Why it matters
- The chief complaint is the first sorting tool in an OSCE station: it tells you whether the task is pain triage, routine care, trauma assessment, infection screening, or communication.
- Many wrong answers come from treating the patient’s requested procedure instead of the problem hidden inside the complaint.
- Red-flag wording such as “can’t swallow,” “rapid swelling,” or “woke me from sleep” changes priority faster than radiographs or treatment preferences.
- Good chief complaint analysis prevents unsafe shortcuts, especially before the later steps of medical history, medication review, and definitive treatment planning.
Key Terms & Must-Know Facts
1.1.1.1 Key terms
- Chief complaint (CC): The patient’s main reason for seeking care, ideally in the patient’s own words.
- History of present illness (HPI): The structured expansion of the complaint using targeted symptom questions.
- Provoked pain: Pain triggered by stimulus such as cold, heat, biting, or sweets.
- Spontaneous pain: Pain that occurs without an obvious trigger.
- Referred pain: Pain perceived away from the true source.
- Red flag: A history element suggesting emergency risk, spreading infection, airway concern, systemic instability, or non-routine referral threshold.
- Urgent dental complaint: A problem needing prompt evaluation, often same day, to control pain, infection, or risk.
- Elective concern: A patient-centered preference or routine need that can wait if safety issues are present.
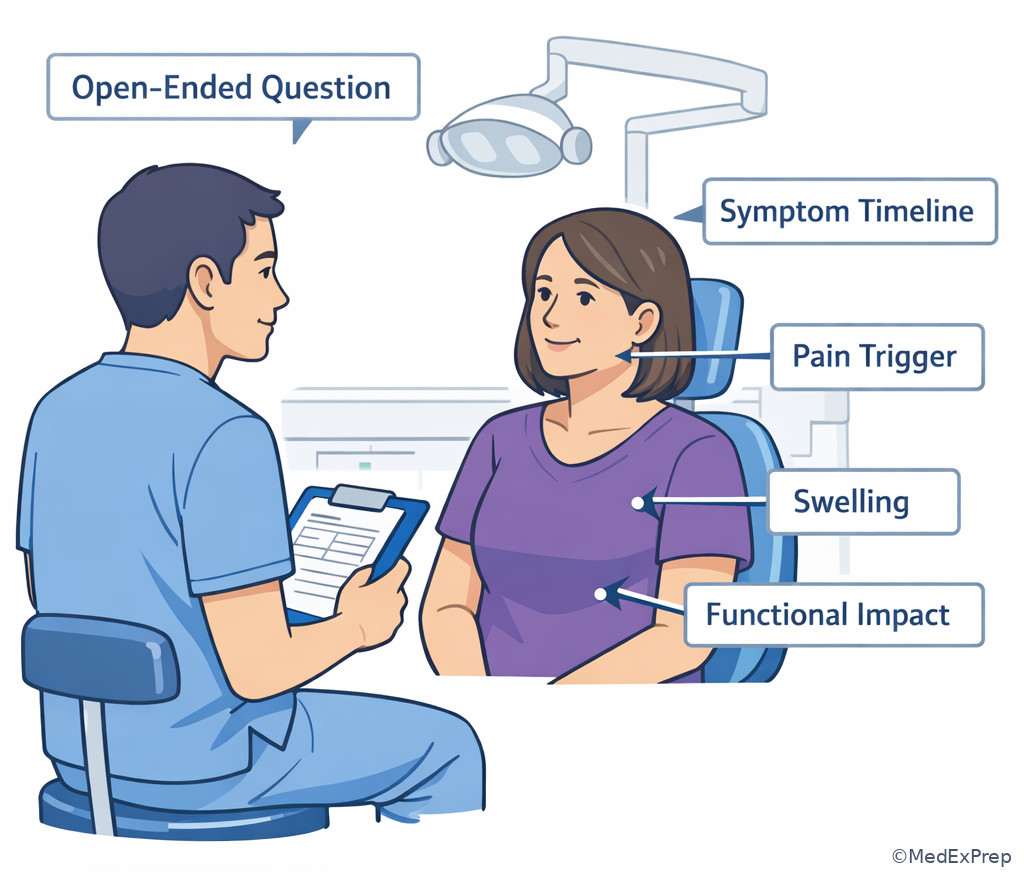
- Open-ended question: A question that lets the patient describe the problem without being led.
- Closed-ended question: A question used to confirm specific features after the initial narrative.
- Pain chronology: Timing, duration, onset, frequency, and progression of symptoms.
- Functional impact: Effect on eating, sleeping, speaking, opening, swallowing, or daily activity.
- Best next step: The safest immediate action based on the complaint and available findings.
1.1.1.2 Must-know facts
- Chart the chief complaint in the patient’s own words when possible, then translate it into a clinical question.
- The complaint is not automatically the diagnosis; “I need a filling” may hide irreversible pulpitis, fracture, or sinus-related pain.
- Red flags outrank treatment preference.
- Open first, narrow second: start broad, then ask targeted follow-up questions.
- On boards, spontaneous, lingering, poorly localized pain usually matters more than cosmetic dissatisfaction.
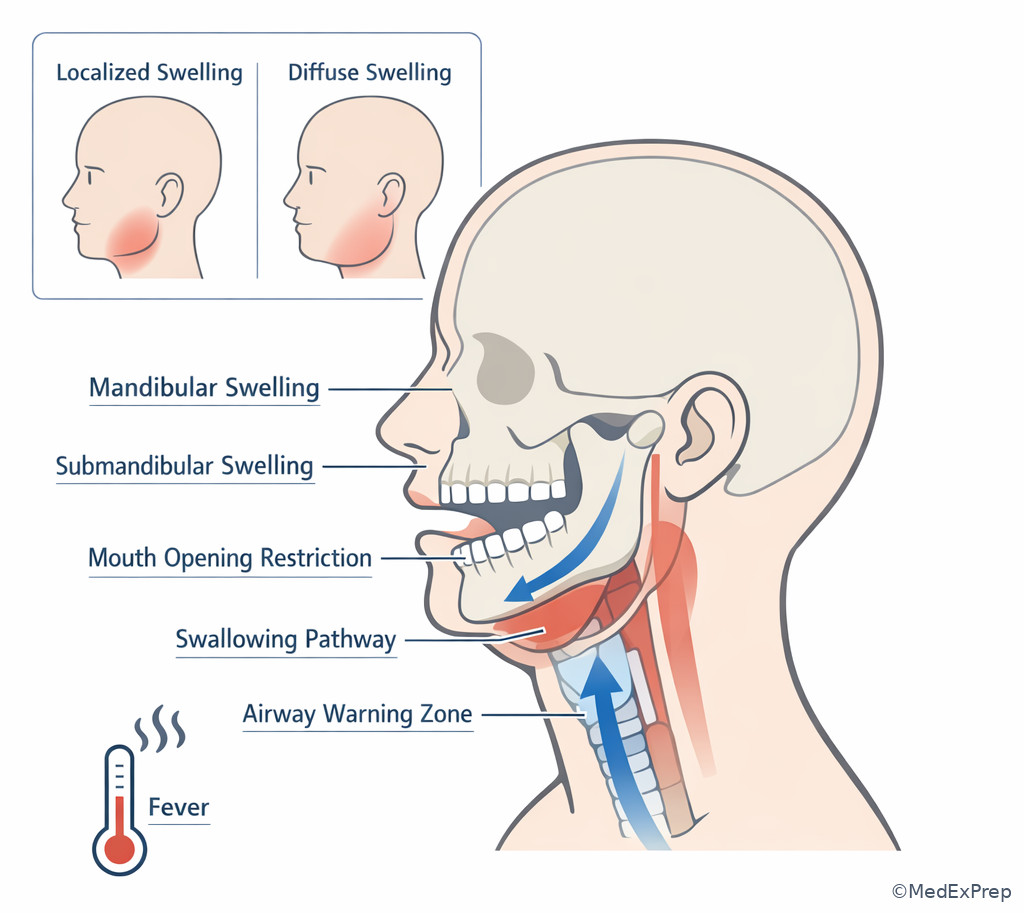
- Swelling plus fever, malaise, dysphagia, or trismus raises urgency.
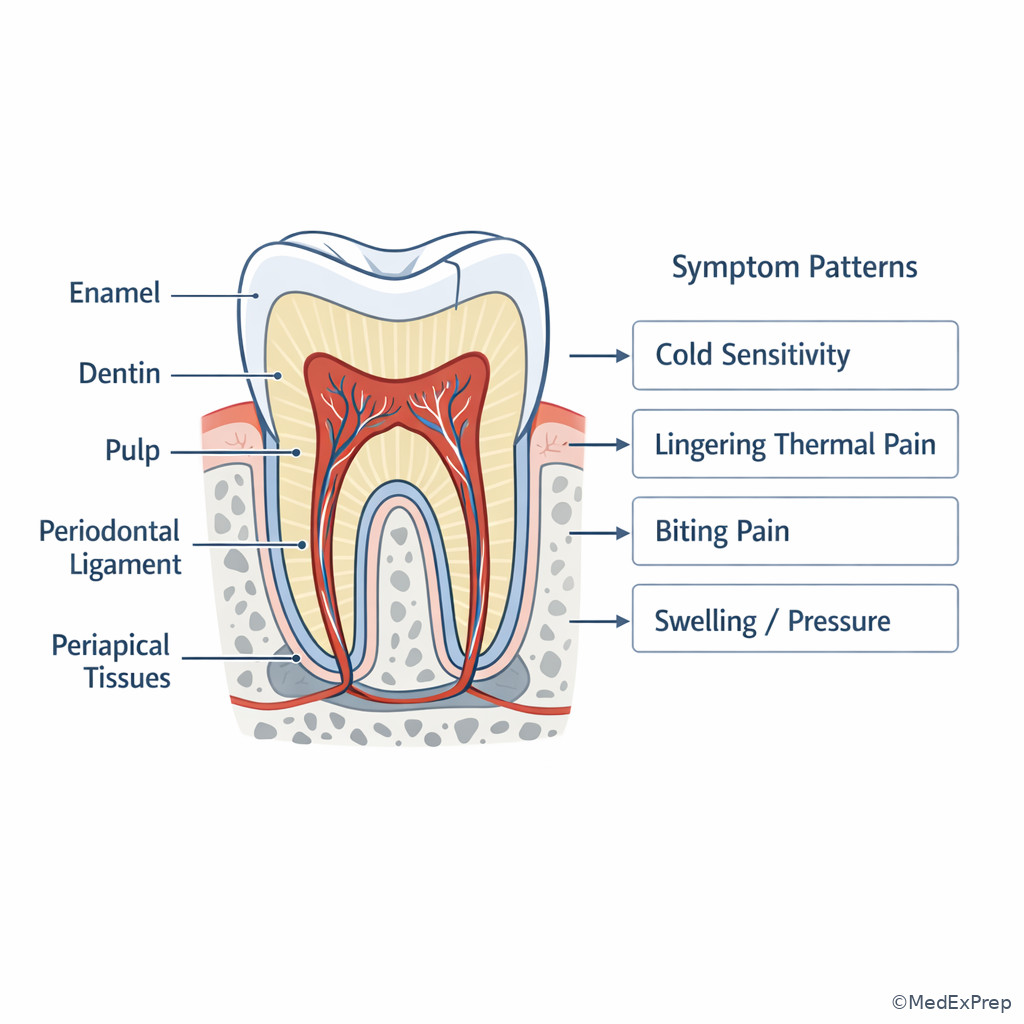
- Biting pain suggests crack, high occlusion, apical inflammation, or periodontal involvement more than simple reversible sensitivity.
- Cold sensitivity that resolves immediately points differently from pain that lingers after stimulus removal.
- The safest answer may be urgent evaluation, deferral, consultation, or emergency referral rather than definitive treatment.
- Chief complaint analysis is incomplete until you identify the task: diagnose, triage, stabilize, reassure, refer, or proceed with routine care.
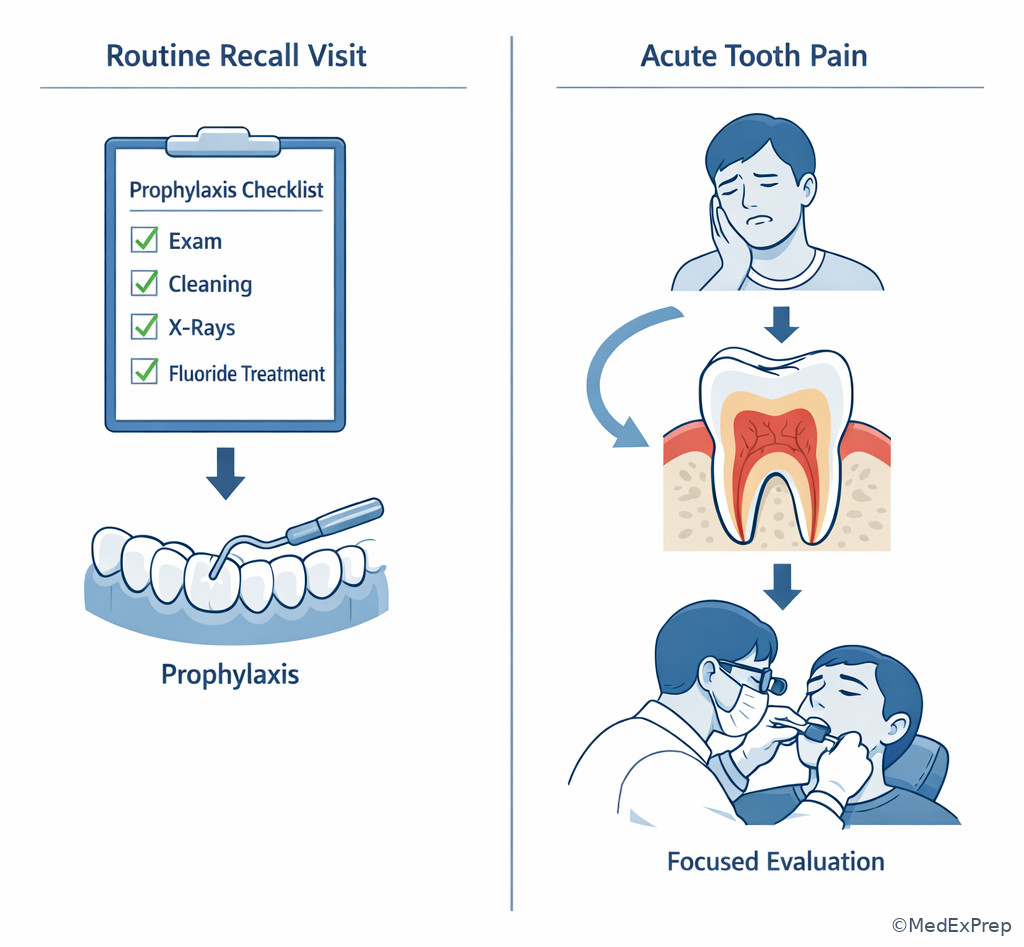
Exam takeaway: Start by deciding whether the complaint signals routine care, urgent dental care, or emergency escalation before choosing any procedure.
flowchart TD
A[Patient opening statement] --> B{Red flag features?}
B -->|Yes| C[Assess airway/systemic risk]
C --> D[Emergency referral or urgent same-day escalation]
B -->|No| E{Pain, swelling, trauma, bleeding, function loss?}
E -->|Yes| F[Focused symptom analysis]
F --> G[Exam and targeted tests]
G --> H[Best next step: stabilize, diagnose, treat, or refer]
E -->|No| I[Routine/elective concern]
I --> J[Comprehensive assessment and sequencing] Exam takeaway: Use neutral posture and focused questioning to obtain accurate symptom details without leading the patient.
Core content
1.1.1.3 Define the complaint before you solve it
A Explanation
The first decision conflict is simple but heavily tested: Do you act on the patient’s requested treatment, or do you first clarify the problem? The correct move is to clarify the problem. A patient saying “I need a crown,” “I want this tooth pulled,” or “my filling fell out” is giving you a starting point, not a final plan. The single rule that resolves the conflict is this: the chief complaint identifies the task; it does not authorize the procedure. In DLOSCE-style reasoning, you must translate the patient’s words into a clinical target: pain source, swelling source, trauma pattern, esthetic concern, functional issue, or preventive request.
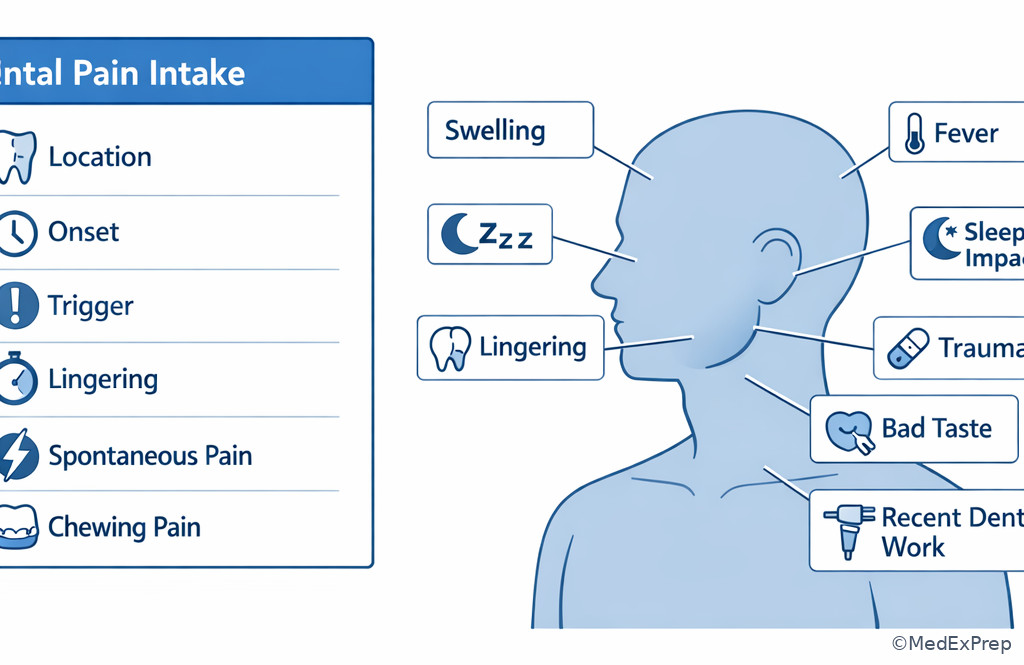
Start with an open-ended invitation: “Tell me what brought you in today.” Then narrow the history with focused questions about onset, location, quality, severity, duration, triggers, progression, associated swelling, fever, bad taste, trauma, and impact on chewing or sleep. If the complaint is nonpainful, ask what change the patient noticed, how long it has been present, and whether it bleeds, grows, or interferes with function. This preserves diagnostic neutrality and avoids anchoring too early.
WHY THIS IS TESTED: Boards want to know whether you can avoid premature closure. The testable pattern is a patient request that sounds specific but hides a different clinical problem. See Fig 1.
Key rule: Document the complaint in the patient’s own words, then restate it clinically: “Patient reports lower right tooth pain for 3 days, triggered by cold and chewing, worse at night.” That is far more defensible than charting “needs extraction.”
Memory anchor: Use SOFT-T for the first pass of chief complaint analysis: Site, Onset, Function impact, Trigger, Time course. Add red flags immediately if present.
Exam takeaway: Convert the patient’s request into a neutral clinical question before you consider treatment.
B Worked example
A 43-year-old man presents saying, “I’m here for an extraction on the upper left.” He has obesity and seasonal allergies. He mentions he took ibuprofen before arrival and notes a “sinus headache” last week. He works night shifts and says the tooth “feels loose” when he bites bread. No swelling is visible. The tempting clue is the patient’s direct request for extraction; the distracting detail is the recent sinus pressure.
Reasoning chain: Identify task: not “perform extraction,” but determine why he wants one. Extract key facts: upper left, biting discomfort, possible mobility sensation, recent sinus symptoms, no obvious swelling, self-medicated pain. Apply rule: patient request does not equal indicated treatment. Eliminate distractors: immediate extraction is premature; routine prophylaxis ignores the pain complaint; attributing everything to sinusitis is unsupported without exam. Verify best answer: obtain focused history and perform targeted clinical and radiographic evaluation before deciding treatment.
A board-safe response would be: “I want to understand exactly what that tooth is doing before we decide whether extraction is the right option.” That shows patient-centered communication and defensible sequencing.
C Exam trap
Common wrong answer: Proceeding directly with the patient’s requested procedure.
Why it is tempting: The patient sounds certain, and the request appears efficient.
Single clue that eliminates it: There has been no focused symptom analysis or diagnostic confirmation; on the exam, skipping assessment is unsafe and indefensible.
D Checkpoint
Question: A 29-year-old patient says, “My filling came out, so I just need it replaced today.” She has mild asthma and reports that the tooth now hurts only when she drinks cold water, with the pain ending right away. Which is the most appropriate next step?
- Replace the restoration immediately — tempting because the patient identifies a lost filling, but wrong because symptom clarification and exam still come first.
- Begin antibiotics because cold sensitivity suggests infection — tempting because pain is present, but wrong because isolated brief cold sensitivity does not itself justify antibiotics.
- Obtain focused history and examine the tooth before selecting treatment — tempting and correct because the complaint names a possible cause, not the final management decision.
- Refer for emergency hospital evaluation — tempting if any pain is overcalled as urgent, but wrong because no airway, systemic, or spreading infection red flags are given.
Practitioner Action: Assess the patient’s own words, then clarify onset, trigger, progression, and function. Intervene by reframing the request into a diagnostic task. Refer only if red flags or out-of-scope findings appear. Document the complaint verbatim plus your clinical restatement and immediate triage decision.
1.1.1.4 Extract the discriminating symptom pattern
A Explanation
The next decision conflict is which symptom detail actually changes your differential and next step? Students often collect many facts but miss the one that matters most. In chief complaint analysis, the highest-yield details are timing, trigger, duration after stimulus, spontaneity, localization, and whether pain is associated with chewing, swelling, or sleep interruption. These details narrow what kind of evaluation you prioritize. For example, brief cold sensitivity points in a different direction from spontaneous throbbing pain that lingers or wakes the patient.
Use a structured symptom grid. Ask: Where is it? When did it start? What triggers it? Does it linger? Can the patient point to one tooth? Is chewing involved? Is there swelling, fever, bad taste, trauma, or recent dental treatment? Can the patient sleep? Did the problem worsen or fluctuate? This pattern-based approach is more useful than asking random questions. It helps you decide whether the complaint sounds like dentin sensitivity, pulpal pain, cracked tooth, occlusal trauma, periodontal tenderness, periapical involvement, or a nonodontogenic mimic requiring broader thinking.
WHY THIS IS TESTED: The exam often gives several true statements, but only one symptom pattern should drive the best next step. The testable pattern is choosing between plausible diagnoses based on a single discriminating clue.
Recall: This is the first topic in the course, so there is no prior topic to build from. As you move into Medical History Risk Flags and Medication And Allergy Review, you will layer systemic and pharmacologic modifiers onto this same symptom framework.
High-Yield Connection: This concept is tested alongside Dental Pain Differentials and Pulpal Diagnosis Terms. Know both the symptom pattern and the appropriate follow-up test on exam day — they are frequently paired in stems.
Exam takeaway: In pain complaints, the trigger-duration pattern often separates the best next diagnostic direction.
B Worked example
A 34-year-old woman presents with “tooth pain on the right.” She has controlled hypothyroidism and gastroesophageal reflux disease. She says cold drinks cause pain in a lower molar, but the pain stops within seconds after she swallows. She also mentions occasional jaw clenching at work and points out a new whitening toothpaste. No swelling, fever, or spontaneous pain is reported. The tempting-but-wrong clue is the clenching history, which can push students toward occlusal trauma without enough support.
Reasoning chain: Identify task: characterize the symptom pattern. Extract key facts: cold-triggered, brief, no lingering, no spontaneous pain, no swelling, no sleep disturbance. Apply rule: brief stimulus-provoked pain that ends quickly points away from more advanced pulpal urgency. Eliminate distractors: antibiotics are unsupported; emergency referral is unnecessary; extraction discussion is premature. Verify: focused examination for caries, exposed dentin, defective restoration, or cervical sensitivity is the appropriate next step.
The point is not to make a final endodontic diagnosis from history alone. The point is to choose the right diagnostic lane.
C Exam trap
Common wrong answer: Equating any temperature sensitivity with severe infection.
Why it is tempting: Candidates overlearn that pain equals pathology requiring urgent treatment.
Single clue that eliminates it: The pain is brief and stimulus-bound rather than lingering or spontaneous.
D Checkpoint
Question: Which complaint pattern most strongly supports prioritizing a more urgent pulpal/periapical workup over routine sensitivity evaluation?
- Cold pain that ends immediately after the drink is removed — tempting because temperature sensitivity is present, but wrong because the nonlingering pattern is less urgent.
- Dull pressure after chewing crusty bread one time last week — tempting because biting pain matters, but wrong because isolated mild chewing discomfort is less concerning than spontaneous lingering pain.
- Spontaneous night pain that lingers after heat and is hard to localize — tempting and correct because spontaneous, lingering, poorly localized pain raises concern for a more advanced pulpal process needing focused urgent workup.
- Sensitivity to sweets around an exposed root surface — tempting because it may be painful, but wrong because this pattern more often fits localized dentin sensitivity.
Practitioner Action: Assess timing, trigger, duration, localization, and function impact for every pain complaint. Intervene with targeted clinical tests guided by the pattern, not by habit. Refer if the pattern suggests nonroutine infection, trauma, or nonodontogenic concern beyond entry-level immediate care. Document the symptom pattern in concise chart language that supports your differential.
- The most useful first distinction in pain history is often provoked vs spontaneous.
- True or False: A patient request for extraction can be accepted as the final treatment plan before evaluation. False.
- Name 3 key symptom discriminators: trigger, duration after stimulus, and functional impact.
Exam takeaway: Use trigger, lingering, localization, and swelling to narrow the complaint before you choose tests or treatment.
flowchart LR
A[Pain complaint] --> B{Trigger?}
B -->|Cold/sweets| C{Lingering?}
C -->|No| D[Consider superficial sensitivity/caries/exposed dentin]
C -->|Yes| E[Prioritize pulpal evaluation]
B -->|Biting| F[Consider crack/occlusion/apical or periodontal source]
B -->|Spontaneous/night| G[Higher concern for pulpal urgency]
A --> H{Swelling/fever/trismus?}
H -->|Yes| I[Escalate urgency]
H -->|No| J[Continue focused exam] Exam takeaway: Matching common symptom triggers to likely tooth structures improves early differential narrowing.
1.1.1.5 Recognize red flags that change urgency
A Explanation
Now the decision conflict becomes urgent dental issue vs emergency risk vs routine complaint. This is where patient safety dominates. Some complaints can wait for a standard exam; others require same-day urgent dental attention; a smaller group requires emergency referral because the risk is no longer just dental pain. The single rule that resolves the conflict is: if the complaint suggests airway compromise, rapidly spreading infection, significant systemic illness, uncontrolled bleeding, or concerning trauma compromise, escalation outranks definitive office treatment.
Red-flag complaint elements include rapidly increasing swelling, trouble swallowing, trouble breathing, inability to handle secretions, trismus limiting function, fever with facial swelling, malaise with odontogenic symptoms, diffuse rather than localized swelling, postextraction bleeding that does not stop with appropriate pressure, facial trauma with occlusal change or suspected fracture, and severe pain with systemic toxicity. In these situations, an entry-level general dentist candidate should think stabilization, referral, emergency activation when indicated, and clear documentation. You are not expected to manage as the physician or specialist of record.
This section is foundational because many DLOSCE mistakes happen when learners are too procedure-focused. A patient asking for “just antibiotics” or “just something for pain” may actually be describing a red-flag emergency pattern that requires a different level of care.
WHY THIS IS TESTED: The exam wants proof that you will not proceed with routine dentistry when the complaint itself signals danger. See Fig 1 and Fig 3.
Key rule: Swelling plus dysphagia, airway symptoms, rapidly progressive spread, or systemic toxicity is an escalation problem first and a dental procedure problem second.
Memory anchor: Think AIR-SWELL: Airway symptoms, Increasing size, Restricted opening; Swallowing difficulty, Whole-face or diffuse spread, Elevated temperature/ill appearance, Lingering systemic symptoms, Low threshold to escalate.
Exam takeaway: Red-flag symptoms move the complaint from routine diagnosis to urgent stabilization or emergency referral.
B Worked example
A 52-year-old woman presents late in the day saying, “I think I just need antibiotics for a tooth.” She has type 2 diabetes and hypertension. She reports lower right facial swelling that “got a lot bigger today,” difficulty swallowing solid food, and trouble opening fully. She also mentions she had a root canal on another tooth years ago, a distracting clue that does not explain the current urgency. Her temperature in clinic is 100.8°F.
Reasoning chain: Identify task: determine urgency, not choose a routine dental procedure. Extract key facts: rapidly progressive swelling, dysphagia, trismus, fever, systemic risk modifier of diabetes. Apply rule: possible spreading odontogenic infection with deeper space concern requires escalation. Eliminate distractors: routine exam and delayed follow-up are unsafe; simply prescribing medication without escalation ignores airway/systemic risk; definitive specialist-level management is beyond entry-level general dentist scope. Verify best answer: urgent emergency evaluation/referral pathway with appropriate stabilization steps and clear communication.
The correct exam mindset is safety first, scope-aware second, procedure last.
C Exam trap
Common wrong answer: Managing a potentially spreading infection as a routine localized toothache.
Why it is tempting: The patient frames the visit as “just antibiotics,” and candidates sometimes anchor on a familiar office-level dental pain workflow.
Single clue that eliminates it: Dysphagia or airway-related functional change is a red flag that upgrades urgency immediately.
D Checkpoint
Question: Which complaint most requires immediate escalation beyond routine same-day dental evaluation?
- Cold sensitivity in a premolar that resolves quickly — tempting because pain is present, but wrong because this is not an emergency pattern.
- Localized gingival tenderness after popcorn impaction — tempting because it is acute, but wrong because it lacks airway or systemic red flags.
- Facial swelling with difficulty swallowing and progressive trismus since morning — tempting and correct because these features suggest a potentially dangerous spreading infection pattern requiring urgent escalation.
- Lost temporary crown with mild chewing discomfort — tempting because it may need prompt follow-up, but wrong because it does not carry the same risk threshold.
Practitioner Action: Assess for swelling spread, swallowing, breathing, fever, and trismus in every infection-related complaint. Intervene by prioritizing stabilization and appropriate urgent disposition. Refer to emergency services or appropriate specialist when findings exceed routine ambulatory general dentistry scope. Document red-flag symptoms, vital signs if available, advice, and referral instructions.
1.1.1.6 Separate urgent symptoms from routine and elective concerns
A Explanation
Another frequent board conflict is what the patient wants today vs what should actually happen today. A patient may present for whitening, a recall exam, or “just to discuss implants,” but the chief complaint may uncover active pain, swelling, trauma, or bleeding that changes sequence. The reverse also occurs: a patient dramatizes a nonurgent sensitivity complaint, and the candidate unnecessarily over-escalates. The single rule is: sequence care by urgency and risk, not by the loudest preference in the room.
Routine/elective complaints include esthetics, maintenance, replacement of worn restorations without symptoms, denture fit issues without ulceration or inability to function, and stable chronic concerns. Urgent complaints include uncontrolled pain, acute fracture with sharp edges or exposed tissue, new swelling, posttreatment complications, trauma, and bleeding. Mixed visits are especially testable. If the patient says, “I came for cleaning but also this lower tooth kept me up last night,” you must pivot from preventive sequencing to acute problem-focused evaluation.
This is also where communication matters. You can acknowledge the original appointment reason while safely reframing the visit: “We can address your cleaning plan after we evaluate the pain that kept you awake.” That response is patient-centered and clinically defensible.
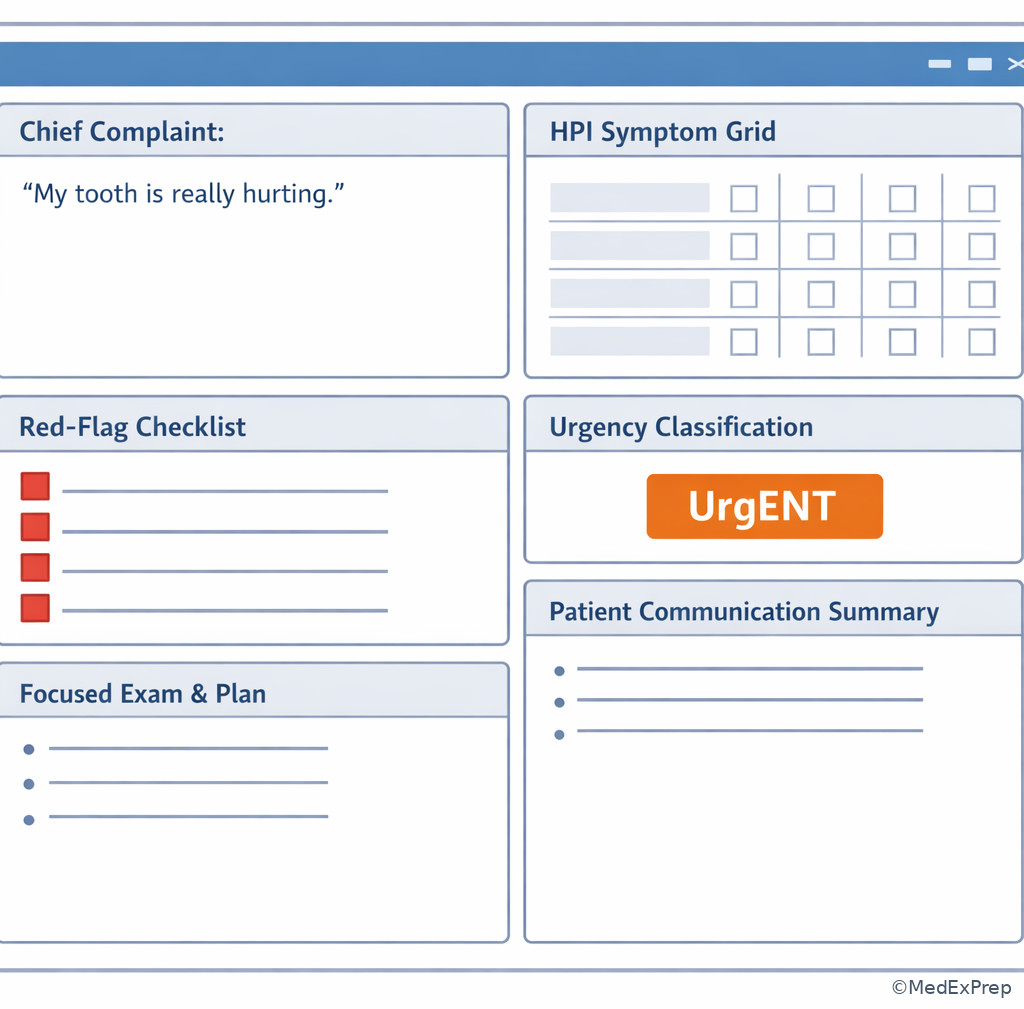
WHY THIS IS TESTED: The exam often embeds the true urgent issue inside a routine visit reason. See Fig 4.
High-Yield Connection: This concept overlaps with Risk-Based Case Prioritization and Phases Of Care. Exam stems frequently pair a chief complaint with treatment sequencing, so know which problem must be addressed first.
Exam takeaway: When routine and acute concerns compete, treat the complaint that changes safety or function first.
B Worked example
A 26-year-old graduate student presents for “a routine cleaning before my wedding.” She has mild anxiety and iron-deficiency anemia. During intake, she adds that a top front tooth chipped yesterday and now catches on her lip; she also had brief bleeding from the area but no loss of consciousness or facial swelling. She is mainly worried about appearance. The distracting clue is the wedding timeline, which can push the candidate toward cosmetic thinking first.
Reasoning chain: Identify task: re-rank today’s priorities. Extract key facts: recent anterior fracture, soft tissue irritation, minor bleeding, no airway or major trauma red flags, routine cleaning was original purpose. Apply rule: acute structural problem affecting comfort and tissue takes priority over elective prophylaxis. Eliminate distractors: proceeding directly with full routine cleaning ignores the more urgent symptomatic problem; emergency hospital referral is excessive; promising definitive esthetic treatment without evaluation is premature. Verify best answer: focused assessment of the fractured tooth and soft tissue risk first, then determine whether limited smoothing, temporization, or referral is appropriate before elective care.
C Exam trap
Common wrong answer: Keeping the appointment on the original elective track because that was the scheduled reason for visit.
Why it is tempting: Candidates confuse schedule type with clinical priority.
Single clue that eliminates it: A new acute complaint disclosed during intake changes the task and must be triaged first.
D Checkpoint
Question: A patient presents for denture adjustment but reports that a lower molar began causing spontaneous pain overnight and now hurts when biting. Which is the most appropriate next step?
- Proceed with the denture adjustment only because that was the scheduled procedure — tempting because it respects the appointment type, but wrong because acute pain changes priority.
- Shift to focused evaluation of the painful tooth before elective denture care — tempting and correct because symptom-driven reprioritization is the safe sequence.
- Dismiss the tooth complaint as stress-related until the denture issue is handled — tempting if the patient has multiple concerns, but wrong because spontaneous overnight pain is clinically meaningful.
- Send the patient to the emergency department solely for biting pain — tempting if all acute pain is overtriaged, but wrong because no emergency red flags are described.
Practitioner Action: Assess whether any new complaint changes urgency during intake, even on a routine visit. Intervene by reprioritizing the appointment toward the higher-risk problem. Refer if the newly disclosed issue exceeds office scope or requires specialist/emergency care. Document the original visit reason, the newly revealed complaint, and why the sequence changed.
- True or False: The scheduled procedure always remains the highest priority. False.
- The best reason to defer elective care is a complaint that changes risk, function, or urgency.
- Name one routine complaint and one urgent complaint: whitening request; progressive swelling.
Exam takeaway: Red flags and function loss determine whether to reassure, evaluate urgently, or escalate immediately.
flowchart TD
A[Chief complaint] --> B{Airway, dysphagia, rapidly spreading swelling, uncontrolled bleeding, major trauma?}
B -->|Yes| C[Immediate escalation / emergency referral]
B -->|No| D{Severe pain, new swelling, fracture, post-op complication, sleep/eating impact?}
D -->|Yes| E[Same-day urgent dental evaluation]
D -->|No| F{Routine maintenance or elective concern?}
F -->|Yes| G[Routine assessment and scheduling]
F -->|No| H[Focused history and exam to reclassify urgency] Exam takeaway: Visible spread, swallowing difficulty, and restricted opening are complaint-level clues that upgrade urgency before definitive treatment.
1.1.1.7 Convert the complaint into a defensible next step and chart note
A Explanation
The last foundational integration task is what do you do after you understand the complaint? The wrong move is to stop at pattern recognition. The correct move is to convert the complaint into a best-next-step statement that is safe, scope-aware, and documentable. The governing rule is: every complaint analysis should end with a triage category, focused plan, and chart-ready summary.
A good chart note links the patient’s words to your clinical interpretation without overstating certainty. Example: “CC: ‘Lower left tooth hurts when I bite.’ HPI: 4 days, localized, worse with chewing, no swelling, no fever, no dysphagia, no spontaneous night pain. Plan: focused exam and diagnostic testing of lower left posterior region today.” This is better than “cracked tooth” before confirmation or “needs extraction” before diagnosis. Your next-step statement should also reflect scope. If the complaint suggests an emergency or specialist threshold, document referral and patient instructions clearly rather than implying definitive specialist treatment will occur in your chair.
Patient communication matters here too. You should explain what you are doing and why: “Based on what you’ve told me, the safest next step is to examine the painful area first and then decide whether this is something we treat today, monitor, or refer.” This is the kind of language that sounds competent in an OSCE.
WHY THIS IS TESTED: Boards assess not just recognition, but action selection and defensible documentation. See Fig 4 and Fig 5.
Recall: In the upcoming topic Medical History Risk Flags, you will add systemic modifiers to this next-step decision. A complaint that seems routine can become delayed or modified once uncontrolled medical disease is identified.
Exam takeaway: Finish every chief complaint interview with a triage label, immediate action, and chartable summary.
B Worked example
A 61-year-old man presents saying, “I just want my partial adjusted.” He has osteoarthritis and controlled hyperlipidemia. During intake he reveals that a lower left tooth has had dull pain for 2 weeks, now worse on chewing, with one episode of waking at night; he denies swelling, fever, or difficulty swallowing. He also says he has an old bridge “on that side somewhere,” a tempting clue that may cause anchoring on prosthetic irritation rather than targeted pain evaluation.
Reasoning chain: Identify task: determine best immediate focus and document it. Extract key facts: partial adjustment request, but active posterior tooth pain with chewing and night awakening; no emergency red flags. Apply rule: complaint analysis ends in triage and next step. Eliminate distractors: routine prosthesis adjustment alone ignores the higher-priority pain; emergency referral is unsupported; definitive specialty treatment cannot be chosen before exam. Verify best answer: document the revised chief complaint and perform focused diagnostic assessment of the painful posterior region first, then address the partial if time and safety permit.
A defensible chart line would state both issues but clearly prioritize the painful tooth complaint.
C Exam trap
Common wrong answer: Writing a vague note such as “patient in pain” and proceeding without a structured plan.
Why it is tempting: Under time pressure, vague documentation feels faster.
Single clue that eliminates it: OSCE scoring rewards explicit reasoning: complaint, symptom pattern, urgency level, and next step must all be visible.
D Checkpoint
Question: Which charting statement best reflects defensible chief complaint analysis?
- “Needs root canal.” — tempting because it sounds decisive, but wrong because it overstates a diagnosis before evaluation.
- “Patient reports ‘sharp pain on lower right when chewing for 3 days’; no swelling, fever, or dysphagia; focused exam planned today.” — tempting and correct because it preserves the patient’s report, records key negatives, and states the next step without overcommitting.
- “Pain probably from stress.” — tempting when the history seems vague, but wrong because it is unsupported and prematurely dismissive.
- “Will extract if confirmed.” — tempting because it sounds conditional, but wrong because it still jumps ahead to a procedural solution rather than documenting the current assessment task.
Practitioner Action: Assess the complaint until you can state the problem in clinical terms. Intervene by selecting the safest next step within entry-level scope. Refer when the next step is beyond routine ambulatory general dentistry or emergency thresholds are met. Document verbatim complaint, targeted HPI details, red-flag negatives/positives, urgency level, plan, and patient instructions.
Exam takeaway: The strongest notes connect the patient’s words to urgency level and a specific next action without overstating diagnosis.
flowchart LR A[Patient words] --> B[Focused HPI details] B --> C[Red flag screen] C --> D[Urgency label] D --> E[Best next step] E --> F[Chart note + patient explanation]
Exam takeaway: A chart note should show patient words, symptom discriminators, urgency findings, and the immediate plan in a clear sequence.
Exam takeaway: Visual sequencing helps distinguish when acute symptoms should displace planned elective care.
Exam takeaway: A short, structured question set captures the symptom details that most often separate similar answer choices.
Tables
| Complaint detail | Why it matters | What it changes |
|---|---|---|
| Patient’s exact words | Preserves the presenting concern without clinician bias | Improves chart defensibility and communication |
| Onset and time course | Separates sudden acute problems from chronic stable concerns | Urgency and likely pathophysiologic lane |
| Trigger | Cold, heat, chewing, sweets, or spontaneous onset narrow possibilities | Choice of focused tests and differential |
| Lingering after stimulus | Distinguishes milder superficial sensitivity patterns from more concerning pulpal patterns | Urgency of workup |
| Localization | Well-localized versus diffuse symptoms affect source confidence | Need for broader differential and targeted exam |
| Swelling/fever/trismus/dysphagia | Complaint-level red flags | Urgent escalation threshold |
| Effect on eating or sleep | Signals symptom severity and function loss | Same-day prioritization |
| Recent trauma or dental treatment | Changes likely source and possible complications | Focused trauma/post-op pathway |
| Pattern | Choose this framing | Reject this shortcut | Best next step |
|---|---|---|---|
| Patient requests extraction or crown | Requested procedure is not the diagnosis | Immediate procedural commitment | Clarify complaint and examine first |
| Brief cold sensitivity | Trigger-duration pattern matters | Assuming severe infection from any thermal pain | Focused routine evaluation |
| Spontaneous night pain with lingering thermal pain | More concerning pain behavior | Treating as simple sensitivity | Prioritize pulpal/periapical workup |
| Rapid swelling with dysphagia | Safety outranks procedure | Routine office-only management | Immediate escalation/emergency referral |
| Routine recall plus new acute pain | Reprioritize by urgency | Staying on elective schedule only | Focused acute evaluation first |
| Vague complaint without clear source | Neutral documentation and targeted history | Overstated diagnosis in the chart | Structured HPI and exam plan |
| Complaint category | Typical clues | Common wrong answer | Discriminator |
|---|---|---|---|
| Routine/elective | Cleaning, whitening, stable prosthesis adjustment, asymptomatic replacement | Over-escalating every concern | No urgent function loss or red flags |
| Urgent dental | Acute pain, fracture discomfort, new localized swelling, chewing pain, post-op concern | Keeping the visit purely elective | Symptoms affect comfort/function and need prompt evaluation |
| Emergency escalation | Dysphagia, airway compromise, rapidly spreading swelling, uncontrolled bleeding, major trauma concerns | Providing routine definitive office care first | Potential systemic or airway threat |
| Nonodontogenic possibility | Poor localization, atypical pattern, mismatch with dental findings | Forcing a tooth-based diagnosis too early | History pattern does not fit common odontogenic triggers |
| Patient-request-driven | “I need a root canal,” “just pull it,” “just give antibiotics” | Accepting the request as treatment plan | No diagnosis has been established yet |
| Charting approach | Strong example | Weak example |
|---|---|---|
| Chief complaint | “Patient states, ‘My lower right tooth hurts when I bite.’” | “Needs dental work.” |
| Symptom details | 3 days, chewing-triggered, no swelling, no fever, sleep intact | “Painful.” |
| Urgency statement | No airway/systemic red flags; urgent focused dental evaluation today | No urgency assessment recorded |
| Plan | Focused exam and diagnostic testing before treatment decision | “Will fix tooth.” |
| Referral note | Dysphagia and diffuse swelling discussed; patient directed for emergency evaluation | “Told patient to go somewhere else.” |
Exam Traps & Differentiators
Common traps & distractors: The most common wrong answer is treating the stated request as the true clinical task. This is tempting because patients often sound certain and the request resembles a treatment plan. The discriminator is whether you have enough complaint analysis to justify action. If not, the next step is clarification and targeted evaluation.
Looks similar but isn’t: Acute sensitivity and urgent pulpal pain can both involve thermal triggers, but the discriminator is whether the pain lingers or occurs spontaneously. Routine recall and urgent same-day care can occur in the same visit, but the discriminator is whether the newly disclosed symptom affects safety, function, or urgency.
| If the stem says... | Think... |
|---|---|
| “I just need this tooth pulled” | Clarify the underlying complaint before accepting the requested procedure |
| “Cold hurts, but it stops right away” | Provoked nonlingering pattern; routine focused evaluation lane |
| “It woke me up and I can’t tell which tooth” | More concerning pulpal pain pattern; urgent diagnostic workup lane |
| “The swelling got much bigger today and it’s hard to swallow” | Emergency escalation threshold |
| “I came for cleaning, but this tooth started throbbing yesterday” | Reprioritize the visit to the acute complaint |
| “Just give me antibiotics” | Do not let the patient select management before triage and diagnosis |
Cross-topic confusable pairs: In the upcoming Medical History Risk Flags lesson, some patients with routine-looking complaints will need care modification or deferral because of uncontrolled systemic disease. In Medication And Allergy Review, a patient’s complaint may reflect medication effect, adverse reaction, or mistaken allergy labeling. Here, your job is not to solve those topics yet, but to leave room for them by not anchoring too early.
Algorithm / Approach
Exam takeaway: A repeatable triage sequence helps you choose the safest defensible next step under OSCE time pressure.
Rapid Review
- Requested procedure → not the same as diagnosis
- Patient quote in chart → stronger than clinician paraphrase alone
- Provoked brief cold pain → lower urgency than spontaneous lingering pain
- Night-waking pain → raises concern beyond simple sensitivity
- Biting pain → think crack/occlusion/apical-periodontal lane before cosmetic explanations
- Dysphagia with swelling → escalation problem, not routine office care
- Diffuse swelling → more concerning than localized gingival tenderness
- Routine visit plus new acute symptom → reprioritize the visit
- Open-ended first question → reduces anchoring and improves accuracy
- Function loss → urgency clue even before definitive diagnosis
- “Just antibiotics” request → patient preference, not management authority
- Defensible note → patient words + HPI pattern + urgency + next step
- Emergency referral answer → justified by airway/systemic compromise, not pain alone
- Best next step → often focused evaluation, not definitive treatment
Memory anchor: For OSCE pacing, use QUOTE → SORT → SCREEN → STEP: quote the patient, sort the symptom pattern, screen red flags, choose the next step.
Self-check quiz
1. A 31-year-old patient says, “I need a crown on this tooth today.” She has mild eczema and seasonal allergies. She adds that the tooth has been sensitive to cold for 1 week, but the pain stops immediately after the drink is removed. Which is the most appropriate next step?
- A. Schedule crown preparation immediately
- B. Obtain focused history and examine the tooth before selecting treatment
- C. Prescribe antibiotics for likely infection
- D. Refer to the emergency department
2. A 24-year-old patient presents for whitening consultation. He has mild asthma and no recent dental care. During intake he reports lower molar pain that began with cold drinks and now wakes him at night. Which complaint feature most strongly changes this from a routine esthetic visit to an urgent diagnostic visit?
- A. Interest in whitening
- B. History of mild asthma
- C. Night-waking pain
- D. Lack of recent dental care
3. A 47-year-old woman presents saying, “I think food is stuck back there.” She has controlled hypertension and osteoarthritis. She reports localized gingival soreness after popcorn last night, no swelling, no fever, no dysphagia, and she can point to the site exactly. Which is the most appropriate complaint classification?
- A. Emergency escalation for spreading infection
- B. Urgent same-day localized dental evaluation
- C. Purely elective cosmetic concern
- D. Immediate hospital management for airway risk
4. A 39-year-old man presents for a denture adjustment. He has GERD and hyperlipidemia. During intake he reports a lower right tooth with sharp pain on chewing for 4 days and one episode of spontaneous pain overnight; no swelling, fever, or trauma. What is the most appropriate next step?
- A. Proceed with the denture adjustment only because that was scheduled
- B. Shift to focused evaluation of the painful tooth before elective denture care
- C. Send him for emergency hospital evaluation because pain was spontaneous once
- D. Promise extraction today if the patient wants it
5. A 58-year-old patient says, “Just give me antibiotics.” He has type 2 diabetes and reports facial swelling since yesterday, feverish feeling, and increasing difficulty opening. He denies chest pain. Which single complaint clue most requires escalation of urgency?
- A. Request for antibiotics
- B. Facial swelling with increasing difficulty opening
- C. Type 2 diabetes alone
- D. Absence of chest pain
6. A 44-year-old woman presents saying, “My upper left tooth is cracked, so I want it out.” She has anxiety and hypothyroidism. She reports pain only on biting hard foods for 2 weeks, no swelling, no fever, no spontaneous pain, and no sleep interruption. Which is the most defensible immediate response?
- A. Agree to extraction because the patient has identified the cause
- B. Explain that the complaint needs focused evaluation before any treatment decision
- C. Prescribe antibiotics because chewing pain suggests apical infection
- D. Refer to the emergency department for all cracked-tooth complaints
7. A 63-year-old man presents for routine prophylaxis. He has controlled atrial fibrillation and chronic kidney disease stage 3. On questioning, he reports that a lower posterior tooth developed spontaneous throbbing pain last night and now feels “high” when he bites; he also notes mild localized swelling near the tooth but no dysphagia, no breathing difficulty, and no diffuse facial swelling. Which is the most appropriate next step?
- A. Continue with prophylaxis because the scheduled visit is routine
- B. Reclassify the visit as urgent same-day dental evaluation of the painful tooth
- C. Send him directly to emergency services because any swelling requires hospital care
- D. Chart “likely abscess, extraction needed” before examination
8. A 36-year-old patient says, “I chipped a front tooth, but I mostly just want my cleaning.” She has iron-deficiency anemia and controlled asthma. The chip occurred today, the edge is sharp and catching her lip, there is no loss of consciousness, no malocclusion, and no facial swelling. Which is the most appropriate sequencing decision?
- A. Perform the full cleaning first, then discuss the chip if time remains
- B. Focus first on evaluation and limited management of the acute chipped tooth issue
- C. Refer immediately to emergency services because all dental trauma is emergent
- D. Ignore the chip because the patient says the cleaning matters more
Answer key
1.1.1.8 1. Answer: B
A. Schedule crown preparation immediately — Tempting because the patient requests a crown and there is localized sensitivity. Incorrect for this scenario because a requested procedure is not yet the indicated treatment; the single discriminating clue is that no focused evaluation has been completed. Authoritative dental diagnostic standards require assessment before definitive treatment selection. Sources: ADA oral health topics; Stefanac and Nesbit.
B. Obtain focused history and examine the tooth before selecting treatment — Tempting because it may feel less decisive, but it is correct. The brief cold sensitivity pattern and patient-request framing both support diagnostic clarification first; the discriminating clue is symptom analysis before procedure choice. Sources: Stefanac and Nesbit; CDT principles of diagnosis and treatment planning.
C. Prescribe antibiotics for likely infection — Tempting because pain can make infection seem likely. Incorrect because isolated brief cold sensitivity without swelling or systemic signs does not justify empiric antibiotic management; the discriminating clue is the absence of infection red flags. Sources: ADA guideline principles on antibiotic stewardship in dental pain/swelling contexts.
D. Refer to the emergency department — Tempting if any dental pain is overtriaged. Incorrect because there are no airway, systemic, or major trauma findings; the discriminating clue is a stable symptom pattern without red flags. Sources: ADA and standard urgent care triage principles.
1.1.1.9 2. Answer: C
A. Interest in whitening — Tempting because it explains why the patient came in. Incorrect because appointment reason does not determine urgency; the discriminating clue is that a new pain history supersedes the elective request. Sources: Stefanac and Nesbit.
B. History of mild asthma — Tempting because medical history matters in later sequencing. Incorrect here because asthma does not itself explain the urgency shift; the discriminating clue is symptom behavior, not the comorbidity. Sources: entry-level dental assessment standards.
C. Night-waking pain — Correct because it is a high-yield symptom discriminator suggesting a more urgent pain pattern than routine sensitivity alone. The single clue is pain that wakes the patient from sleep, which changes priority. Sources: pulpal pain history principles in standard endodontic diagnosis texts and dental diagnosis references.
D. Lack of recent dental care — Tempting because overdue care can increase disease burden. Incorrect because it does not by itself establish urgency; the discriminating clue remains the night pain. Sources: standard dental diagnostic reasoning texts.
1.1.1.10 3. Answer: B
A. Emergency escalation for spreading infection — Tempting because the problem is acute and oral soreness can be mistaken for infection. Incorrect because the symptoms are localized and lack systemic or airway red flags; the discriminating clue is exact localization without fever, dysphagia, or diffuse swelling. Sources: ADA urgent care principles; dental diagnosis texts.
B. Urgent same-day localized dental evaluation — Correct because a new symptomatic localized problem merits focused prompt evaluation, even if it is not an emergency. The single clue is acute localized soreness after food impaction with no emergency features. Sources: Stefanac and Nesbit.
C. Purely elective cosmetic concern — Tempting if the soreness seems minor. Incorrect because the patient has an active symptom requiring assessment; the discriminating clue is that this is a current painful complaint, not a preference-based visit. Sources: treatment planning fundamentals.
D. Immediate hospital management for airway risk — Tempting if candidates overreact to any oral pain. Incorrect because airway risk signs are absent; the discriminating clue is no swelling, fever, or dysphagia. Sources: standard dental emergency triage guidance.
1.1.1.11 4. Answer: B
A. Proceed with the denture adjustment only because that was scheduled — Tempting because it respects the appointment plan. Incorrect because the new complaint changes clinical priority; the discriminating clue is chewing pain plus spontaneous overnight pain. Sources: treatment sequencing principles in dental care planning.
B. Shift to focused evaluation of the painful tooth before elective denture care — Correct because symptoms suggesting acute tooth pathology should be addressed before elective prosthetic adjustments. The single clue is that an acute painful complaint was disclosed during intake. Sources: CDT and entry-level treatment planning standards.
C. Send him for emergency hospital evaluation because pain was spontaneous once — Tempting because spontaneous pain feels serious. Incorrect because emergency escalation requires more than a single spontaneous episode without airway/systemic compromise; the discriminating clue is absence of swelling, fever, or dysphagia. Sources: ADA urgent care triage principles.
D. Promise extraction today if the patient wants it — Tempting as a decisive pain solution. Incorrect because procedure choice follows diagnosis, not the patient’s anticipated preference; the discriminating clue is no diagnostic confirmation. Sources: Stefanac and Nesbit.
1.1.1.12 5. Answer: B
A. Request for antibiotics — Tempting because it sounds like the patient believes infection is present. Incorrect because patient preference does not determine urgency; the discriminating clue is objective complaint severity, not the requested therapy. Sources: ADA antibiotic stewardship principles.
B. Facial swelling with increasing difficulty opening — Correct because progressive swelling with trismus is a red-flag pattern that can indicate spreading infection requiring escalation. The single clue is increasing difficulty opening. Sources: ADA emergency/urgent care principles; standard oral infection triage guidance.
C. Type 2 diabetes alone — Tempting because diabetes can worsen infection risk. Incorrect because diabetes is an important modifier but not the single complaint feature that most directly determines immediate escalation here; the discriminating clue remains progressive swelling/trismus. Sources: dental management of medically complex patients texts.
D. Absence of chest pain — Tempting because chest pain is a major medical symptom generally. Incorrect because it does not help classify odontogenic urgency here; the discriminating clue is infection-related functional change, not absence of unrelated symptoms. Sources: general dental urgent triage standards.
1.1.1.13 6. Answer: B
A. Agree to extraction because the patient has identified the cause — Tempting because the history of biting pain on hard foods can suggest crack-related disease. Incorrect because even a plausible self-diagnosis still requires evaluation before treatment commitment; the discriminating clue is that the patient request is not yet a confirmed management decision. Sources: Stefanac and Nesbit; treatment planning standards.
B. Explain that the complaint needs focused evaluation before any treatment decision — Correct because the symptom pattern suggests a diagnostic lane, not a definitive procedure. The single clue is pain only on biting hard foods without infection red flags, which supports targeted assessment first. Sources: standard dental diagnosis and treatment planning references.
C. Prescribe antibiotics because chewing pain suggests apical infection — Tempting because chewing pain can occur with apical involvement. Incorrect because there is no swelling, fever, or systemic evidence supporting empiric antibiotic use; the discriminating clue is isolated biting pain without red-flag infectious signs. Sources: ADA antibiotic guidance.
D. Refer to the emergency department for all cracked-tooth complaints — Tempting if trauma or fracture is generalized into emergency care. Incorrect because this stable complaint lacks emergency features; the discriminating clue is no swelling, fever, or sleep disruption. Sources: standard dental urgent care principles.
1.1.1.14 7. Answer: B
A. Continue with prophylaxis because the scheduled visit is routine — Tempting because the patient came for maintenance and appears medically stable overall. Incorrect because the new complaint includes spontaneous throbbing pain, biting change, and localized swelling, which require reprioritization; the discriminating clue is active acute symptom burden. Sources: treatment sequencing standards.
B. Reclassify the visit as urgent same-day dental evaluation of the painful tooth — Correct because there is an acute dental complaint without current emergency airway features. The single clue is localized swelling with spontaneous pain but no dysphagia or diffuse facial spread, placing this in urgent same-day rather than emergency escalation. Sources: ADA urgent dental care principles; Stefanac and Nesbit.
C. Send him directly to emergency services because any swelling requires hospital care — Tempting because swelling raises concern. Incorrect because not all swelling is emergent; the discriminating clue is the absence of airway compromise, dysphagia, or diffuse rapidly spreading swelling. Sources: dental emergency triage guidance.
D. Chart “likely abscess, extraction needed” before examination — Tempting because the symptom cluster may suggest infection. Incorrect because documentation should record the complaint and plan without overstating diagnosis or treatment; the discriminating clue is that examination is still pending. Sources: objective charting and diagnosis principles.
1.1.1.15 8. Answer: B
A. Perform the full cleaning first, then discuss the chip if time remains — Tempting because the patient says the cleaning is the main goal. Incorrect because an acute fractured edge injuring soft tissue changes priority; the discriminating clue is same-day sharp edge catching the lip. Sources: dental trauma and sequencing fundamentals.
B. Focus first on evaluation and limited management of the acute chipped tooth issue — Correct because the complaint has become an acute symptomatic problem even without major trauma red flags. The single clue is soft tissue-catching sharpness from today’s fracture, which should be addressed before elective prophylaxis. Sources: standard entry-level dental trauma assessment and treatment planning principles.
C. Refer immediately to emergency services because all dental trauma is emergent — Tempting because trauma language sounds serious. Incorrect because there is no loss of consciousness, malocclusion, facial swelling, or other emergency-level red flag; the discriminating clue is isolated uncomplicated acute tooth injury. Sources: dental trauma triage standards.
D. Ignore the chip because the patient says the cleaning matters more — Tempting as a patient-autonomy misinterpretation. Incorrect because patient preference does not override safe sequencing when an acute symptomatic issue is present; the discriminating clue is active soft tissue irritation. Sources: patient-centered care and clinical prioritization standards.