Why it matters
- Triage errors are tested as missed emergencies: the exam often hides a dangerous diagnosis behind a common complaint such as weakness, dizziness, abdominal pain, or anxiety.
- The first correct move in emergency medicine is often not the diagnosis but recognizing that the patient is too unstable to wait.
- PAEA-style questions reward the learner who prioritizes airway, perfusion, mental status, and time-sensitive red flags before ordering expansive workups.
- Disposition depends on acuity: the same symptom can be dischargeable in one patient and resuscitation-level in another based on one discriminating clue.
Key Terms & Must-Know Facts
1.1.1.1 Key terms
- Triage acuity: initial urgency assignment based on instability and risk.
- Red flag: a finding that raises concern for immediate threat to life, limb, or organ function.
- Unstable patient: patient with threatened airway, breathing, circulation, or severe neurologic compromise.
- Compensated shock: early shock with preserved blood pressure but abnormal heart rate, skin signs, mentation, or perfusion.
- Occult hypoperfusion: inadequate perfusion not obvious from a single normal blood pressure reading.
- Toxic appearance: ill-looking patient with poor tone, lethargy, pallor, cyanosis, or significant distress.
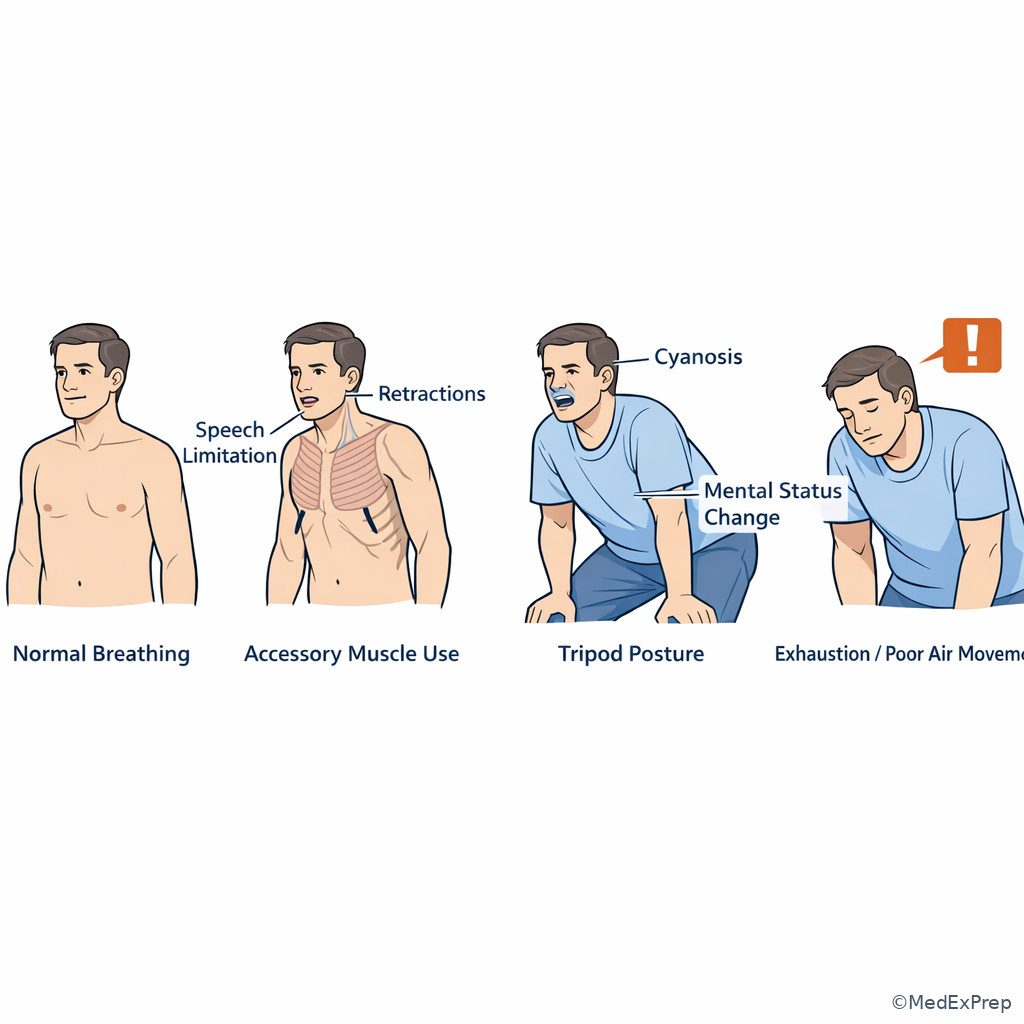
- Work of breathing: visible respiratory effort such as retractions, accessory muscle use, or inability to speak full sentences.
- Altered mental status: any acute change in alertness, orientation, attention, or behavior.
- Time-sensitive diagnosis: condition where delay worsens outcome, such as stroke, ACS, sepsis, ectopic pregnancy, or aortic catastrophe.
- ESI-style logic: concept that triage reflects expected resources and immediate danger, though exact institutional scales vary.
- Reassessment: repeat vital signs and clinical check after initial triage or intervention.
- High-risk complaint: symptom with dangerous causes disproportionate to its apparent severity.
1.1.1.2 Must-know facts
- A single normal blood pressure does not rule out shock.
- Altered mental status is a vital sign equivalent in emergency medicine.
- Abnormal appearance can outrank a modestly reassuring number.
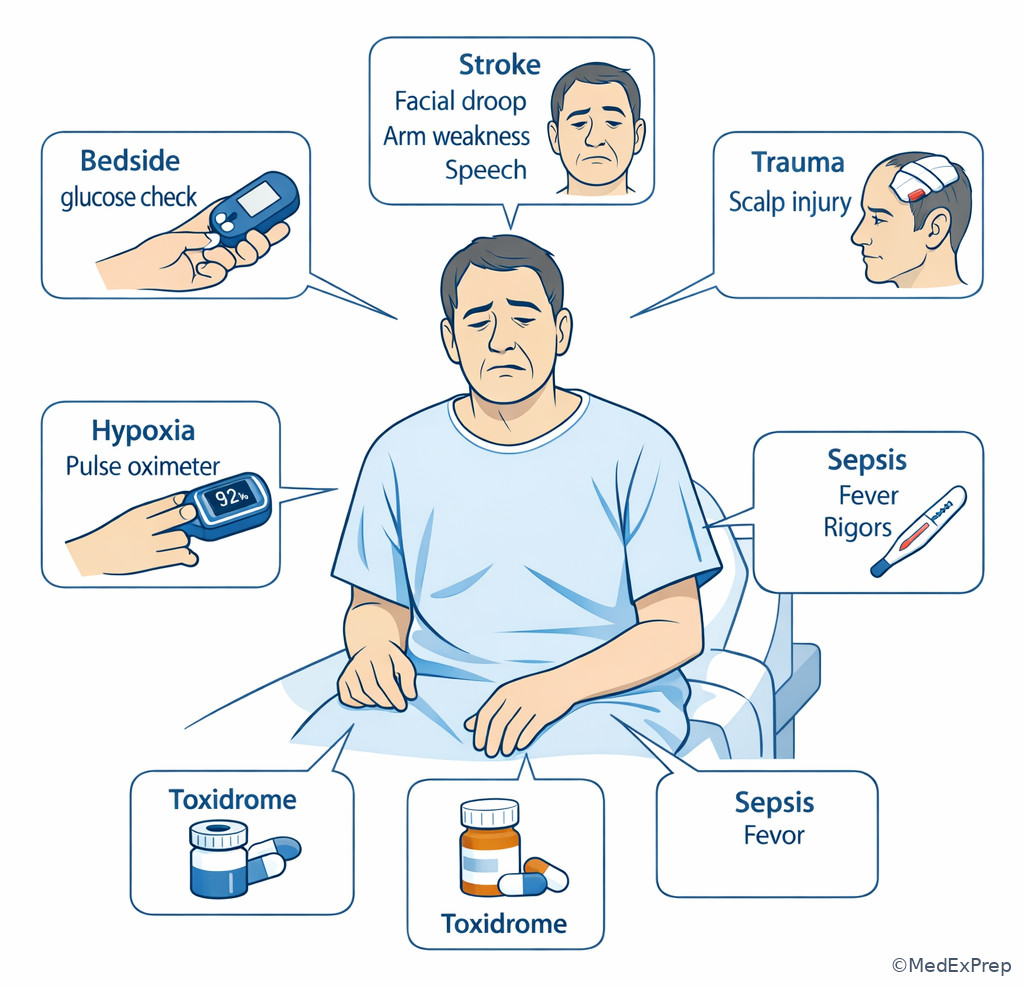
- Hypoxia, hypoglycemia, stroke, toxidrome, and sepsis can all present first as confusion.
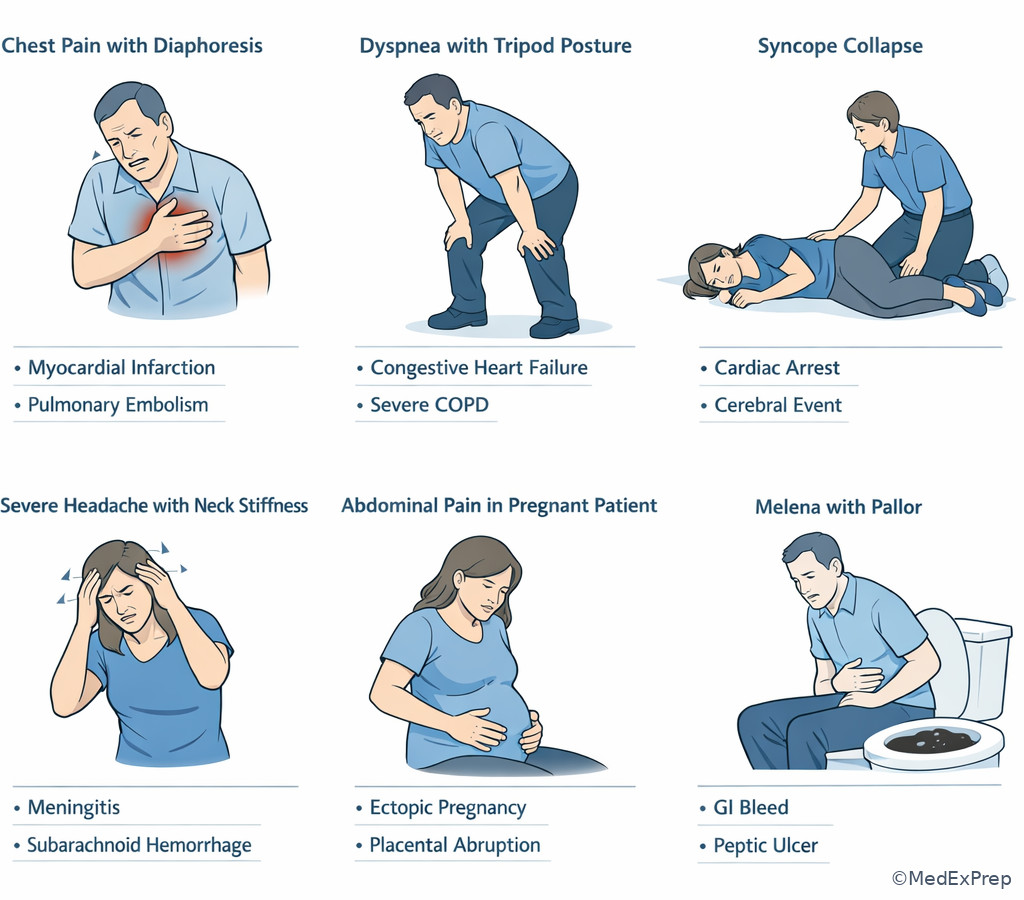
- Chest pain, dyspnea, syncope, severe headache, GI bleeding, and abdominal pain are classic dangerous triage complaints.
- Extremes of age, immunocompromise, pregnancy, and anticoagulation lower the threshold for escalation.
- Trend vitals; a deteriorating pattern matters more than one isolated measurement.
- Pain score alone does not determine acuity; physiologic threat does.
| Domain | Immediate concern | Examples of red flags | Typical triage implication |
|---|---|---|---|
| Airway | Impending obstruction | Stridor, muffled voice, drooling, facial burns, angioedema | Immediate rooming, airway setup, urgent physician involvement |
| Breathing | Respiratory failure | SpO2 low, severe work of breathing, cyanosis, silent chest | Monitor, oxygen/ventilatory support, rapid reassessment |
| Circulation | Shock or hemorrhage | Tachycardia, cool clammy skin, hypotension, weak pulses, syncope | High-acuity placement, IV access, urgent evaluation |
| Neurologic | Brain threat | New focal deficit, seizure, GCS drop, severe agitation/lethargy | Immediate assessment, glucose check, stroke/seizure pathway |
| Exposure/general | Toxic appearance | Pallor, diaphoresis, mottling, rigors, inability to sit upright | Do not leave in waiting room; escalate |
Exam takeaway: Start with instability domains rather than the chief complaint label when deciding urgency.
flowchart TD
A[Patient arrives] --> B{Immediate threat?}
B -->|Airway signs| C[Immediate rooming and airway escalation]
B -->|Breathing distress| D[Oxygen monitor reassess now]
B -->|Perfusion concern| E[Shock or hemorrhage pathway]
B -->|Neuro change| F[Glucose stroke seizure tox check]
B -->|None obvious| G[Focused triage history and repeat vitals]
G --> H{High-risk complaint or vulnerable patient?}
H -->|Yes| I[Low threshold for monitored bed]
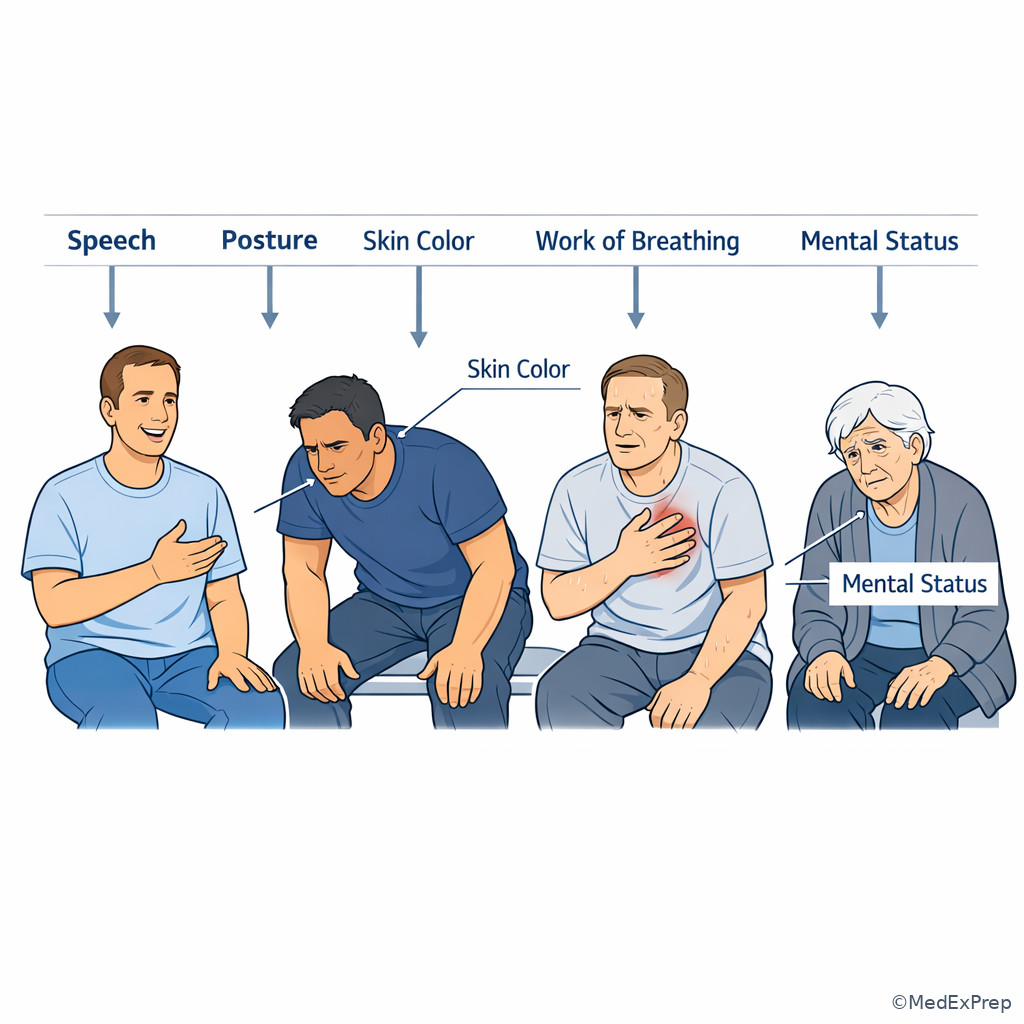
H -->|No| J[Standard workup pathway] Exam takeaway: Appearance, posture, color, and speech often reveal instability before the full history is obtained.
Core content
1.1.1.3 Foundational triage question: stable enough to wait or not?
A Explanation
The central triage conflict is simple: do you continue routine intake, or do you interrupt the normal process because the patient may decompensate? The single rule that resolves this is whether there is any threat to airway, breathing, circulation, or brain function right now. A patient does not need a final diagnosis to be high acuity. They need one of the following: inability to maintain airway, visible respiratory distress, poor perfusion, active major bleeding, or altered mental status.
WHY THIS IS TESTED: exam stems often hide urgent illness behind nonspecific complaints like fatigue, weakness, dizziness, or “not acting right.” The tested skill is choosing escalation before overfocusing on a diagnostic label.
Choose immediate escalation when the patient looks ill, cannot speak normally, seems confused, has abnormal skin perfusion, or has concerning vital sign patterns. Reject the low-acuity pathway when you are reassured only by a normal-looking chief complaint or a single normal systolic pressure. Early shock and respiratory failure can still have preserved blood pressure.
For this first topic, your job is not definitive management. Your job is to recognize that the patient should not remain in the waiting area and needs monitoring, repeat vitals, and physician attention. See Fig 1.
B Worked example
A 67-year-old man presents to urgent care with “indigestion” and mild nausea for 45 minutes. He has diabetes, CKD stage 3, and hypertension. He says the pain is only 3/10 and thinks it started after coffee. He looks pale and keeps pausing mid-sentence. Triage vitals show BP 132/78 mm Hg, HR 112/min, RR 24/min, SpO2 95% on room air, temperature 36.8°C. A distracting clue is that he reports recent spicy food. The tempting wrong move is to place him in a routine queue because the pain sounds mild and the BP is normal.
Reasoning chain: identify task → this is triage acuity, not final diagnosis. Extract key facts → older patient, vascular comorbidity, tachycardia, tachypnea, pallor, interrupted speech. Apply rule → appearance and physiologic stress outweigh the low pain score. Eliminate distractors → reflux is possible but does not explain the ill appearance and abnormal vitals. Verify next step → immediate monitored evaluation, ECG, supervising physician involvement, and high concern for ACS or other cardiopulmonary emergency.
C Exam trap
D Checkpoint
Question: A 58-year-old woman presents with weakness and vomiting. She has heart failure and diabetes. Vitals are BP 118/70 mm Hg, HR 122/min, RR 28/min, SpO2 97%, and she appears cool and diaphoretic. What is the most appropriate triage interpretation?
- A. Low acuity because oxygen saturation is normal
- B. High acuity because tachycardia, tachypnea, and poor perfusion suggest instability
- C. Moderate acuity because vomiting explains the vital sign changes
- D. Low acuity because the blood pressure is not hypotensive
Answer: B
- A: Tempting because normal oxygen saturation can falsely reassure; wrong because breathing and perfusion problems can exist without hypoxemia.
- B: Correct because the triage decision is driven by abnormal physiologic signs and ill appearance, not by one preserved number.
- C: Tempting because vomiting can cause tachycardia; wrong because cool diaphoresis and marked tachypnea push this beyond routine dehydration until proven otherwise.
- D: Tempting because hypotension is a classic shock sign; wrong because compensated shock may precede blood pressure collapse.
1.1.1.4 Vital signs: what matters most and how normal values mislead
A Explanation
The decision conflict here is whether to trust isolated numbers or interpret them in clinical context. The single resolving rule: vital signs are trends plus pattern recognition, not a pass/fail checklist. Tachycardia, tachypnea, fever or hypothermia, hypoxia, narrow pulse pressure, or new hypotension all matter, but so does the story around them. A mildly abnormal heart rate in an anxious patient differs from the same rate in a pale older adult with syncope.
WHY THIS IS TESTED: common board traps present one normal value to distract from a dangerous pattern. A patient can have sepsis with only tachypnea, occult bleeding with only tachycardia, or respiratory failure with normal oxygen saturation early in the course if work of breathing is severe.
Choose high concern when abnormal vitals cluster together, worsen over time, or mismatch the apparent benign complaint. Reject dismissal when the patient is elderly, beta-blocked, immunocompromised, pregnant, or very young; these groups may show blunted or atypical vital sign responses. A normal temperature does not exclude infection, and a normal pulse oximeter reading does not exclude fatigue from impending ventilatory failure.
In triage, repeated measurements are often the discriminator. Trend matters because a patient going from HR 102 to 122/min and RR 20 to 28/min is declaring illness even if the BP remains technically normal. See Fig 2.
Exam takeaway: A concerning pattern across multiple vitals beats one isolated reassuring measurement.
flowchart LR
A[Normal BP] --> B{Still stable?}
B -->|No| C[Tachycardia plus cool skin = possible early shock]
B -->|No| D[Tachypnea plus confusion = possible sepsis or metabolic crisis]
B -->|No| E[Normal SpO2 plus exhaustion = impending ventilatory failure]
B -->|Maybe| F[Reassess trend and appearance]
F --> G[Escalate if worsening or high-risk host] B Worked example
A 24-year-old woman presents with anxiety, shortness of breath, and tingling in her fingers after an argument. She has asthma and recent influenza-like symptoms. Vitals are BP 124/76 mm Hg, HR 118/min, RR 34/min, SpO2 99%, temperature 38.5°C. She is speaking in short phrases. A tempting wrong clue is the history of panic attacks. A distracting lab from urgent care paperwork shows a mildly low potassium. The wrong move is to label this as uncomplicated hyperventilation syndrome based on the tingling and normal saturation.
Reasoning chain: identify task → determine triage acuity and whether a benign explanation is safe. Extract key facts → fever, tachypnea, tachycardia, short phrases, asthma history. Apply rule → clustered abnormal vitals with respiratory complaint do not fit simple anxiety until life threats are excluded. Eliminate distractors → panic attack can mimic dyspnea, but fever and limited speech push toward pulmonary or infectious illness. Verify next step → immediate clinical evaluation and respiratory assessment, not waiting room reassurance.
C Exam trap
D Checkpoint
Question: Which triage finding most strongly argues against dismissing a patient as low acuity despite a normal blood pressure?
- A. Pain score of 9/10
- B. Temperature of 37.2°C
- C. Rising respiratory rate and worsening confusion on reassessment
- D. Chief complaint of nausea for 1 day
Answer: C
- A: Tempting because severe pain deserves attention; wrong because pain intensity alone does not define physiologic instability.
- B: Tempting because learners search for infection clues; wrong because this temperature is not the key discriminator here.
- C: Correct because worsening respiratory rate plus mental status change on trend indicates deterioration.
- D: Tempting because nausea can hide serious disease; wrong because the stem asks for the strongest physiologic reason, and symptom label alone is less discriminating than objective decline.
- True or False: A normal systolic blood pressure excludes shock. False.
- The most concerning trend in triage is not one abnormal number but worsening serial vitals.
- Name 3 signs of increased work of breathing: accessory muscle use, inability to speak full sentences, retractions/tripod posture.
1.1.1.5 High-risk symptoms that should immediately raise acuity
A Explanation
The triage conflict here is whether a common symptom can stay in a routine queue. The resolving rule is: some complaints are high-risk because their dangerous differentials are common, lethal, and easy to miss early. The classic complaints are chest pain, dyspnea, syncope, severe headache, focal neurologic symptoms, GI bleeding, severe abdominal pain, testicular pain, vaginal bleeding in pregnancy, and sudden back pain with systemic symptoms.
WHY THIS IS TESTED: exam stems frequently use vague or softened language such as “pressure,” “indigestion,” “dizzy spell,” or “worst headache after exercise.” The challenge is recognizing the dangerous differential that drives triage priority.
Choose higher acuity when the symptom suggests a short list of cannot-miss conditions: chest pain may represent ACS or dissection; dyspnea may reflect asthma, PE, edema, or pneumothorax; syncope may be arrhythmia, hemorrhage, or PE; headache may be SAH or meningitis; abdominal pain may be AAA, bowel ischemia, ectopic pregnancy, or perforation. Reject the temptation to downgrade because the patient is young, symptoms improved briefly, or the initial exam is not dramatic.
Risk is multiplied by context: pregnancy, anticoagulation, immunosuppression, cancer, recent surgery, older age, and significant cardiopulmonary disease lower the threshold for monitored evaluation. See Fig 3.
Exam takeaway: Common complaints become high acuity when paired with a dangerous differential or vulnerable host.
flowchart TD A[Common ED complaint] --> B[Chest pain] A --> C[Dyspnea] A --> D[Syncope] A --> E[Severe headache] A --> F[Abdominal pain] A --> G[GI bleed or pregnancy bleeding] B --> H[ACS dissection PE] C --> I[Asthma edema PE pneumothorax] D --> J[Arrhythmia hemorrhage PE] E --> K[SAH meningitis stroke] F --> L[AAA ectopic obstruction ischemia] G --> M[Hemorrhagic shock or ectopic] H --> N[Escalate acuity] I --> N J --> N K --> N L --> N M --> N
Exam takeaway: Recognize the symptom clusters that should never be left in a routine waiting pathway.
B Worked example
A 31-year-old pregnant woman at 8 weeks by dates presents with light vaginal bleeding and lower abdominal cramping. She also reports shoulder discomfort after lifting groceries. She has a history of PID and smokes cigarettes. Vitals are BP 108/68 mm Hg, HR 110/min, RR 22/min, SpO2 99%. A tempting wrong clue is that the bleeding is less than a normal period. A distracting detail is that she ate poorly all day and feels weak. The wrong move is to classify this as routine early-pregnancy spotting.
Reasoning chain: identify task → triage acuity for pregnancy-related bleeding. Extract key facts → pregnancy, abdominal pain, tachycardia, ectopic risk factor, shoulder pain. Apply rule → this complaint has a cannot-miss hemorrhagic diagnosis. Eliminate distractors → threatened abortion is possible but does not safely explain the referred pain and risk profile. Verify next step → urgent evaluation for possible ectopic pregnancy; do not leave in low-acuity flow.
C Exam trap
D Checkpoint
Question: Which patient most requires immediate elevation in triage acuity despite only modest symptoms at presentation?
- A. A 19-year-old with sore throat, fever, and odynophagia for 2 days
- B. A 42-year-old with gradual low back pain after lifting boxes
- C. A 63-year-old on anticoagulation with syncope and now mild abdominal discomfort
- D. A 28-year-old with dysuria and urinary frequency
Answer: C
- A: Tempting because throat symptoms can occasionally threaten the airway; wrong because the stem does not suggest airway compromise.
- B: Tempting because back pain can hide serious disease; wrong because this story fits a musculoskeletal mechanism without an immediate red flag.
- C: Correct because syncope plus anticoagulation plus abdominal symptoms raises concern for occult hemorrhage or other high-risk causes.
- D: Tempting because infection matters; wrong because uncomplicated lower urinary symptoms lack the same immediate danger profile.
1.1.1.6 Vulnerable patients and misleading presentations
A Explanation
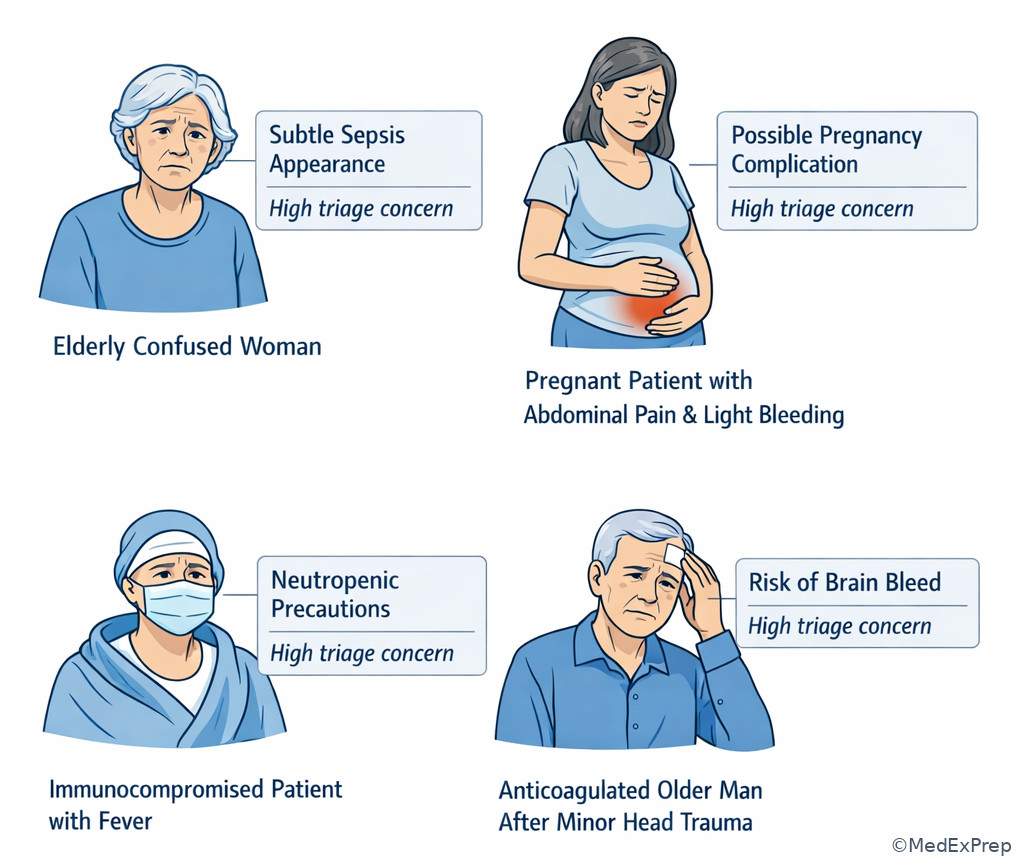
The conflict here is whether to use the same triage threshold for everyone. The rule: certain populations deserve a lower threshold for escalation because they may present atypically or deteriorate faster. These include older adults, infants, pregnant patients, immunocompromised patients, patients on anticoagulants, and patients with major cardiopulmonary disease.
WHY THIS IS TESTED: the exam commonly softens classic findings in these groups. Older adults may have infection without fever, ACS without chest pain, or bleeding without overt hypotension. Immunocompromised patients may have subtle symptoms despite serious infection. Anticoagulated patients with even minor trauma may harbor dangerous bleeding. Pregnant patients can decompensate while vitals still look near-normal.
Choose higher acuity when the host is fragile even if the complaint sounds vague: weakness, confusion, fall, decreased intake, or malaise may be the entry point for sepsis, intracranial bleed, ACS, or metabolic crisis. Reject the trap of attributing acute change to baseline dementia, anxiety, age, or medication side effects without first excluding emergency causes.
This is where triage becomes risk-adjusted rather than symptom-only. A young healthy patient with mild vomiting may wait safely; an older patient on dialysis with the same complaint and confusion should not. See Fig 4.
Exam takeaway: Older age, pregnancy, immunocompromise, and anticoagulation lower the threshold for escalation even with subtle symptoms.
- The elderly patient with infection may have no fever.
- True or False: Minor head trauma on anticoagulation can still be high risk. True.
- Name 3 vulnerable groups needing a lower threshold for escalation: older adults, pregnant patients, immunocompromised patients.
B Worked example
An 81-year-old woman is brought by family for “not acting like herself.” She has dementia, diabetes, and chronic prednisone use for polymyalgia. She denies pain. Triage vitals are BP 126/72 mm Hg, HR 104/min, RR 24/min, temperature 37.4°C, SpO2 96%. She is sleepy but arousable. A tempting wrong clue is the known dementia. A distracting point is that the family reports poor sleep for two nights. The wrong move is to assign low acuity because there is no fever or focal complaint.
Reasoning chain: identify task → determine whether altered baseline in a vulnerable host is high risk. Extract key facts → older adult, immunosuppressive steroid use, mental status change, tachycardia, tachypnea. Apply rule → vulnerable patient with acute change deserves higher acuity and workup for infection, hypoperfusion, metabolic disturbance, or CNS event. Eliminate distractors → dementia does not explain an acute deviation from baseline. Verify next step → urgent evaluation, bedside glucose, broad consideration for sepsis or metabolic causes, not routine waiting.
C Exam trap
D Checkpoint
Question: Which patient should be triaged with the lowest threshold for immediate clinician evaluation?
- A. A 27-year-old with vomiting and no medical history, normal mentation, and HR 96/min
- B. A 33-year-old pregnant patient with mild lower abdominal pain and spotting
- C. A 25-year-old with sore throat and stable vitals
- D. A 40-year-old with chronic migraine requesting refill medication and normal exam
Answer: B
- A: Tempting because vomiting can hide serious disease; wrong because the stem lacks the host risks present in option B.
- B: Correct because pregnancy plus pain and bleeding carries ectopic risk and needs prompt assessment.
- C: Tempting because airway issues can arise from throat complaints; wrong because no airway red flags are given.
- D: Tempting because headache should be respected; wrong because this appears consistent with a chronic pattern and lacks danger cues.
1.1.1.7 Integration: safest first step, reassessment, and disposition from triage
A Explanation
The final triage conflict is what to do next once concern is recognized. The rule is: the safest first step matches the threat. Immediate rooming, monitors, repeat vitals, bedside glucose, ECG, oxygen when indicated, hemorrhage control, and urgent escalation are often the right early actions. Triage is not just sorting; it launches the first protective steps.
WHY THIS IS TESTED: many exam questions ask for the “most appropriate next step” rather than the diagnosis. The best answer is often the action that protects the patient while the differential remains open. If the patient may be unstable, do not choose a slow outpatient-style step.
Choose monitored evaluation and rapid reassessment when you see any unresolved red flag. Choose immediate bedside glucose for altered mental status because hypoglycemia is common, dangerous, and quickly correctable. Choose ECG early for chest pain, syncope, palpitations, or unexplained diaphoresis. Reject time-consuming history expansion when the patient is visibly deteriorating. Reject discharge thinking before the patient has shown stability over time and the dangerous differential has narrowed.
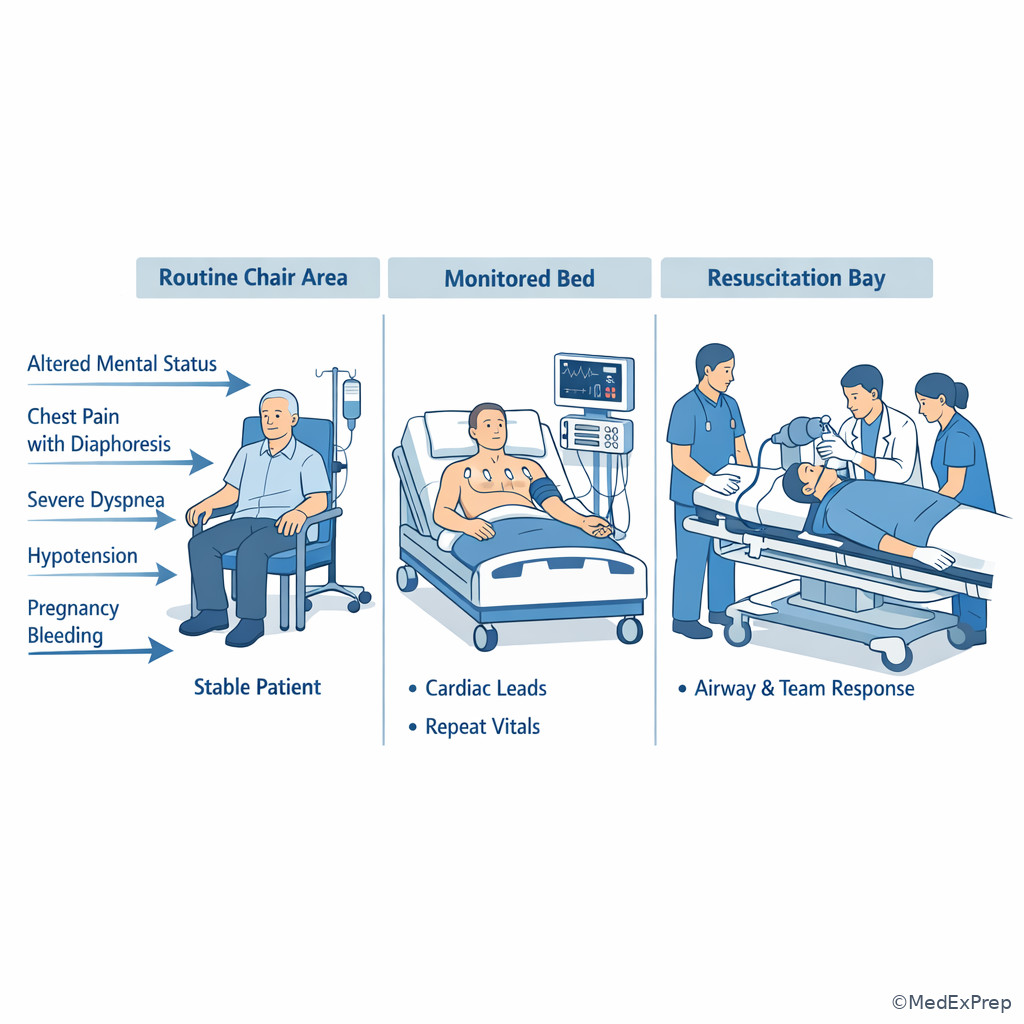
Disposition begins at triage. Some patients need the resuscitation area; others need a monitored bed; some need observation even if the initial complaint sounds mild because their trend or risk factors remain concerning. See Fig 5 and Fig 6.
Exam takeaway: The best next step after recognizing red flags is the fastest action that protects the patient while the diagnosis remains open.
flowchart TD
A[Red flag recognized] --> B{Primary concern}
B -->|Altered mental status| C[Bedside glucose and monitored bed]
B -->|Chest pain syncope diaphoresis| D[Immediate ECG and urgent evaluation]
B -->|Resp distress| E[Oxygen support and respiratory assessment]
B -->|Bleeding or shock signs| F[Hemorrhage control IV access escalation]
B -->|Pregnancy pain/bleeding| G[Urgent pregnancy-focused evaluation]
C --> H[Repeat vitals and reassess]
D --> H
E --> H
F --> H
G --> H
H --> I{Improving and stable?}
I -->|No| J[Immediate supervising physician/team escalation]
I -->|Yes| K[Continue expedited workup] Exam takeaway: Placement decisions depend on physiologic risk, trend, and red flags rather than symptom severity alone.
Exam takeaway: In emergency triage, mental status change should trigger immediate glucose check and rapid search for reversible causes.
Exam takeaway: Increasing respiratory effort can signal impending failure even before severe hypoxemia appears.
B Worked example
A 72-year-old man presents after a brief syncopal episode in the lobby. He has coronary artery disease, atrial fibrillation on apixaban, and recently started a diuretic. He now says he feels “fine” except for mild lightheadedness. Vitals are BP 102/64 mm Hg, HR 54/min, RR 18/min, SpO2 98%. He has a forehead bruise from the fall. A tempting wrong clue is that he recovered quickly. A distracting detail is recent poor oral intake. The wrong move is to attribute the event to dehydration and send him to routine evaluation.
Reasoning chain: identify task → determine safest next step from triage. Extract key facts → syncope, anticoagulation, head injury, cardiovascular disease, relative hypotension/bradycardia. Apply rule → syncope with injury and anticoagulation requires high concern; he needs monitored evaluation and ECG, not delayed intake. Eliminate distractors → dehydration is plausible but does not safely account for the anticoagulation-related bleeding risk and arrhythmia history. Verify next step → urgent rooming, cardiac monitoring, physician involvement, and evaluation for arrhythmia or intracranial bleed.
C Exam trap
D Checkpoint
Question: A 70-year-old man with diabetes is found confused in the waiting area. Which is the most appropriate immediate next step in triage?
- A. Obtain a detailed medication reconciliation before moving him
- B. Arrange outpatient follow-up because confusion is chronic in older adults
- C. Move to a monitored setting and obtain a bedside glucose promptly
- D. Wait for the full physician evaluation before any testing
Answer: C
- A: Tempting because medication issues can cause confusion; wrong because immediate reversible threats come first.
- B: Tempting if the learner assumes baseline dementia; wrong because acute confusion is high risk until proven otherwise.
- C: Correct because bedside glucose is fast, high yield, and directly relevant to a reversible emergency while monitored placement addresses potential instability.
- D: Tempting because some settings sequence tasks that way; wrong because emergency triage should not delay time-sensitive stabilizing actions.
Exam Traps & Differentiators
Most common wrong answer and why: choosing the routine workup pathway because the patient lacks dramatic hypotension or severe pain. This is tempting because learners are trained to look for textbook collapse. In triage, however, subtle tachypnea, ill appearance, confusion, anticoagulation, pregnancy, or a high-risk complaint are often the real discriminator.
| Looks similar | Why it tempts you | Single clue that separates the dangerous patient | Triage implication |
|---|---|---|---|
| Anxiety hyperventilation vs respiratory emergency | Tingling, distress, normal SpO2 | Fever, short-phrase speech, wheeze, chest pain, or severe work of breathing | Upgrade and assess airway/breathing |
| Benign dizziness vs shock/arrhythmia | Patient says “I feel better now” | Syncope, diaphoresis, abnormal pulse, chest symptoms, anticoagulation | Monitored bed and ECG |
| Chronic confusion vs acute encephalopathy | Known dementia or psychiatric history | Acute deviation from baseline, tachypnea, poor intake, or focal deficit | Immediate clinician evaluation and glucose check |
| Gastritis/reflux vs ACS | Epigastric discomfort after food | Diaphoresis, pallor, dyspnea, exertional onset, vascular risk factors | High-acuity chest symptom pathway |
| Threatened abortion vs ectopic pregnancy | Light bleeding and mild cramps | Unilateral pain, shoulder pain, tachycardia, PID/tubal risk factors | Urgent pregnancy-focused evaluation |
| Simple viral illness vs sepsis in older adult | No obvious fever or only vague weakness | Acute confusion, tachypnea, poor perfusion, immunocompromise | Escalate despite muted classic signs |
If the stem says...
- “Normal blood pressure” → think compensated shock may still be present.
- “Looks pale and diaphoretic” → think high acuity even before the diagnosis is known.
- “Not acting like herself” → think acute altered mental status until proven otherwise.
- “Pregnant with pain or bleeding” → think ectopic until excluded.
- “Symptoms resolved after a brief event” → think transient dangerous events still need urgent evaluation.
- “On anticoagulation after fall/syncope” → think hidden bleeding risk.
| Related upcoming topic | Confusable pair | Current lesson focus | Later lesson focus |
|---|---|---|---|
| Airway Breathing Circulation Priorities | Recognizing stridor vs managing stridor | Do not miss the airway red flag at triage | What oxygenation/airway actions come first |
| Unstable Patient Recognition | Tachycardia as triage clue vs shock subtype interpretation | Upgrade acuity based on pattern | Classify shock and resuscitation logic |
| Observation Admission And Discharge | Monitored evaluation vs final disposition | Who cannot safely wait | Who can safely leave after workup and reassessment |
Algorithm / Approach
Rapid Review
- Compensated shock → tachycardia and poor perfusion before hypotension
- Respiratory distress → work of breathing outranks a temporarily normal SpO2
- Altered mental status → acute change from baseline is high acuity until proven otherwise
- Syncope → recovery does not erase arrhythmia or hemorrhage risk
- Pregnancy with pain/bleeding → ectopic risk drives urgency
- Anticoagulated fall → subtle trauma can still mean dangerous bleed
- Elderly infection → confusion or tachypnea may replace fever
- Chest pain equivalent → diaphoresis, nausea, or dyspnea can replace classic pain
- Benign complaint with toxic appearance → appearance wins over symptom label
- Normal BP → never enough to declare stability alone
- Trend → serial worsening beats isolated mild abnormality
- Triage action → best next step is the fastest protective move, not the final diagnosis
Self-check quiz
1. A 64-year-old man presents with “indigestion” and nausea for 30 minutes. He has diabetes and hypertension. He looks pale and diaphoretic, BP is 138/82 mm Hg, HR 108/min, and SpO2 96%. Which triage interpretation is most appropriate?
- A. Low acuity because the blood pressure is normal
- B. Low acuity because the pain is not severe
- C. High acuity because appearance and tachycardia suggest a possible time-sensitive cardiopulmonary emergency
- D. Moderate acuity because GI causes are more likely than cardiac causes
2. A 79-year-old woman with baseline mild dementia is brought in for “sleepiness.” She is more confused than usual, RR 26/min, HR 106/min, temperature 37.3°C, and BP 122/70 mm Hg. Which finding most strongly raises triage concern?
- A. The absence of fever
- B. Acute change from baseline mental status with tachypnea
- C. Her history of dementia
- D. Her age alone without other abnormalities
3. A 28-year-old woman at 7 weeks gestation presents with light vaginal bleeding and left lower quadrant pain. She has a history of PID. BP is 110/68 mm Hg, HR 112/min, and she reports mild shoulder discomfort. What is the most appropriate next triage step?
- A. Routine waiting-room placement because the bleeding is light
- B. Prompt monitored evaluation for possible ectopic pregnancy
- C. Discharge with outpatient obstetric follow-up because the blood pressure is normal
- D. Treat as simple musculoskeletal shoulder strain first
4. A 23-year-old man presents with shortness of breath after an argument. He has asthma and recent viral symptoms. He is febrile to 38.4°C, HR 120/min, RR 32/min, SpO2 99%, and speaking in short phrases. What is the most appropriate triage decision?
- A. Label this a panic attack because oxygen saturation is normal
- B. Assign low acuity because young age lowers risk
- C. Escalate evaluation because work of breathing and fever argue against simple anxiety
- D. Delay evaluation until a full psychiatric history is obtained
5. A 71-year-old man with CAD and atrial fibrillation on apixaban has brief syncope in the lobby and now feels better. He struck his head on the floor. BP 104/66 mm Hg, HR 56/min. Which is the most appropriate next step?
- A. Routine evaluation because the episode resolved
- B. Monitored placement with urgent ECG and clinician evaluation
- C. Oral hydration in the waiting room
- D. Discharge if he can ambulate without dizziness
6. A 68-year-old woman presents with weakness and vomiting. She has heart failure, CKD, and diabetes. BP 116/72 mm Hg, HR 124/min, RR 30/min, SpO2 97%, skin cool and clammy. Which single feature most strongly supports high-acuity triage despite the normal blood pressure?
- A. Vomiting for 1 day
- B. Cool clammy skin with marked tachycardia and tachypnea
- C. History of diabetes alone
- D. Oxygen saturation above 95%
7. A 74-year-old immunocompromised man on chronic prednisone presents with malaise and decreased appetite. Family says he is less interactive today. Temperature 37.1°C, HR 108/min, RR 24/min, BP 124/74 mm Hg. Which interpretation is most appropriate?
- A. Low acuity because there is no fever
- B. High acuity because vulnerable hosts may have subtle sepsis or metabolic emergencies
- C. Low acuity because malaise is nonspecific
- D. Routine evaluation because blood pressure is preserved
8. A 66-year-old man with diabetes is found confused in triage. He is pale, sweaty, and unable to answer questions reliably. BP 128/76 mm Hg, HR 102/min, RR 22/min, SpO2 98%. Which immediate action best reflects emergency triage priorities?
- A. Move to monitored care and obtain a bedside glucose
- B. Wait for full laboratory results before acting
- C. Reassure family because the blood pressure is normal
- D. Send him back to the waiting area after a brief interview
Answer key
1.1.1.8 1. Question 1
Correct answer: C
- A: Tempting because learners often use hypotension as the threshold for emergency concern. Incorrect for this scenario because preserved blood pressure does not exclude ACS or compensated shock. Single clue: pallor and diaphoresis with tachycardia. Source: Tintinalli; AHA/ACC ACS guidance.
- B: Tempting because low pain intensity can seem reassuring. Incorrect because pain severity does not reliably correlate with acuity, especially in diabetic patients who may have atypical ischemia. Single clue: ill appearance despite mild symptom description. Source: Harrison’s; AHA/ACC.
- C: Correct because the mechanism-to-treatment logic is possible acute coronary or other cardiopulmonary pathology with sympathetic stress signs, which requires prompt monitored evaluation and ECG. Single clue: pale, diaphoretic appearance. Source: AHA/ACC chest pain guidance; Tintinalli.
- D: Tempting because indigestion is a real GI presentation. Incorrect because triage should not prefer benign GI diagnoses over time-sensitive cardiac causes in a high-risk patient with alarming appearance. Single clue: vascular risk factors plus autonomic symptoms. Source: AHA/ACC; Harrison’s.
1.1.1.9 2. Question 2
Correct answer: B
- A: Tempting because fever is associated with infection screening. Incorrect because older adults may have serious infection or encephalopathy without fever. Single clue: abnormal mentation and tachypnea matter more than absent fever. Source: Tintinalli; Harrison’s.
- B: Correct because acute change from baseline mental status plus tachypnea signals high acuity and possible sepsis, metabolic derangement, or hypoperfusion. Single clue: “more confused than usual.” Source: Tintinalli; Sepsis literature.
- C: Tempting because dementia commonly causes chronic confusion. Incorrect because the key issue is acute deviation, not the existence of baseline impairment. Single clue: family notes a new change. Source: Harrison’s.
- D: Tempting because advanced age increases baseline risk. Incorrect because age alone is less discriminating than the combination of acute mental-status change and tachypnea. Single clue: physiologic abnormality plus acute change. Source: Tintinalli.
1.1.1.10 3. Question 3
Correct answer: B
- A: Tempting because the bleeding is light and the patient is not frankly hypotensive. Incorrect because early ectopic pregnancy can present subtly before decompensation. Single clue: unilateral pain with tachycardia and PID history. Source: ACOG-oriented emergency references; Tintinalli.
- B: Correct because the pathophysiologic concern is ectopic implantation with possible intra-abdominal bleeding; prompt monitored evaluation is safer than routine waiting. Single clue: pregnancy plus pain/bleeding plus shoulder discomfort. Source: Tintinalli; Harrison’s.
- C: Tempting because blood pressure is normal. Incorrect because normal pressure does not exclude evolving hemorrhage. Single clue: tachycardia with classic ectopic risk factors. Source: Tintinalli.
- D: Tempting because shoulder pain can be musculoskeletal. Incorrect because in this reproductive context, referred pain raises concern for diaphragmatic irritation from bleeding. Single clue: associated pregnancy-related symptoms. Source: Harrison’s.
1.1.1.11 4. Question 4
Correct answer: C
- A: Tempting because panic attacks can cause dyspnea, tingling, and tachypnea. Incorrect because fever and short-phrase speech argue for a respiratory or infectious process, not isolated anxiety. Single clue: febrile respiratory distress. Source: Tintinalli; respiratory emergency references.
- B: Tempting because younger patients often appear lower risk. Incorrect because age does not neutralize abnormal work of breathing. Single clue: speaking in short phrases. Source: Tintinalli.
- C: Correct because the mechanism is increased respiratory effort with possible asthma exacerbation or infection; urgent assessment is required even with normal oxygen saturation. Single clue: severe tachypnea with limited speech. Source: Tintinalli; asthma guidelines.
- D: Tempting because stress triggered the symptoms. Incorrect because psychiatric evaluation follows medical stabilization when respiratory danger is possible. Single clue: fever and asthma history. Source: Tintinalli.
1.1.1.12 5. Question 5
Correct answer: B
- A: Tempting because the patient feels better and transient syncope is often benign. Incorrect because syncope with anticoagulation, head injury, and cardiac history is high risk. Single clue: apixaban plus head strike. Source: Tintinalli; syncope risk references.
- B: Correct because the likely mechanisms include arrhythmia or occult bleeding; monitored placement and urgent ECG are the appropriate first protective steps. Single clue: syncope in a patient with atrial fibrillation history and anticoagulation. Source: Tintinalli; AHA rhythm/syncope guidance.
- C: Tempting because volume depletion can cause syncope. Incorrect because dehydration does not safely explain away the bleeding and arrhythmic risks. Single clue: forehead bruise with anticoagulation. Source: Harrison’s.
- D: Tempting because ambulatory recovery seems reassuring. Incorrect because high-risk syncope requires urgent evaluation rather than functional screening alone. Single clue: high-risk event plus comorbidity profile. Source: Tintinalli.
1.1.1.13 6. Question 6
Correct answer: B
- A: Tempting because vomiting may indicate dehydration or GI illness. Incorrect because the question asks for the strongest sign of current instability, and symptom duration alone is weaker. Single clue: physiologic distress signs are more important than complaint label. Source: Tintinalli.
- B: Correct because cool clammy skin with marked tachycardia and tachypnea indicates sympathetic compensation and poor perfusion, classic for early shock states despite normal BP. Single clue: skin perfusion plus clustered vitals. Source: Harrison’s; Tintinalli.
- C: Tempting because diabetes increases risk for serious disease. Incorrect because comorbidity alone is less discriminating than current perfusion abnormalities. Single clue: objective signs outrank background risk. Source: Harrison’s.
- D: Tempting because normal oxygenation can reassure. Incorrect because adequate oxygen saturation does not exclude shock or metabolic crisis. Single clue: normal SpO2 does not offset shock signs. Source: Tintinalli.
1.1.1.14 7. Question 7
Correct answer: B
- A: Tempting because fever is a classic infection marker. Incorrect because immunocompromised or older patients may not mount a fever despite serious infection. Single clue: chronic prednisone use. Source: Harrison’s; Tintinalli.
- B: Correct because the mechanism is impaired host response and atypical presentation, making subtle sepsis or metabolic emergencies more likely and more dangerous. Single clue: vulnerability plus acute decreased interaction with tachypnea. Source: Tintinalli; emergency infection references.
- C: Tempting because malaise is nonspecific. Incorrect because in vulnerable hosts, nonspecific symptoms are often the presenting face of serious disease. Single clue: immunosuppression changes pretest probability. Source: Harrison’s.
- D: Tempting because blood pressure remains normal. Incorrect because early sepsis or hypoperfusion can exist before hypotension develops. Single clue: tachycardia and tachypnea with altered interaction. Source: Tintinalli.
1.1.1.15 8. Question 8
Correct answer: A
- A: Correct because altered mental status with diaphoresis in a patient with diabetes raises immediate concern for hypoglycemia and other reversible emergencies; monitored placement plus bedside glucose is fast and protective. Single clue: confusion with diabetes and sweating. Source: Tintinalli; ADA emergency references.
- B: Tempting because definitive labs are useful. Incorrect because triage must address immediately reversible causes first; waiting delays care. Single clue: bedside glucose is a time-critical screening tool. Source: Tintinalli.
- C: Tempting because blood pressure appears normal. Incorrect because acute confusion itself is a high-acuity sign and BP does not rule out neurologic or metabolic emergencies. Single clue: unreliable answers and diaphoresis. Source: Harrison’s.
- D: Tempting if the learner underestimates the risk. Incorrect because a confused patient may deteriorate and cannot safely remain unmonitored. Single clue: altered mental status at triage. Source: Tintinalli.