patient needs proceed, optimization, or delay.
flowchart TD
A[Elective surgery patient] --> B{Active unstable condition?}
B -->|Yes| C[Delay and urgent evaluation]
B -->|No| D{Procedure low risk or functional capacity adequate?}
D -->|Yes| E[Proceed with routine targeted preparation]
D -->|No| F{Would further testing change management?}
F -->|Yes| G[Targeted optimization and evaluation]
F -->|No| E B Worked example
A 76-year-old woman presents with incarcerated femoral hernia and vomiting. She has a history of severe aortic stenosis, CKD, and coronary artery disease. She reports months of exertional presyncope but no current chest pain. Lactate is mildly elevated, and the surgical team is concerned for evolving bowel compromise. A tempting but wrong clue is that her outpatient valve evaluation is “not yet complete.” The question asks for the most appropriate next step.
Reasoning chain: Identify task: urgent surgical timing versus delay for cardiac workup. Determine stability and acuity: this is not elective; possible bowel compromise makes prolonged delay unsafe. Extract key facts: symptomatic severe valvular disease raises perioperative risk, but urgency limits the value of postponement for a full elective evaluation. Apply rule: urgent surgery proceeds with focused stabilization, explicit risk recognition, and immediate escalation to supervising surgery/anesthesia/cardiology as appropriate. Eliminate distractors: completing outpatient valve workup first is appealing because the valve disease is real, but the hernia complication is time-sensitive. Verify: stabilize, communicate risk, and expedite definitive surgical care rather than converting an urgent abdomen into an elective cardiology project.
C Exam trap
D Checkpoint
Question: A 70-year-old man needs elective total hip arthroplasty. He has stable CAD, no chest pain, no orthopnea, and can climb stairs carrying laundry. Which is the most appropriate overall disposition?
- Proceed with planned surgery without additional cardiac testing
- Delay surgery for coronary angiography because of known CAD
- Cancel surgery because age over 70 alone predicts prohibitive risk
- Obtain stress testing routinely because orthopedic surgery is always high risk
- A. Tempting because the patient sounds stable; right because stable CAD plus adequate functional capacity and no active cardiac condition usually supports proceeding.
- B. Tempting because CAD can worsen perioperative outcomes; wrong because stable disease alone does not mandate invasive evaluation.
- C. Tempting if you overvalue age; wrong because age alone does not prohibit surgery.
- D. Tempting because orthopedic surgery can involve significant stress; wrong because routine testing is not automatic when the patient is stable and functional.
| Scenario | Best frame | Best next step |
|---|---|---|
| Low-risk elective procedure, good functional capacity, stable disease | Low-value additional testing | Proceed with routine targeted preparation |
| Elective surgery, worsening orthopnea and edema | Active cardiac condition | Delay and evaluate/optimize |
| Urgent abdominal pathology, severe chronic comorbidity | No time for full elective workup | Stabilize, escalate, and proceed as urgency dictates |
| Poor/unknown functional capacity and multiple risk markers | Further assessment may matter | Consider targeted evaluation if results would change care |
| Stable remote MI with no current symptoms | Chronic risk, not active instability | Integrate with surgery type and capacity; do not reflexively delay |
Exam takeaway: Bedside questions about symptoms, exercise tolerance, and recent change often outperform indiscriminate testing.
Exam Traps & Differentiators
Most common wrong answer and why: ordering a stress test or broad “clearance workup” for any older patient with comorbidities. This is tempting because age, diabetes, and hypertension are familiar risk factors. It is wrong when the patient has low-risk surgery, adequate functional capacity, and no active unstable symptoms.
- Looks similar but isn’t: stable chronic CAD versus unstable angina. Both may mention prior heart disease; the discriminator is current symptoms or recent worsening.
- Looks similar but isn’t: dyspnea from deconditioning/COPD versus decompensated HF. The discriminator is orthopnea, PND, edema, weight gain, or pulmonary congestion.
- Looks similar but isn’t: poor mobility from arthritis versus poor cardiopulmonary reserve. The discriminator is whether limitation reflects joint pain or exertional cardiopulmonary symptoms.
- Related future trap: in Preoperative Testing Indications, the wrong answer will often be “order everything.” Risk stratification comes first so testing stays targeted.
- Related future trap: in Medication Management Preop, the wrong answer will be to hold or continue medications without balancing bleeding and thrombotic risk. Risk level sets that conversation.
| Confusable pair | Why they seem similar | Single discriminator |
|---|---|---|
| Stable angina vs unstable angina | Both involve coronary disease and chest discomfort history | Rest pain or increasing frequency/severity suggests unstable disease |
| Compensated HF vs decompensated HF | Both may have reduced EF history | New orthopnea, edema, weight gain, or pulmonary edema indicates decompensation |
| Low exercise due to arthritis vs poor METs from cardiac limitation | Both reduce measured activity | Symptom-limited exertion indicates physiologic reserve issue |
| Remote MI vs recent unstable ischemia | Both raise concern for perioperative events | Recent symptoms/change from baseline determine urgency |
| Risk factor burden vs active contraindication to elective surgery | Both increase concern | Active unstable condition changes timing; risk factors alone often do not |
If the stem says...
- “Can climb 2 flights of stairs” → think adequate functional capacity
- “Needs 3 pillows now; gained 6 lb this week” → think decompensated heart failure
- “Elective outpatient procedure” → think avoid reflex overtesting
- “Urgent abdominal pathology” → think stabilize and escalate, not exhaustive elective workup
- “Prior CAD but asymptomatic and active” → think stable disease does not equal automatic stress test
- “Unknown exercise tolerance because of arthritis” → think capacity is uncertain; context matters
Algorithm / Approach
Use this exact mental script on exam day: identify task → determine timing/stability → extract hinge clue → apply threshold/rule → reject reflex testing → choose safest next step. See Fig 5 for the elective pathway and Fig 6 for the bedside questions that often reveal the correct answer faster than labs.
Rapid Review
- Elective surgery + active cardiac condition → delay and evaluate
- Urgent surgery + major comorbidity → stabilize and escalate, not exhaustive elective workup
- Functional capacity ≥ 4 METs → usually reassuring if no active symptoms
- ASA class → global severity label, not a stand-alone next-step rule
- Stable CAD → not the same as unstable angina
- Orthopnea + weight gain → think decompensated HF, not simple deconditioning
- Low-risk procedure → usually low yield for routine cardiac testing
- Poor/unknown METs + multiple risk factors → consider whether targeted testing would change care
- Remote normal stress test → does not overrule new symptoms
- Arthritis-limited mobility → does not automatically equal poor cardiopulmonary reserve
- CKD and insulin-treated diabetes → meaningful perioperative risk markers
- “Clearance” wording in stem → still answer with risk reasoning, not paperwork
Self-check quiz
1. A 61-year-old man is being evaluated before elective knee arthroscopy. He has controlled hypertension and hyperlipidemia. He reports no chest pain, can climb one flight of stairs without symptoms, and has no edema or orthopnea. Which finding most supports proceeding without additional cardiac testing?
- Ability to climb one flight of stairs without symptoms
- History of hyperlipidemia
- Age older than 60 years
- Controlled hypertension on one medication
2. A 55-year-old woman with obesity and well-controlled diabetes is scheduled for elective trigger finger release. Which perioperative concept most directly describes a patient’s ability to tolerate exertion-based physiologic stress?
- ASA class
- Functional capacity
- Surgical wound class
- Pain score
3. A 73-year-old woman is preparing for elective ventral hernia repair. She has HFrEF, CKD, and hypertension. Over the last week she has developed worsening orthopnea and new bilateral leg edema. Troponin is negative, and she denies fever. What is the most appropriate next step?
- Proceed because the surgery is abdominal rather than cardiac
- Delay elective surgery and evaluate decompensated heart failure
- Proceed after obtaining a routine chest x-ray only
- Proceed because a negative troponin excludes major perioperative risk
4. A 68-year-old man with prior stroke, insulin-treated diabetes, and CKD is scheduled for elective colectomy. He denies chest pain, but severe hip arthritis makes his exercise tolerance difficult to assess. Which is the most appropriate principle to guide additional testing?
- Order broad routine testing because any colectomy requires full cardiac workup
- Use targeted evaluation only if the result would change perioperative management
- Avoid all further assessment because he has no chest pain
- Use age alone to determine whether the operation should be canceled
5. A 64-year-old woman with stable coronary artery disease, COPD, and osteoarthritis is scheduled for elective laparoscopic cholecystectomy. She denies chest pain and says she can walk uphill to her mailbox and carry groceries into the house. Which is the most appropriate interpretation?
- She has poor functional capacity and needs mandatory stress testing
- She likely has adequate functional capacity of at least 4 METs
- Her COPD automatically outweighs the activity history
- Her CAD history alone indicates an active cardiac condition
6. A 77-year-old man presents with an incarcerated groin hernia, vomiting, and increasing abdominal pain. He has symptomatic severe aortic stenosis, CKD, and coronary artery disease. He reports exertional presyncope for months but now has concern for bowel compromise on exam. Which is the most appropriate next step?
- Delay surgery until full outpatient valve evaluation is completed
- Proceed with urgent stabilization and immediate escalation because the surgical problem is time-sensitive
- Cancel operative planning because symptomatic aortic stenosis makes surgery absolutely contraindicated
- Discharge for elective follow-up after cardiology review
7. A 70-year-old woman is scheduled for elective colon resection. She has CAD, CKD, and diabetes. She denies chest pain. She says she cannot walk far because of knee pain, but she also becomes short of breath when hurrying across a parking lot. Which single detail most prevents you from treating her limited activity as purely orthopedic?
- Her age
- Her diabetes history
- Dyspnea with exertion
- The planned abdominal operation
8. A 66-year-old man is scheduled for elective hip replacement. He has remote MI, well-controlled hypertension, and CKD stage 3. He gardens daily, climbs stairs carrying tools, and denies orthopnea, palpitations, or chest pain. Which is the most appropriate management strategy?
- Delay for coronary angiography because of prior MI and CKD
- Proceed without additional cardiac testing because disease appears stable and functional capacity is adequate
- Cancel surgery because CKD stage 3 creates prohibitive operative risk
- Obtain stress testing routinely because orthopedic surgery always requires it
Answer key
1.1.1.8 Question 1: A
Correct answer mechanism-to-treatment logic: Climbing one flight of stairs without symptoms suggests functional capacity of about 4 METs, which is commonly used as a reassuring threshold in perioperative assessment when there is no active cardiac condition. For a low-stress elective procedure, this supports proceeding without additional cardiac testing. Sources: 2024 ACC/AHA perioperative cardiovascular management guideline; Goldman-Cecil Medicine.
- A. Ability to climb one flight of stairs without symptoms — Tempting because it is a classic exam clue; correct because it directly estimates adequate functional capacity. Single stem clue: stair climbing without symptoms.
- B. History of hyperlipidemia — Tempting because it is a cardiovascular risk factor; incorrect because it does not by itself determine perioperative testing needs. Single stem clue: no active symptoms and good activity tolerance matter more.
- C. Age older than 60 years — Tempting because age raises baseline risk; incorrect because age alone is not the operational decision point. Single stem clue: preserved exertional tolerance.
- D. Controlled hypertension on one medication — Tempting because blood pressure is always reviewed preop; incorrect because controlled hypertension alone does not drive cardiac testing. Single stem clue: no instability or poor capacity.
1.1.1.9 Question 2: B
Correct answer mechanism-to-treatment logic: Functional capacity reflects the patient’s ability to tolerate exertional physiologic stress and is commonly estimated in METs during preoperative assessment. It helps determine whether additional cardiac testing is likely to be useful. Sources: 2024 ACC/AHA guideline; Sabiston Textbook of Surgery.
- A. ASA class — Tempting because it is a preop label; incorrect because ASA class describes global illness severity rather than exertional reserve. Single stem clue: “ability to tolerate exertion-based physiologic stress.”
- B. Functional capacity — Tempting and correct because it directly matches the construct being asked. Single stem clue: exertion tolerance.
- C. Surgical wound class — Tempting because it is another perioperative term; incorrect because it relates to contamination/infection risk, not cardiopulmonary reserve. Single stem clue: not about wound contamination.
- D. Pain score — Tempting because symptoms can limit activity; incorrect because pain score is not the formal perioperative risk concept for physiologic reserve. Single stem clue: board-style preop framework language.
1.1.1.10 Question 3: B
Correct answer mechanism-to-treatment logic: Worsening orthopnea and new edema in a patient with HFrEF indicate decompensated heart failure, an active cardiac condition that should delay elective surgery pending evaluation and optimization. Negative troponin does not exclude clinically significant perioperative HF risk. Sources: 2024 ACC/AHA guideline; Harrison’s Principles of Internal Medicine.
- A. Proceed because the surgery is abdominal rather than cardiac — Tempting because the operation does not involve the heart; incorrect because perioperative risk depends on patient instability, not operative specialty. Single stem clue: worsening orthopnea and edema.
- B. Delay elective surgery and evaluate decompensated heart failure — Tempting and correct because the symptoms signal an active unstable condition. Single stem clue: new HF symptoms over one week.
- C. Proceed after obtaining a routine chest x-ray only — Tempting because chest x-ray may show congestion; incorrect because imaging alone does not address the need to delay and optimize. Single stem clue: this is not a routine screening problem.
- D. Proceed because a negative troponin excludes major perioperative risk — Tempting because troponin is associated with acute coronary syndromes; incorrect because heart failure decompensation can be high risk without troponin elevation. Single stem clue: HF symptoms, not ACS biomarkers, drive the decision here.
1.1.1.11 Question 4: B
Correct answer mechanism-to-treatment logic: In a stable elective patient with multiple risk markers and uncertain functional capacity, additional testing should be considered only if the result would change perioperative management. This prevents low-value indiscriminate testing. Sources: 2024 ACC/AHA guideline; Goldman-Cecil Medicine.
- A. Order broad routine testing because any colectomy requires full cardiac workup — Tempting because colectomy is a substantial operation; incorrect because testing is not automatic and must be purposeful. Single stem clue: the question asks for the governing principle.
- B. Use targeted evaluation only if the result would change perioperative management — Tempting and correct because this is the core preop testing rule. Single stem clue: uncertain capacity plus comorbidities, not overt instability.
- C. Avoid all further assessment because he has no chest pain — Tempting because chest pain is a major red flag; incorrect because absence of chest pain does not erase all risk. Single stem clue: CKD, prior stroke, and insulin-treated diabetes still matter.
- D. Use age alone to determine whether the operation should be canceled — Tempting because age correlates with complications; incorrect because age alone is not a cancellation rule. Single stem clue: the stem emphasizes comorbidity integration, not age cutoff.
1.1.1.12 Question 5: B
Correct answer mechanism-to-treatment logic: Walking uphill and carrying groceries are practical activity clues consistent with at least moderate exertional capacity, roughly the 4-MET range or higher. In the absence of active symptoms, this is generally reassuring. Sources: 2024 ACC/AHA guideline; Sabiston Textbook of Surgery.
- A. She has poor functional capacity and needs mandatory stress testing — Tempting because CAD and COPD can increase risk; incorrect because the activity history suggests adequate capacity. Single stem clue: walking uphill and carrying groceries.
- B. She likely has adequate functional capacity of at least 4 METs — Tempting and correct because the described activities cross the practical threshold. Single stem clue: exertional activities without symptoms.
- C. Her COPD automatically outweighs the activity history — Tempting because pulmonary disease affects reserve; incorrect because stable COPD does not nullify demonstrated functional capacity. Single stem clue: no limiting respiratory symptoms during moderate activity.
- D. Her CAD history alone indicates an active cardiac condition — Tempting because CAD is high yield; incorrect because stable history without current symptoms is not an active condition. Single stem clue: denies chest pain and remains active.
1.1.1.13 Question 6: B
Correct answer mechanism-to-treatment logic: The patient has a time-sensitive surgical emergency concern—possible bowel compromise from an incarcerated hernia. Symptomatic severe aortic stenosis increases perioperative risk substantially, but urgent pathology limits the ability to defer for a complete elective workup. The correct approach is focused stabilization, urgent escalation, and expedited definitive care. Sources: 2024 ACC/AHA guideline; Sabiston Textbook of Surgery.
- A. Delay surgery until full outpatient valve evaluation is completed — Tempting because symptomatic severe aortic stenosis is genuinely dangerous; incorrect because outpatient delay risks bowel ischemia or perforation. Single stem clue: concern for bowel compromise.
- B. Proceed with urgent stabilization and immediate escalation because the surgical problem is time-sensitive — Tempting and correct because urgency changes the risk calculus. Single stem clue: incarcerated hernia with increasing pain and vomiting.
- C. Cancel operative planning because symptomatic aortic stenosis makes surgery absolutely contraindicated — Tempting because the valve lesion is high risk; incorrect because urgent surgery may still be necessary. Single stem clue: not an elective case.
- D. Discharge for elective follow-up after cardiology review — Tempting if you anchor solely on chronic symptoms; incorrect because the acute surgical abdomen concern makes discharge unsafe. Single stem clue: vomiting plus increasing abdominal pain with incarceration.
1.1.1.14 Question 7: C
Correct answer mechanism-to-treatment logic: In preoperative evaluation, limited activity from musculoskeletal pain can obscure functional assessment. However, exertional dyspnea suggests true cardiopulmonary limitation rather than a purely orthopedic barrier, making capacity less reassuring. Sources: 2024 ACC/AHA guideline; Harrison’s Principles of Internal Medicine.
- A. Her age — Tempting because older age correlates with lower reserve; incorrect because age alone does not distinguish orthopedic limitation from cardiopulmonary limitation. Single stem clue: symptom quality matters more than age.
- B. Her diabetes history — Tempting because diabetes raises cardiovascular risk; incorrect because it does not specifically explain the activity limitation. Single stem clue: the question asks what prevents a purely orthopedic interpretation.
- C. Dyspnea with exertion — Tempting and correct because it points to physiologic limitation beyond knee pain. Single stem clue: shortness of breath when hurrying across a parking lot.
- D. The planned abdominal operation — Tempting because higher-stress surgery increases concern; incorrect because it does not explain the nature of her limited activity. Single stem clue: symptom-based functional assessment is the discriminating issue.
1.1.1.15 Question 8: B
Correct answer mechanism-to-treatment logic: Remote MI and CKD increase baseline perioperative risk, but this patient is stable, asymptomatic, and functionally active above the 4-MET threshold. In elective surgery, additional cardiac testing is not routinely indicated when it is unlikely to change management. Sources: 2024 ACC/AHA guideline; Goldman-Cecil Medicine.
- A. Delay for coronary angiography because of prior MI and CKD — Tempting because both conditions raise cardiac concern; incorrect because stable, asymptomatic patients with adequate function do not need invasive routine evaluation. Single stem clue: gardens daily and climbs stairs carrying tools.
- B. Proceed without additional cardiac testing because disease appears stable and functional capacity is adequate — Tempting and correct because the stem provides the exact reassurance cues. Single stem clue: high activity tolerance with no active symptoms.
- C. Cancel surgery because CKD stage 3 creates prohibitive operative risk — Tempting because CKD increases complications; incorrect because stage 3 CKD alone is not a categorical contraindication. Single stem clue: stable disease and preserved function.
- D. Obtain stress testing routinely because orthopedic surgery always requires it — Tempting because orthopedic procedures can be substantial; incorrect because testing is not automatic and must be management-changing. Single stem clue: adequate functional capacity makes routine testing low yield.