Why it matters
- Many missed COMLEX questions are not knowledge failures; they are task-recognition failures where the learner answers a different question than the one asked.
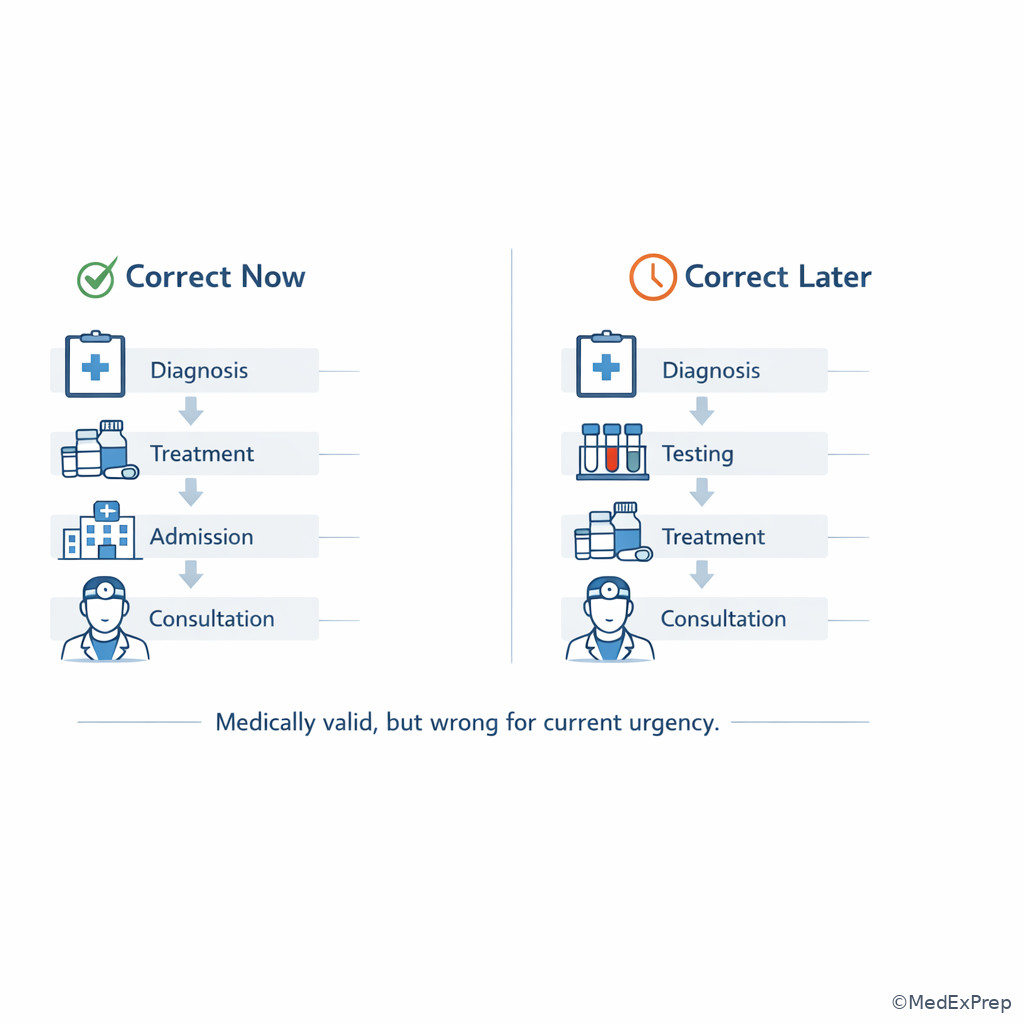
- Board stems often contain enough information to support several reasonable actions; the correct option is the one that matches the task now, not the one that is true in general.
- Safety-sensitive items reward sequencing: stabilize first, then diagnose, then confirm, then treat definitively.
- Osteopathic reasoning is testable, but it is never a reason to ignore instability, contraindications, or a time-sensitive emergency.
Key Terms & Must-Know Facts
1.1.1.1 Key terms
- Clinical task — the action the question is truly asking you to perform
- Most likely diagnosis — identify the condition that best fits the data already provided
- Best initial test — first study that safely narrows management
- Confirmatory test — study that establishes the diagnosis after suspicion exists
- Most appropriate next step — the immediate action that improves safety or advances care now
- First-line treatment — standard initial therapy for the patient in front of you
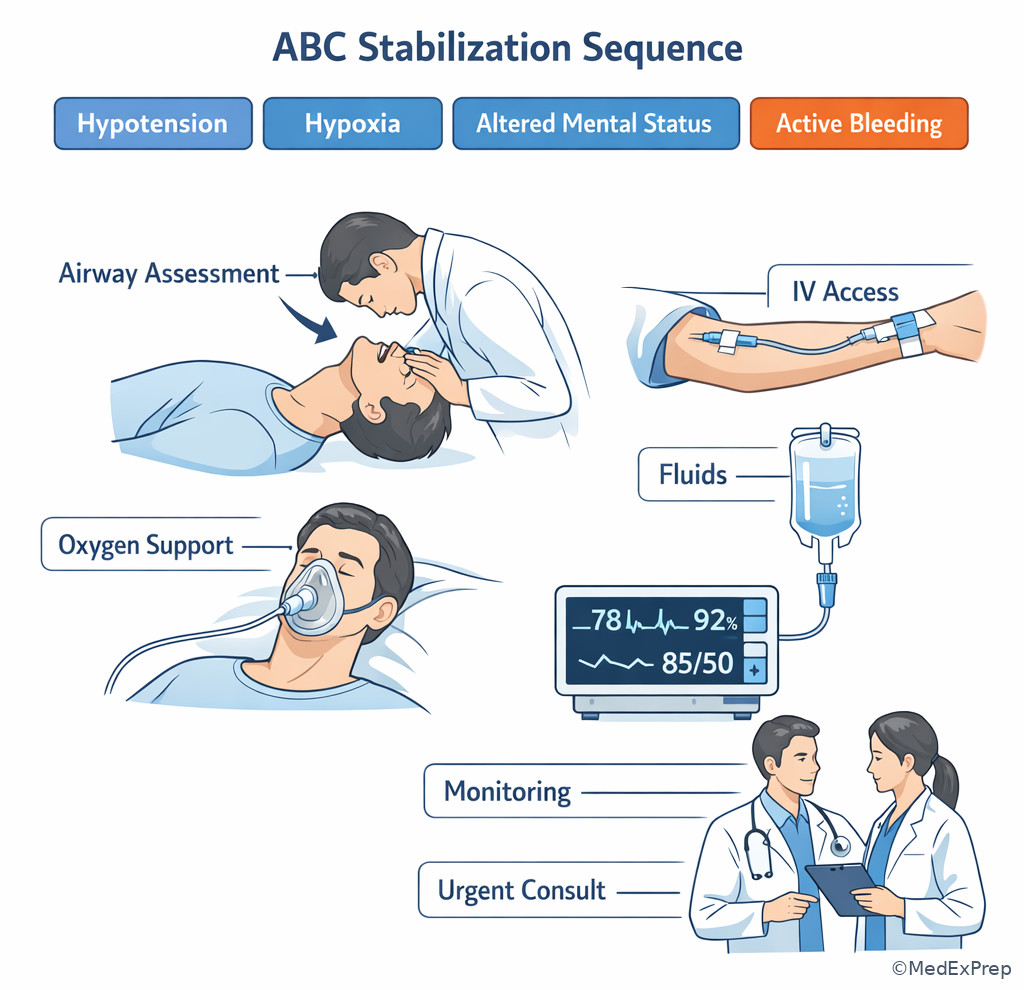
- Immediate stabilization — ABCs, hemorrhage control, reversal of life threats before complete workup
- Disposition — admit, observe, discharge, ICU transfer, urgent consult
- Contraindication — a feature that makes an otherwise reasonable option unsafe
- Distractor — an answer choice that would be correct in a different but similar scenario
- Noise — extra stem detail that is real but not task-determining
- Rule-out emergency — condition that must be excluded first because delay harms the patient
- Board wording trigger — phrase such as “best next step,” “requires immediate clarification,” or “most important to monitor”
1.1.1.2 Must-know facts
- The question stem often tests recognition of the task more than recall of a disease fact.
- “Best next step” is not the same as “most accurate test.”
- An unstable patient changes the task from diagnosis to stabilization.
- If the diagnosis is already obvious, the task may be treatment or disposition rather than more testing.
- If a question asks for “confirmation,” do not choose a screening or initial test.
- If an option is broadly true but mistimed, it is wrong.
- A tempting wrong answer often fits a nearby topic, not the task being tested.
- On COMLEX, OMT may be useful only when it is appropriate, safe, and not delaying urgent care.
Exam takeaway: Match the stem's wording to the exact clinical task before interpreting answer choices.
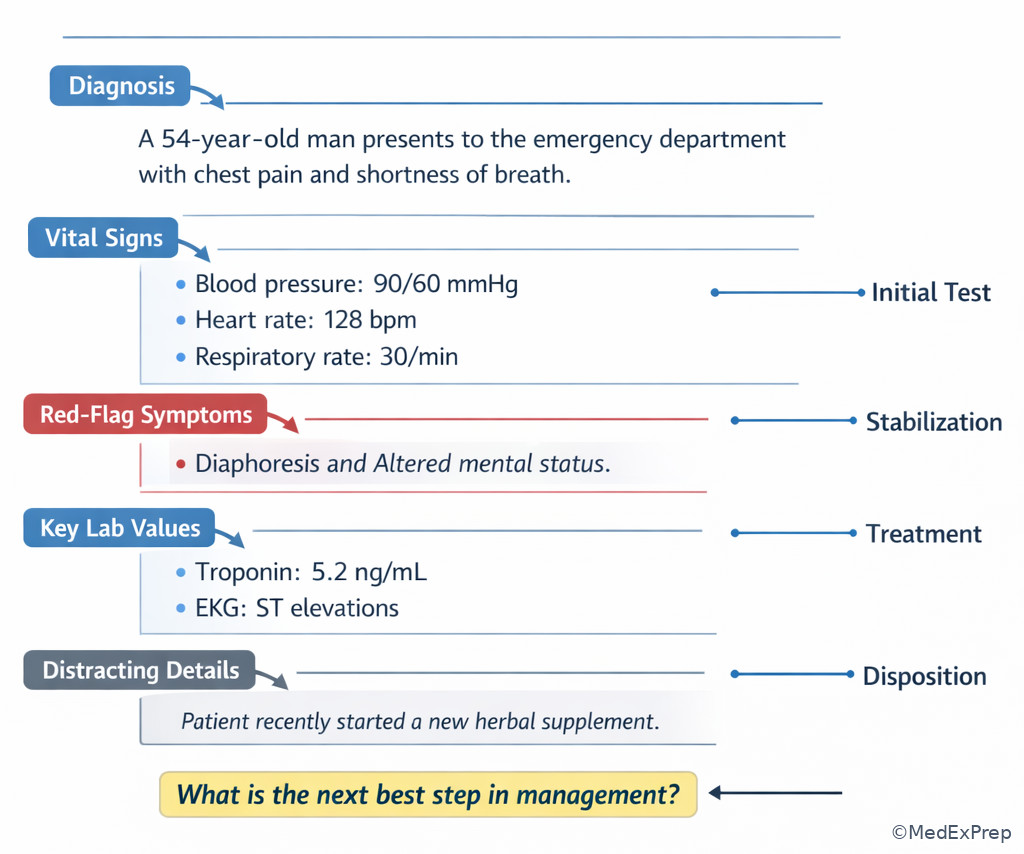
flowchart TD
A[Read final sentence first] --> B{What is being asked?}
B --> C[Diagnosis]
B --> D[Initial test]
B --> E[Immediate stabilization]
B --> F[Treatment]
B --> G[Disposition or follow-up]
C --> H[Use pattern recognition]
D --> I[Choose safest high-yield first study]
E --> J[ABCs and life threats first]
F --> K[Pick first-line for this patient now]
G --> L[Admit, observe, discharge, or escalate] Use this figure as your first pass on any vignette. See Fig 1.
Exam takeaway: Visual cues such as the final sentence and instability markers usually reveal the intended task faster than the diagnosis details.
| Stem wording | Usual task | What to prioritize | Common mistake |
|---|---|---|---|
| Most likely diagnosis | Name the condition | Pattern fit | Choosing a management step |
| Best initial test | First study | Safety and yield | Picking gold-standard confirmation |
| Most appropriate next step | Immediate action | Timing now | Jumping to definitive therapy too soon |
| Best initial therapy | Start treatment | First-line management | Ordering more tests despite enough information |
| Requires immediate clarification | Find the unsafe gap | Patient safety | Focusing on minor inaccuracies |
| Most important to monitor | Follow complication risk | Expected adverse effect | Picking a routine but less critical parameter |
Core content
1.1.1.3 Foundational move: identify the task before solving the case
A Explanation
The first decision conflict is simple but high-yield: Are you being asked to name the problem, test for it, treat it, or stabilize the patient? The single rule that resolves this is to read the final sentence first. If the final sentence says “most likely diagnosis,” stay in diagnostic mode. If it says “best initial therapy,” do not overthink testing unless the stem lacks enough certainty. If it says “most appropriate next step,” the task is usually sequencing rather than fact recall.
WHY THIS IS TESTED: Board writers build stems with enough true details to make multiple options feel medically defensible. The exam rewards the learner who identifies the governing task before engaging disease knowledge. A common choose-vs-reject framework is: choose the option that fits the exact requested action now; reject options that are true but belong to a later stage.
Practical rule: the task lives in the question wording, not in your favorite disease association. If a patient clearly has appendicitis and the question asks for the best next step in an unstable patient, resuscitation may beat CT. If the patient is stable and the diagnosis is obvious from classic signs, treatment may beat more testing.
Exam takeaway: Specific verbs in the question stem map directly to diagnosis, testing, treatment, monitoring, or disposition tasks.
flowchart LR
A[Final sentence] --> B{Trigger word}
B --> C[Most likely diagnosis]
B --> D[Best initial test]
B --> E[Most appropriate next step]
B --> F[Best initial therapy]
B --> G[Most important to monitor]
B --> H[Requires admission or urgent escalation]
C --> C1[Pattern recognition]
D --> D1[First study]
E --> E1[Sequencing]
F --> F1[Treatment choice]
G --> G1[Complication tracking]
H --> H1[Disposition] When the stem feels crowded, reduce it to this map. See Fig 2.
B Worked example
A 67-year-old man presents with 45 minutes of crushing substernal chest pressure. He has diabetes, CKD stage 3, and GERD. He says the pain started after a spicy meal, and he took antacids without relief. Blood pressure is 84/56 mm Hg, pulse 118/min, oxygen saturation 92% on room air. ECG shows ST elevations in II, III, and aVF. The question asks: What is the most appropriate next step in management?
Reasoning chain: Identify task → not diagnosis, because the diagnosis is already essentially given. Extract key facts → hypotension, STEMI pattern, ongoing pain. Apply rule → unstable ischemic patient needs immediate reperfusion-oriented management and stabilization, not confirmatory troponin waiting. Eliminate distractors → GERD is tempting because of meal history, but ECG and shock physiology override. Verify → the best next step is urgent STEMI management, not more diagnostic refinement.
C Exam trap
Common wrong answer: Choose the gold-standard or confirmatory test even when the stem asks for the next action.
Why it is tempting: Students remember that “definitive diagnosis” sounds sophisticated and fear acting before complete certainty.
Single clue that eliminates it: The final sentence asks for the next step, and the patient has instability or enough evidence already to act now.
D Checkpoint
Question: A vignette gives classic nephrolithiasis symptoms and then asks for the best initial pain management. Which answer style is most likely correct?
- CT abdomen/pelvis without contrast — Tempting because it is commonly used to confirm stone location, but wrong if the question asks for initial symptom control rather than diagnosis.
- Urinalysis — Tempting because hematuria supports the diagnosis, but wrong if the task is treatment and the stem already gives enough clues.
- NSAID analgesia — Tempting because it feels “too simple,” but right when the diagnosis is likely and the task is initial therapy.
- Urology referral for lithotripsy — Tempting because it sounds definitive, but wrong without first-line management or an indication for urgent intervention.
Answer: C.
1.1.1.4 Separate decisive clues from noise
A Explanation
The next conflict is which details matter now. In most board stems, only a few findings determine the task: vital signs, time course, a red-flag symptom, a pivotal lab, a contraindication, or the question wording itself. Everything else may be true but non-decisive noise. Students often miss questions because they overweight a memorable clue and underweight the clue that governs urgency or contraindication.
WHY THIS IS TESTED: Real clinical reasoning requires filtering. The exam mirrors this by adding comorbidities, family history, or one distracting lab value. Choose details that change management; reject details that merely decorate the stem. A useful rule is to ask, “If I removed this fact, would my answer change?” If not, it is probably noise.
Decisive clues usually fall into five buckets: instability, localization, timing, exposure, and exclusion. Instability changes everything. Localization narrows a differential. Timing separates acute from chronic and emergent from outpatient. Exposure points toward toxins, infections, or medications. Exclusion clues remove a tempting answer, such as pregnancy, anticoagulation, immunosuppression, or focal neurologic deficits.
Exam takeaway: Vitals, red flags, and contraindications outweigh incidental history when choosing the best answer.
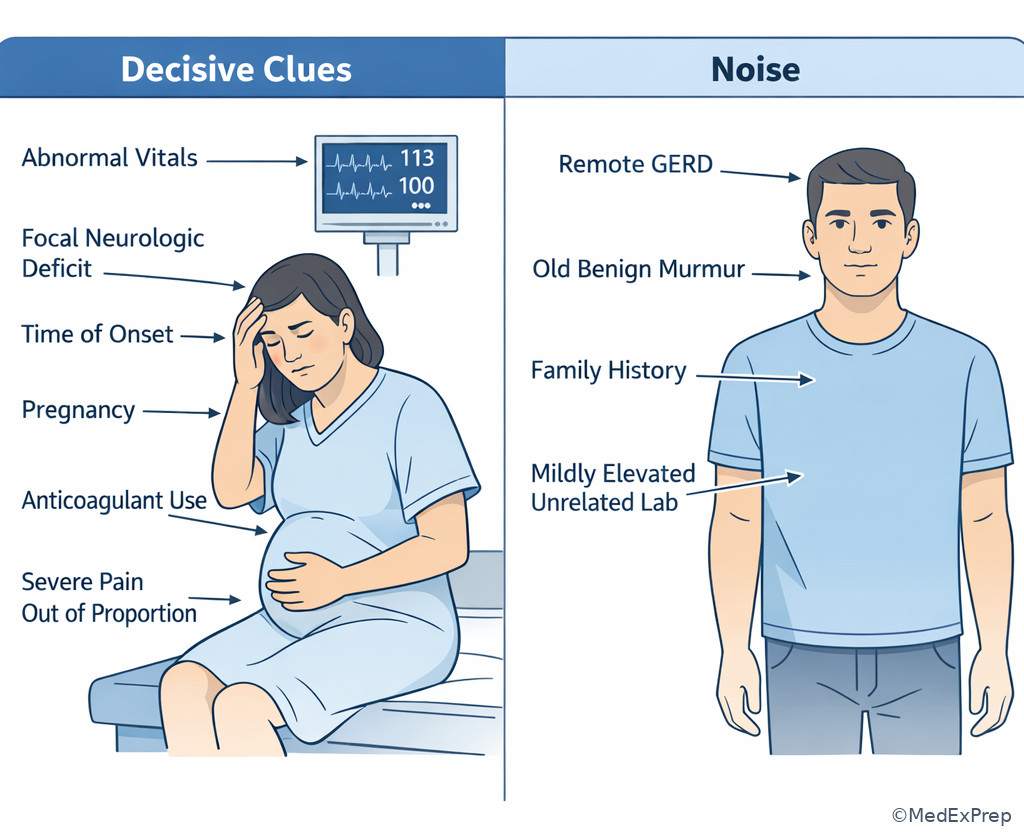
See Fig 3 for a visual way to separate high-value findings from stem clutter.
B Worked example
A 24-year-old woman presents with right lower quadrant pain and nausea. She has IBS and migraines. She returned from a camping trip last week and reports one episode of loose stool yesterday. Temperature is 38.1°C, pulse 104/min. Pregnancy test is positive. WBC count is mildly elevated. The stem asks for the best initial imaging study.
Reasoning chain: Identify task → initial imaging, not diagnosis or treatment. Extract key facts → reproductive-age patient, positive pregnancy test, RLQ pain. Apply rule → avoid default CT when pregnancy changes the safest first imaging choice. Eliminate distractors → recent camping and loose stool tempt you toward infectious GI disease; IBS tempts a benign explanation; neither determines the imaging task. Verify → ultrasound is the best initial imaging approach because pregnancy is the decisive clue.
C Exam trap
Common wrong answer: Anchor on a vivid but low-value detail such as recent travel, chronic GERD, or a mildly abnormal unrelated lab.
Why it is tempting: The detail is memorable and feels “exam-writer intentional.”
Single clue that eliminates it: Ask which fact changes the immediate choice of test or treatment; here, pregnancy changes imaging selection, while the other details do not.
D Checkpoint
Question: Which stem detail is most likely to convert a routine evaluation question into a safety-first question?
- History of seasonal allergies — Tempting because medication allergies can matter, but wrong because seasonal allergies rarely determine emergency sequencing.
- Pain for 3 months with unchanged intensity — Tempting because duration helps chronicity, but wrong because chronic stable symptoms do not usually force immediate stabilization.
- Blood pressure 78/42 mm Hg — Tempting because it is dramatic, and right because hypotension changes the task to urgent assessment and stabilization.
- Remote appendectomy — Tempting because past surgery narrows differential, but wrong because it does not itself create an immediate safety task.
Answer: C.
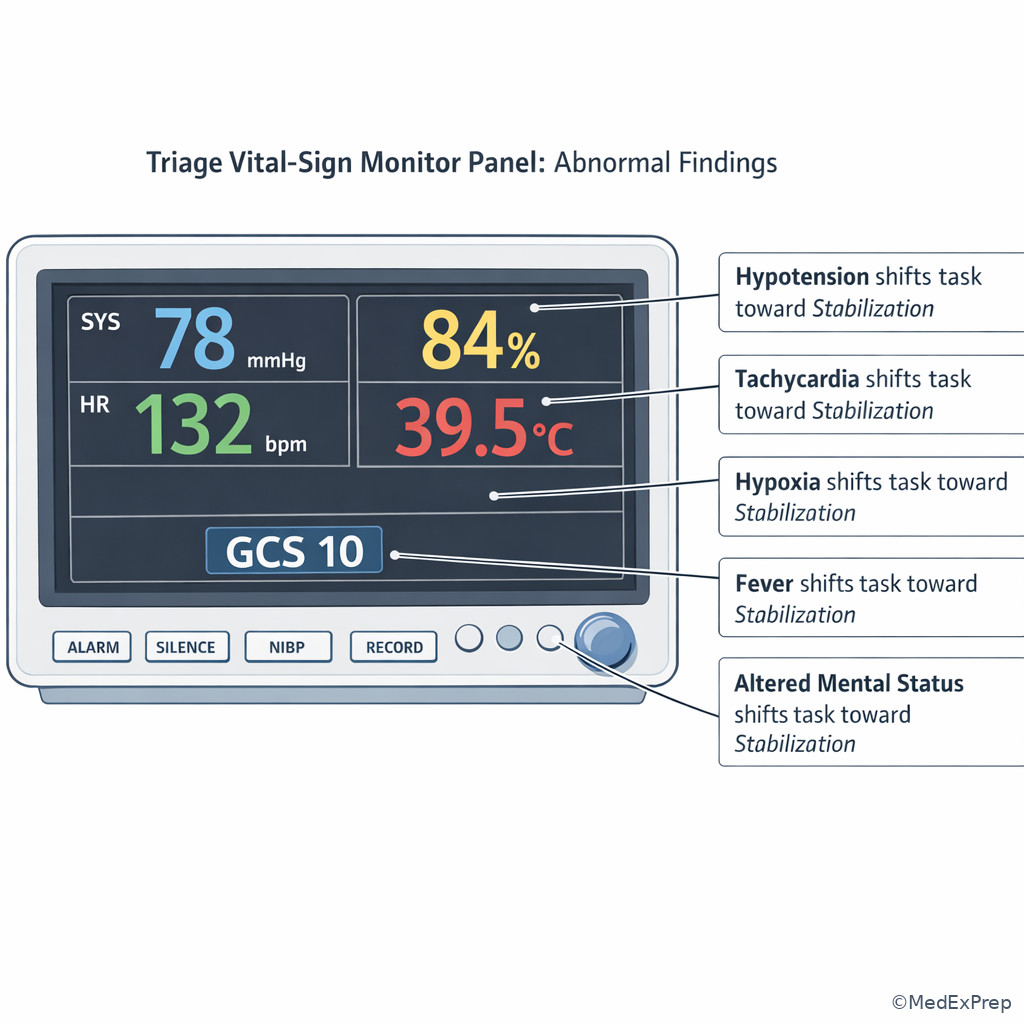
- The most task-changing clue in a vignette is usually abnormal vital signs.
- True or False: The most memorable detail is usually the deciding detail. False.
- Name the 3 highest-yield clue categories: instability, contraindication, timing.
Exam takeaway: Hypotension, hypoxia, fever with toxicity, and altered mental status should immediately move you toward stabilization and escalation.
1.1.1.5 Recognize the common board-style task families
A Explanation
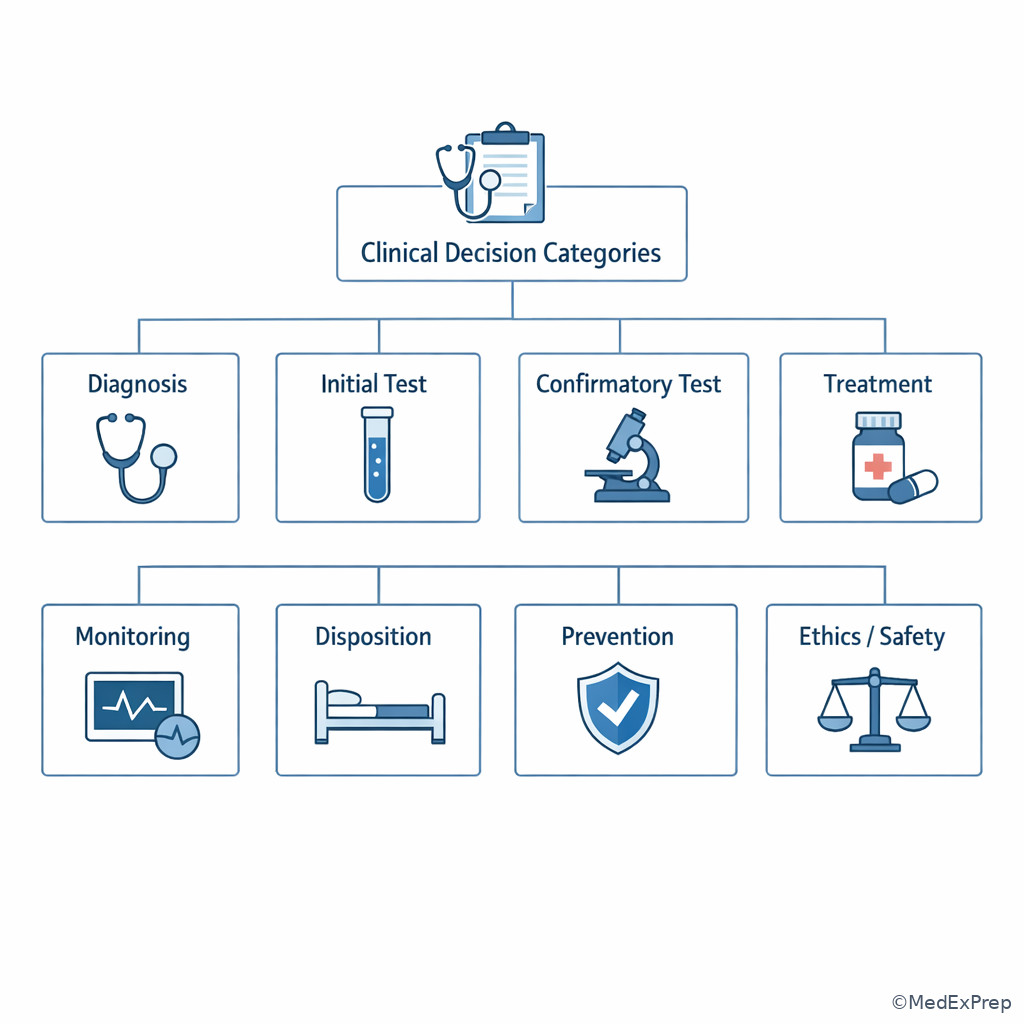
Once you identify that the exam is testing a task, the next conflict is which task family this question belongs to. On COMLEX Level 2-CE, a small set of task families appears repeatedly: diagnosis, best initial test, confirmatory test, best next step, first-line treatment, monitoring, disposition, prevention, ethics/safety clarification, and OMT appropriateness. The single rule is to classify the question before comparing options.
WHY THIS IS TESTED: Different task families use the same disease knowledge differently. For pulmonary embolism, “most likely diagnosis,” “best initial test,” “confirmatory test,” and “most appropriate next step in an unstable patient” can all have different correct answers. The stem tests whether you can shift from one task family to another without being trapped by familiarity.
Choose-vs-reject framing helps: choose diagnostic labels only when the question asks for identification; reject them when the task asks for management. Choose a screening or initial test when the stem asks what to do first; reject the definitive but delayed test if it is mistimed. Choose admission or consultation when the question is really about disposition. Choose counseling or urgent confidentiality action when the stem is about professionalism rather than pathophysiology.
Exam takeaway: Mixed answer categories are a clue that you must classify the question before choosing among options.
flowchart TD
A[Question stem] --> B{Task family}
B --> C[Diagnosis]
B --> D[Testing]
B --> E[Treatment]
B --> F[Monitoring]
B --> G[Disposition]
B --> H[Prevention or counseling]
B --> I[Ethics or safety]
D --> D1[Initial vs confirmatory]
E --> E1[Immediate vs definitive]
G --> G1[Home vs floor vs ICU]
I --> I1[Clarify, report, protect, obtain consent] This classification tool reduces mixed-category confusion. See Fig 4.
B Worked example
A 58-year-old woman with hypertension and obesity has sudden pleuritic chest pain and dyspnea 5 days after knee replacement. She is anxious, mildly tachycardic, and has an oxygen saturation of 91% on room air. The stem asks for the best initial diagnostic test. D-dimer, CT pulmonary angiography, heparin infusion, and lower-extremity duplex ultrasound are listed.
Reasoning chain: Identify task → test selection, not treatment. Extract key facts → postoperative patient, likely PE, stable enough for imaging. Apply rule → because the task family is initial diagnostic testing in a likely PE evaluation, compare only test options first. Eliminate distractors → heparin is management and may be right in another stem, but not in a pure testing question. D-dimer is tempting because it belongs to PE workup, but lower value in a higher-risk postoperative patient. Verify → choose the initial test that best fits suspicion and stability.
C Exam trap
Common wrong answer: Pick a treatment option because the diagnosis seems obvious.
Why it is tempting: Students want to show they know what comes later in management.
Single clue that eliminates it: The stem explicitly asks for a diagnostic test, so mixed-category answers must be filtered by task family first.
D Checkpoint
Question: A stem asks, “Which finding requires immediate clarification before discharge?” What task family is being tested?
- Diagnosis — Tempting because clarification sounds like more data gathering, but wrong because the core issue is safety and disposition.
- Professionalism/patient safety — Tempting because it may feel less “medical,” but right because the task is identifying a barrier or danger before a safe plan.
- First-line treatment — Tempting because clarification may affect therapy, but wrong because treatment is secondary to the immediate unsafe gap.
- Monitoring adverse effects — Tempting because discharge requires follow-up, but wrong because the question is about an unresolved issue before disposition.
Answer: B.
Exam takeaway: Questions become easier when you first sort them into diagnosis, testing, treatment, monitoring, or disposition categories.
1.1.1.6 Applied pattern: when urgency overrides diagnostic completeness
A Explanation
The major application conflict is this: Do you complete the workup, or do you act first because delay is unsafe? The single finding that resolves it is evidence of current or impending instability: airway compromise, respiratory failure, shock, altered mental status, active hemorrhage, evolving ischemia, sepsis with poor perfusion, or another time-sensitive threat. In these scenarios, the task shifts from elegant diagnosis to immediate stabilization or empiric life-saving treatment.
WHY THIS IS TESTED: Board exams heavily reward safe sequencing. The learner must know when diagnostic completeness can wait. This is especially high-yield because many distractors are medically correct but dangerously delayed. Choose-vs-reject framing: choose airway, oxygenation, circulation support, hemorrhage control, antidote, empiric therapy, or emergent consultation when the stem contains instability; reject confirmatory testing that delays rescue.
Do not overextend this rule. Not every abnormal vital sign means bypass all testing. The issue is whether the patient is unstable enough that time-sensitive intervention changes outcome now. That distinction will be expanded in the next lesson, but you must already build the reflex: if the patient is crashing, the question is rarely asking for a leisurely diagnostic refinement.
Exam takeaway: Instability changes many questions from diagnosis or confirmation to immediate stabilization and urgent management.
flowchart TD
A[Identify task] --> B{Any instability or time-sensitive threat?}
B -->|Yes| C[ABCs and immediate rescue]
C --> D[Urgent therapy or consult]
D --> E[Targeted tests after stabilization]
B -->|No| F[Proceed with requested diagnosis/test/treatment task] See Fig 5 whenever you are torn between acting now and completing the workup.
B Worked example
A 72-year-old man presents with fever, productive cough, confusion, and weakness. He has COPD, heart failure, and benign prostatic hyperplasia. Temperature is 39.2°C, blood pressure 82/48 mm Hg, pulse 126/min, respiratory rate 30/min. Lactate is elevated; chest radiograph is pending. The question asks for the most appropriate next step.
Reasoning chain: Identify task → next step. Extract key facts → septic picture with hypotension and confusion. Apply rule → instability overrides the desire for diagnostic completeness. Eliminate distractors → waiting for radiograph confirmation, sputum culture results, or detailed COPD medication history delays urgent treatment. Verify → immediate sepsis-directed resuscitation and empiric antibiotics are the right category of answer now.
C Exam trap
Common wrong answer: Order the perfect confirmatory test before initiating urgent treatment.
Why it is tempting: It feels systematic and academically careful.
Single clue that eliminates it: Hypotension with toxic appearance means the patient cannot wait for diagnostic elegance.
D Checkpoint
Question: Which option best reflects correct board-style sequencing in an unstable patient with suspected ectopic pregnancy?
- Serial outpatient beta-hCG measurements — Tempting because they are used in pregnancy evaluation, but wrong when instability suggests rupture and immediate action is required.
- Expectant management with repeat ultrasound in 48 hours — Tempting because it fits some indeterminate early pregnancies, but wrong in a patient with hemodynamic compromise.
- Immediate stabilization and urgent OB/GYN involvement — Tempting because it is decisive, and right because instability overrides diagnostic completeness.
- Methotrexate after confirmatory imaging — Tempting because it is a recognized treatment for selected stable ectopic pregnancy, but wrong if the patient is unstable.
Answer: C.
- The correct answer in an unstable patient is often the action that improves safety now.
- True or False: The most accurate test is always the best next step. False.
- Name 3 task-switching clues: hypotension, hypoxia, altered mental status.
Exam takeaway: When red flags are present, the exam often tests safe sequencing rather than disease-label recall.
1.1.1.7 Integrate task recognition with osteopathic reasoning and answer elimination
A Explanation
The final integration conflict is how to use all relevant knowledge without overusing any one framework. COMLEX may include structural findings, OMT options, viscerosomatic clues, or patient-centered communication elements. The single rule is that these are helpful only when they match the task and are safe in context. If the patient has a rib dysfunction after pneumonia recovery, OMT may be appropriate. If the patient has acute abdomen, fracture, shock, or neurologic emergency, urgent conventional evaluation and stabilization dominate.
WHY THIS IS TESTED: COMLEX rewards clinically integrated reasoning, not forced OMT or one-note decision making. Choose-vs-reject framing: choose osteopathic assessment or OMT when the stem supports it and no contraindication exists; reject it when used as a substitute for emergency care, definitive testing, or indicated referral. More broadly, when eliminating distractors, ask of each option: Is it the right category? Is it correctly timed? Is it safe? Is there a contraindication? Would it be right for a similar patient but not this one?
This is also where professionalism and safety fit naturally. A question may sound like medicine but really test informed consent, confidentiality, capacity, or escalation. Clinical task recognition keeps you from forcing a pathology answer onto an ethics task.
Exam takeaway: Osteopathic assessment or OMT is appropriate only when it fits the task and does not delay urgent conventional care.
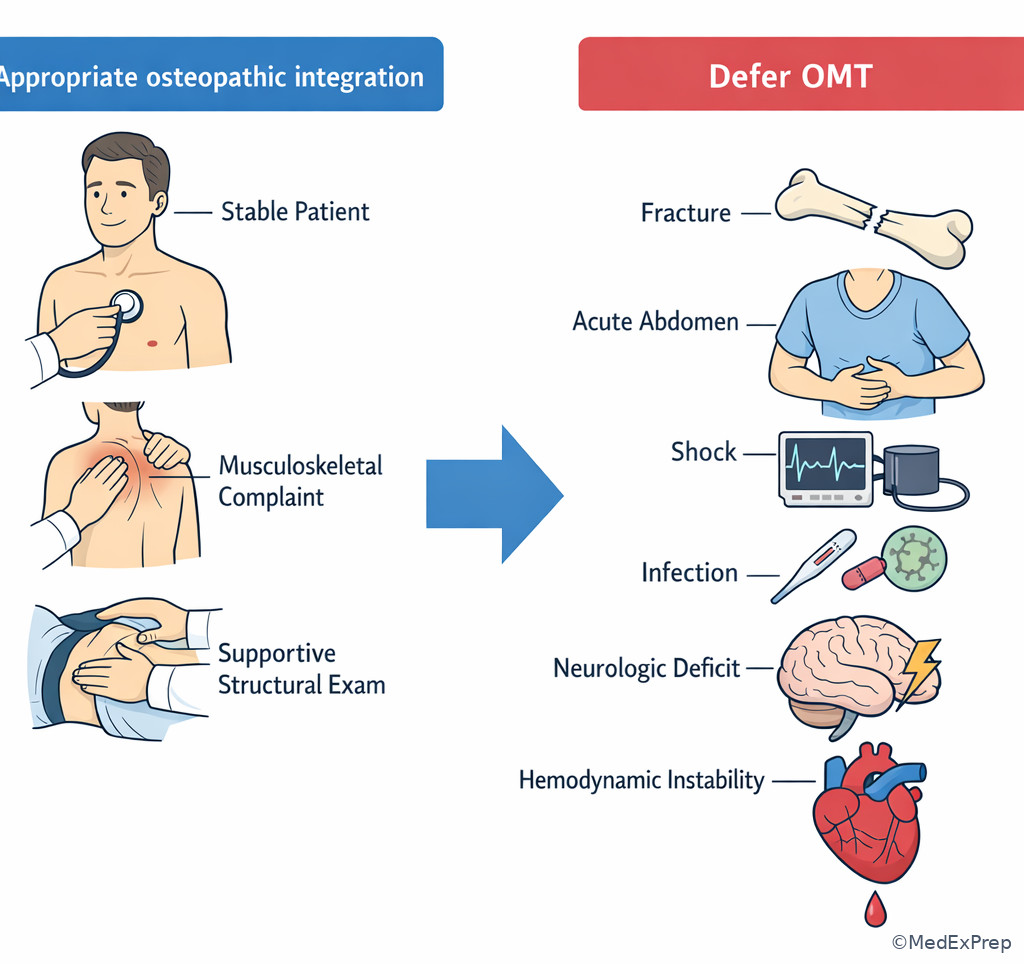
Use this integration frame whenever COMLEX includes structural findings or OMT among the options. See Fig 6.
B Worked example
A 35-year-old woman presents 2 days after a low-speed MVC with neck pain and mild headache. She has asthma and generalized anxiety disorder. She is afebrile, neurologically intact, and hemodynamically stable. Exam notes paraspinal hypertonicity and restricted cervical rotation. The question asks for the most appropriate next step. One option is gentle OMT; another is urgent CT head; another is cervical HVLA; another is discharge without assessment.
Reasoning chain: Identify task → next step. Extract key facts → stable patient, no focal deficits, no red flags, structural findings support a musculoskeletal component. Apply rule → osteopathic care may be appropriate if safe, but forceful technique selection matters; recent trauma makes some maneuvers less appropriate until serious injury is excluded. Eliminate distractors → urgent CT head is tempting because of headache after MVC, but no red flags are provided. Cervical HVLA is tempting because it is OMT-related, but safety and recent trauma make it a poor immediate choice. Verify → the best answer is the safe, appropriately timed action that fits both the task and contraindication profile.
C Exam trap
Common wrong answer: Choose any OMT option simply because the exam is COMLEX and structural findings appear in the stem.
Why it is tempting: The learner expects an osteopathic twist and overweights that cue.
Single clue that eliminates it: OMT must still pass category, timing, and safety checks; recent trauma, infection, fracture, acute surgical abdomen, or instability may require deferral or technique modification.
D Checkpoint
Question: Which rule best helps eliminate close-call answer choices on COMLEX vignettes?
- Pick the most definitive intervention available — Tempting because definitive care sounds strong, but wrong when timing or stability makes a simpler earlier step correct.
- Pick the most osteopathic option whenever structural findings are present — Tempting because COMLEX includes OMM, but wrong because OMT must still be indicated and safe.
- Choose the option that matches category, acuity, timing, and safety — Tempting because it seems procedural, and right because it systematically removes mistimed or contraindicated answers.
- Ignore the final sentence and solve the diagnosis first — Tempting because disease recognition is familiar, but wrong because it can lead you to answer a different task than the one asked.
Answer: C.
Exam Traps & Differentiators
Most common wrong answer and why: The most common wrong answer is the true but mistimed option. It is tempting because it is medically correct in a similar patient, but it fails the current task.
| Looks similar | Actually tested task | What separates them | Board-style clue |
|---|---|---|---|
| Most accurate test | Best initial test | Safety and sequence | “Initial” or “first study” |
| Definitive treatment | Most appropriate next step | Timing now | “Next step” in unstable patient |
| Diagnosis label | Immediate stabilization | Instability overrides naming | Hypotension, hypoxia, AMS |
| Any OMT option | Safe integrated care | Contraindications and deferral | Trauma, fracture, acute abdomen, shock |
| Routine follow-up | Requires admission/escalation | Disposition risk | Toxic appearance, poor support, failed outpatient care |
| If the stem says... | Think... |
|---|---|
| “Most likely diagnosis” | Name the disease; do not pick a test or treatment |
| “Best initial test” | Choose the first safe high-yield study, not the gold standard |
| “Most appropriate next step” | Sequence care based on urgency and what changes management now |
| “Requires immediate clarification” | Find the safety gap, contraindication, or professionalism issue |
| “Most important to monitor” | Track the complication most likely to cause harm |
| “Stable patient” versus “hypotensive/confused/hypoxic” | Task family may switch from workup to stabilization |
Related confusions from neighboring topics: In the upcoming Red Flags And Instability, many wrong answers will be test-before-resuscitate errors. In Best Next Step Logic, many wrong answers will be right-category but wrong-sequence choices. This topic is the foundation for both.
Exam takeaway: The best answer is often distinguished from close distractors by timing and safety rather than by disease knowledge alone.
flowchart LR
A[Option under review] --> B{Same category as task?}
B -->|No| X[Eliminate]
B -->|Yes| C{Right timing?}
C -->|No| X
C -->|Yes| D{Safe for this patient?}
D -->|No| X
D -->|Yes| E[Keep as contender] Exam takeaway: Close-call distractors often represent the right action for a slightly different patient or a later stage of care.
Algorithm / Approach
| Step | Question to ask yourself | What a strong test taker does |
|---|---|---|
| 1 | What is the stem asking me to do? | Identifies task family before reading options |
| 2 | Is the patient stable? | Lets instability override planned workup |
| 3 | Which clues actually change the answer? | Uses 2–4 pivot facts, ignores noise |
| 4 | Which options are mistimed or unsafe? | Eliminates true-but-wrong-now answers |
| 5 | Would this be right for this exact patient now? | Checks age, pregnancy, trauma, contraindications, acuity |
Rapid Review
- Final sentence → defines the task more reliably than the stem’s most vivid clue
- Best initial test → first safe high-yield study, not the most accurate confirmatory test
- Most appropriate next step → timing question, not necessarily a disease-identification question
- Instability → converts many items into stabilization-first decisions
- Noise → real detail that does not alter urgency, diagnosis, contraindication, or disposition
- Mixed answer categories → sign you must classify the task before comparing options
- Gold-standard trap → common wrong answer when the question asks for initial action
- Definitive-treatment trap → common wrong answer when another step must come first
- Pregnancy detail → often changes imaging or medication choice even when not the diagnosis
- Hypotension/hypoxia/AMS → task-changing clues with high board value
- OMT option on COMLEX → correct only if it matches task and is safe in context
- Disposition question → asks risk, support, monitoring needs, and failure of outpatient safety
- Ethics/safety wording → may test clarification, consent, confidentiality, or escalation rather than pathophysiology
- CATS filter → Category, Acuity, Timing, Safety
Self-check quiz
1.1.1.8 Question 1
A 46-year-old man with hypertension presents with classic burning retrosternal discomfort after meals that improves with antacids. Vitals are normal, ECG is normal, and the stem asks for the most likely diagnosis. Which option best matches the task?
- Gastroesophageal reflux disease
- Upper endoscopy
- Proton pump inhibitor therapy
- Hospital admission for telemetry
1.1.1.9 Question 2
A 22-year-old woman with no major medical history presents with dysuria and urinary frequency for 2 days. She is afebrile and hemodynamically stable. The question asks for the best initial test. Which option is the best match to the task family?
- Urinalysis
- Urine culture sensitivity-guided antibiotic selection
- Nitrofurantoin therapy
- CT abdomen and pelvis
1.1.1.10 Question 3
A 68-year-old woman with diabetes and peripheral vascular disease presents with fever, confusion, and a painful erythematous leg wound. She also mentions chronic insomnia. Temperature is 39.1°C, blood pressure 86/50 mm Hg, pulse 122/min. The question asks for the most appropriate next step. Which option is best?
- Obtain wound culture results before starting therapy
- Begin broad stabilization and empiric sepsis treatment
- Schedule outpatient vascular surgery follow-up
- Order ankle-brachial index testing first
1.1.1.11 Question 4
A 29-year-old pregnant woman at 10 weeks presents with right lower quadrant pain and nausea. She has migraines and mild asthma. She ate undercooked food yesterday and has a mild leukocytosis. The stem asks for the best initial imaging study. Which answer is most appropriate?
- CT abdomen/pelvis with contrast
- MRI brain
- Pelvic and abdominal ultrasound
- Diagnostic laparoscopy immediately
1.1.1.12 Question 5
A 56-year-old man 6 days after orthopedic surgery develops pleuritic chest pain and dyspnea. He has obesity and OSA. He is anxious but normotensive. The question asks for the best initial diagnostic test for suspected pulmonary embolism. Which option best fits the task?
- Heparin infusion
- CT pulmonary angiography
- Thrombolytic therapy
- ICU admission without imaging
1.1.1.13 Question 6
A 34-year-old woman 2 days after a minor MVC presents with neck pain and limited range of motion. She has anxiety and well-controlled asthma. She is afebrile, neurologically intact, and hemodynamically stable. The stem asks for the most appropriate next step; options include several osteopathic and imaging choices. Which principle should most strongly guide elimination of answers?
- Always choose an OMT option when structural findings are provided
- Ignore trauma history because the patient is young
- Use category, acuity, timing, and safety to filter options
- Choose the most definitive imaging study available
1.1.1.14 Question 7
A 73-year-old man with heart failure and chronic kidney disease presents with crushing chest pain, diaphoresis, and nausea. He says the pain began after dinner and feels like prior reflux. Blood pressure is 82/54 mm Hg, pulse 118/min, and ECG shows ST elevations in inferior leads. The question asks for the most appropriate next step. Which answer is best?
- Trial of GI cocktail and reassessment
- Serum troponin confirmation before treatment
- Immediate STEMI-directed stabilization and reperfusion pathway
- Outpatient stress testing within 72 hours
1.1.1.15 Question 8
A 17-year-old adolescent presents for sports clearance after a recent urgent care visit for exertional syncope. He has no current symptoms, and exam today is normal except for a systolic murmur that increases with Valsalva. He also reports seasonal allergies. The question asks which finding requires immediate clarification before clearance. Which choice is best?
- Seasonal allergic rhinitis
- History of exertional syncope
- Occasional tension headaches
- Prior ankle sprain
Answer key
1.1.1.16 Question 1 Answer: A. Gastroesophageal reflux disease
Why A is correct: The pathophysiology is gastric acid reflux causing classic postprandial burning pain relieved by antacids. The single discriminating clue is that the stem asks for the most likely diagnosis, so the correct answer must be a diagnosis, not a test or treatment. This matches task recognition rather than management sequencing. Sources: American College of Gastroenterology guidance; Harrison’s Principles of Internal Medicine.
Why B is tempting but wrong: Upper endoscopy is tempting because it is a legitimate diagnostic tool for selected GERD patients with alarm features. It is wrong here because the question asks for the diagnosis, and the clue that discriminates is the final sentence, not the availability of further testing. Sources: ACG; Harrison’s.
Why C is tempting but wrong: PPI therapy is tempting because it is first-line treatment for typical GERD symptoms. It is incorrect for this specific item because treatment is the wrong category; the stem asks what the condition most likely is. The discriminating clue is category mismatch. Sources: ACG; First Aid.
Why D is tempting but wrong: Admission is tempting because chest pain can be dangerous, but the patient is stable, ECG is normal, and the symptom pattern is classic for reflux. The discriminating clue is the benign pattern plus the diagnostic wording of the question. Sources: Harrison’s; UpToDate.
1.1.1.17 Question 2 Answer: A. Urinalysis
Why A is correct: The stem asks for the best initial test in a stable patient with uncomplicated lower urinary symptoms. Urinalysis is the appropriate first study because it matches the task family and the stage of care. The discriminating clue is “initial test.” Sources: Harrison’s; UpToDate UTI evaluation guidance.
Why B is tempting but wrong: Urine culture may be appropriate in more complex or recurrent cases, and sensitivity data help refine treatment. It is incorrect here because it is more confirmatory/refinement-oriented than the initial test asked for. The discriminating clue is uncomplicated presentation in a stable patient. Sources: UpToDate; Harrison’s.
Why C is tempting but wrong: Nitrofurantoin is a plausible treatment for uncomplicated cystitis. It is wrong because the task is testing, not therapy. The single clue is the final sentence asking for the best initial test. Sources: UpToDate; First Aid.
Why D is tempting but wrong: CT is tempting if one overthinks obstruction or stone disease, but there are no features suggesting complicated upper-tract pathology. The discriminating clue is a straightforward lower urinary symptom pattern in a stable patient. Sources: Harrison’s; UpToDate.
1.1.1.18 Question 3 Answer: B. Begin broad stabilization and empiric sepsis treatment
Why B is correct: The mechanism is presumed severe infection causing septic shock physiology, reflected by fever, hypotension, tachycardia, and confusion. The correct management logic is diagnosis-mechanism-treatment: likely sepsis, organ hypoperfusion, immediate resuscitation and empiric therapy. The single clue is hypotension with altered mental status, which changes the task to urgent stabilization. Sources: Surviving Sepsis Campaign; Harrison’s.
Why A is tempting but wrong: Cultures matter and are part of sepsis workup, so this feels systematic. It is wrong because waiting for culture results delays life-saving treatment. The discriminating clue is shock-level blood pressure, not the wound itself. Sources: Surviving Sepsis Campaign; JAMA reviews.
Why C is tempting but wrong: Vascular surgery follow-up may matter later in peripheral vascular disease and wound healing. It is incorrect now because outpatient planning is unsafe in an unstable septic patient. The discriminating clue is immediate physiologic compromise. Sources: Harrison’s; UpToDate.
Why D is tempting but wrong: ABI is tempting because vascular disease contributes to wound complications. It is wrong because it does not address the emergent process causing shock. The discriminating clue is sepsis physiology, which overrides chronic limb assessment. Sources: Harrison’s; Surviving Sepsis Campaign.
1.1.1.19 Question 4 Answer: C. Pelvic and abdominal ultrasound
Why C is correct: The stem asks for the best initial imaging study in a pregnant patient with RLQ pain. Pregnancy is the discriminating clue because it changes the safest first imaging choice. Ultrasound matches the initial-test task and avoids unnecessary radiation. Sources: ACOG guidance; Harrison’s.
Why A is tempting but wrong: CT can be tempting because it is often high-yield for appendicitis in nonpregnant adults. It is wrong here because pregnancy shifts the initial imaging approach. The single discriminating clue is the positive pregnancy status. Sources: ACOG; UpToDate.
Why B is tempting but wrong: MRI is a valuable modality in many settings, but brain MRI is unrelated to the anatomic problem being assessed. It remains plausible only if one gets distracted by her migraine history; that history is noise. Sources: Harrison’s.
Why D is tempting but wrong: Immediate laparoscopy may be needed in selected unstable or clearly surgical cases, but the stem asks for initial imaging in a stable patient. The discriminating clue is stable presentation plus explicit imaging task. Sources: ACOG; Harrison’s.
1.1.1.20 Question 5 Answer: B. CT pulmonary angiography
Why B is correct: The mechanism is a postoperative venous thromboembolic event causing pleuritic chest pain and dyspnea. The task asks for the best initial diagnostic test in a stable patient with likely PE, so CT pulmonary angiography is the best fit among the options provided. The single discriminating clue is that he is normotensive, so the question remains in diagnostic mode rather than immediate rescue mode. Sources: ACCP/Chest guidance; Harrison’s.
Why A is tempting but wrong: Heparin is tempting because anticoagulation is part of PE management. It is wrong in this item because the stem explicitly asks for the initial diagnostic test, not treatment. The discriminating clue is task family mismatch. Sources: CHEST; UpToDate.
Why C is tempting but wrong: Thrombolysis is tempting if one thinks “serious PE,” but it is usually reserved for hemodynamic instability or certain high-risk situations. The discriminating clue is preserved blood pressure. Sources: CHEST; Harrison’s.
Why D is tempting but wrong: ICU admission is plausible in severe cardiopulmonary illness, but without instability it skips the diagnostic task being asked. The discriminating clue is stable hemodynamics with an explicit testing question. Sources: Harrison’s; CHEST.
1.1.1.21 Question 6 Answer: C. Use category, acuity, timing, and safety to filter options
Why C is correct: The mechanism here is not disease-specific but reasoning-specific: several options may seem plausible, especially in a COMLEX stem with structural findings after trauma. The correct discriminator is the CATS framework because it filters options by task category, urgency, correct stage of care, and contraindications. Sources: Savarese-style osteopathic reasoning principles; Harrison’s trauma safety logic.
Why A is tempting but wrong: Structural findings make OMT feel expected on COMLEX. It is wrong because osteopathic care must still be indicated and safe; recent trauma may alter technique choice or require further assessment. The discriminating clue is trauma history. Sources: Osteopathic principles texts; UpToDate cervical trauma evaluation.
Why B is tempting but wrong: Youth can lower some risks, so this may sound pragmatic. It is incorrect because age never cancels the relevance of recent trauma when selecting a safe next step. The discriminating clue is not age but mechanism and safety. Sources: Harrison’s; emergency care references.
Why D is tempting but wrong: Definitive imaging feels thorough, but board questions often punish overtesting when the task is a more immediate and appropriate action. The discriminating clue is that correct answers are chosen by fit to task and safety, not by maximal diagnostic intensity. Sources: Harrison’s; UpToDate.
1.1.1.22 Question 7 Answer: C. Immediate STEMI-directed stabilization and reperfusion pathway
Why C is correct: The pathophysiology is acute coronary occlusion with inferior STEMI causing hypotension and ongoing ischemia. The management logic is immediate stabilization and reperfusion-oriented care because the patient is unstable and the ECG already provides decisive evidence. The single clue that discriminates is ST elevation plus hypotension. Sources: AHA/ACC STEMI guidelines; Harrison’s.
Why A is tempting but wrong: GI symptoms after dinner and a reflux-like description make a GI cocktail tempting. It is wrong because the ECG and shock physiology identify a time-sensitive cardiac emergency. The discriminating clue is objective STEMI evidence, not the meal-associated history. Sources: AHA/ACC; Harrison’s.
Why B is tempting but wrong: Troponin confirmation sounds diagnostically tidy. It is incorrect because waiting for biomarkers delays care in a patient with diagnostic ECG findings and instability. The discriminating clue is that the diagnosis is already actionable. Sources: AHA/ACC; UpToDate.
Why D is tempting but wrong: Stress testing is used in selected chest pain evaluation, which makes it superficially plausible. It is grossly mistimed here because the patient has an active STEMI with shock. The discriminating clue is acuity. Sources: AHA/ACC; Harrison’s.
1.1.1.23 Question 8 Answer: B. History of exertional syncope
Why B is correct: The mechanism is potential occult cardiac pathology causing exertional loss of consciousness, which is a major patient-safety issue in sports clearance. The stem specifically asks what requires immediate clarification before clearance, making this a safety/disposition task rather than a benign screening question. The single discriminating clue is syncope during exertion, especially with a murmur that increases with Valsalva. Sources: AHA preparticipation evaluation guidance; Harrison’s.
Why A is tempting but wrong: Allergic rhinitis is common and may matter for symptom control, so it is plausible in a general clinic stem. It is incorrect because it does not create an immediate safety barrier to sports clearance. The discriminating clue is lack of cardiovascular risk significance. Sources: AHA guidance; UpToDate.
Why C is tempting but wrong: Headaches can suggest exertional concerns in some contexts, but occasional tension headaches are not the urgent safety issue here. The discriminating clue is exertional syncope, which has far greater prognostic significance. Sources: AHA; Harrison’s.
Why D is tempting but wrong: Prior ankle sprain is relevant to orthopedic history and sports participation, making it plausibly testable. It is wrong because it does not demand immediate clarification before clearance in the way potential cardiogenic syncope does. The discriminating clue is risk of sudden cardiac events. Sources: AHA; UpToDate.