Why it matters
- Low cardiac output can look like “just a soft blood pressure” until urine output falls, mentation worsens, and shock is already progressing.
- On CCRN items, the correct answer often depends on whether the patient needs volume, cannot tolerate more volume, or has a different hemodynamic problem entirely.
- Preload is tested because it links assessment findings, invasive monitoring, fluid balance, and nursing prioritization in one decision.
- Trend recognition matters more than isolated numbers: a normal-looking pressure can still mask falling perfusion if compensatory vasoconstriction is present.
Key Terms & Must-Know Facts
1.1.1.1 Key terms
- Cardiac output (CO): Amount of blood ejected by the heart per minute.
- Stroke volume (SV): Blood ejected with each heartbeat.
- Heart rate (HR): Beats per minute; one determinant of CO.
- Cardiac index (CI): CO adjusted for body surface area.
- Preload: Ventricular filling/stretch at end diastole.
- Venous return: Blood returning to the heart; major contributor to preload.
- Frank-Starling relationship: Within limits, more filling can increase SV.
- Preload responsiveness: CO/SV likely rises with additional volume.
- Fluid intolerance: Extra volume worsens congestion without meaningful perfusion benefit.
- CVP: Central venous pressure; an imperfect estimate of right-sided filling pressure.
- PAOP/PCWP: Pulmonary artery occlusion pressure; estimate of left-sided filling pressure when measured correctly.
- Perfusion: Delivery of blood flow to tissues.
- End-organ hypoperfusion: Inadequate flow to organs, often seen as oliguria, altered mentation, cool skin, or elevated lactate.
1.1.1.2 Must-know facts
- ( CO = HR times SV )
- Cardiac index is often more useful than CO alone because it accounts for body size.
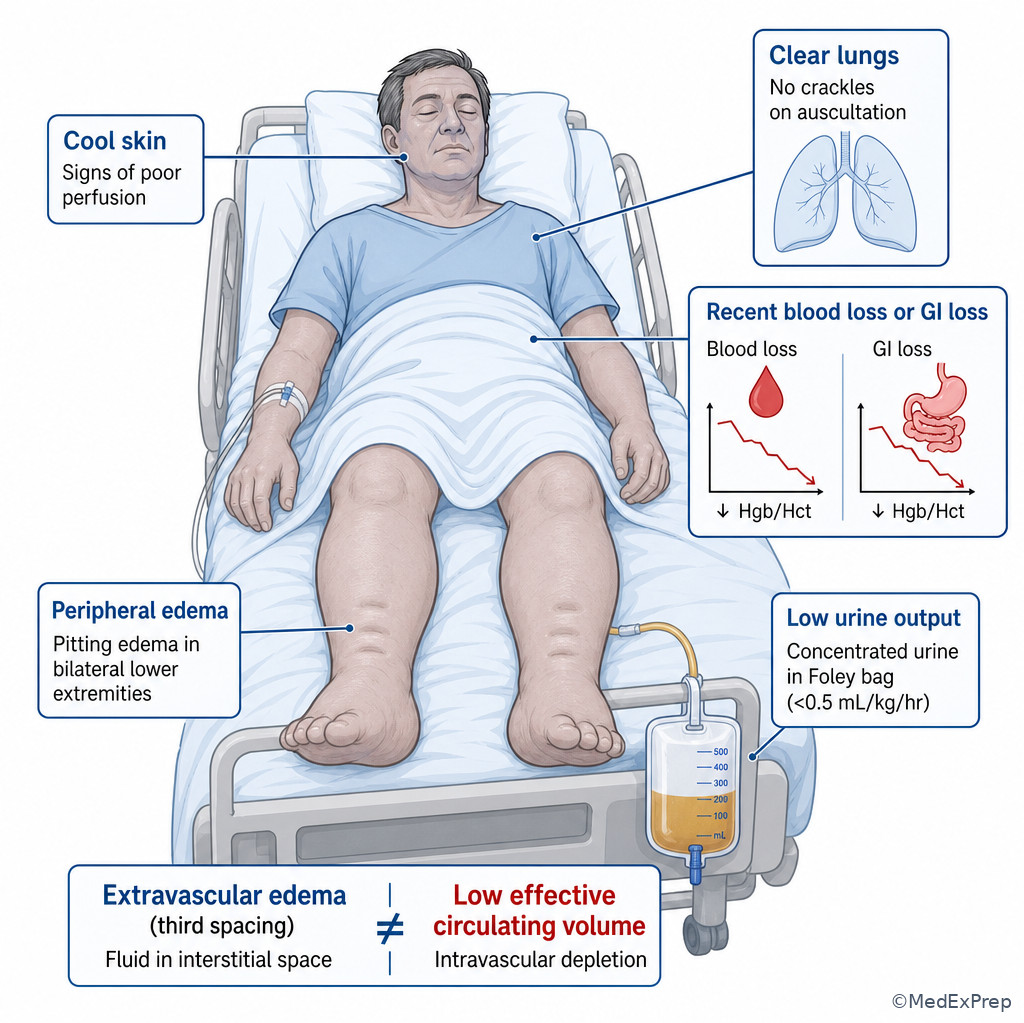
- Preload is not the same as total body fluid; a patient can be edematous yet intravascularly underfilled.
- Filling pressure numbers alone do not prove fluid responsiveness.
- Tachycardia may temporarily preserve CO, but excessive HR can reduce diastolic filling and lower SV.
- Urine output less than about 0.5 mL/kg/hr suggests possible poor renal perfusion in the adult ICU patient.
- Warm flushed skin can occur in distributive states despite poor effective perfusion.
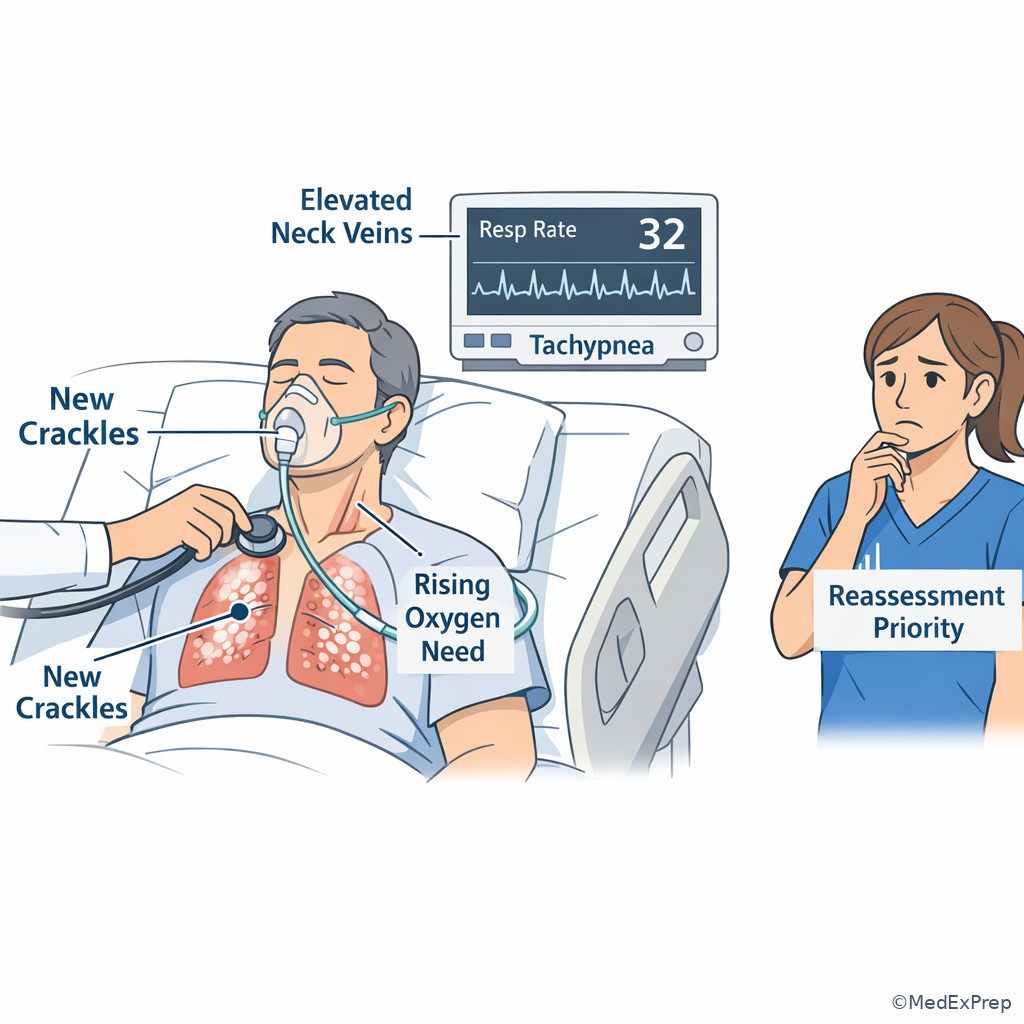
- Crackles, rising oxygen needs, and worsening pulmonary congestion are major clues to reject more fluid.
- The CCRN answer should stay in RN scope: assess, trend, intervene per orders/protocol, and escalate unsafe changes.
Core content
1.1.1.3 Foundational hemodynamic logic: what cardiac output and preload actually mean
A Explanation
The first decision conflict is simple but highly tested: Is the stem asking about flow or filling? Cardiac output is flow per minute. Preload is ventricular filling before contraction. Students often collapse them into one idea, but on exam stems they solve different problems. If the question asks why organs are underperfused, think about inadequate output. If the question asks whether the ventricle has enough volume to fill effectively, think about preload. The single rule that resolves many items is this: preload is one determinant of stroke volume, not a guarantee of adequate cardiac output.
Within the Frank-Starling range, increasing ventricular filling can increase stroke volume. Beyond that range, extra filling mainly increases congestion. That is why a patient with heart failure may have high filling pressures and edema yet still have poor cardiac output. On the other hand, a patient after hemorrhage may have low preload and low cardiac output because the ventricle has too little volume to eject. See Fig 1.
WHY THIS IS TESTED: CCRN items want you to choose between “give volume,” “hold volume,” “reassess another cause,” or “escalate,” using bedside physiology rather than memorized pressure cutoffs.
Key rule: Low blood pressure does not automatically equal low preload. The discriminating question is whether the patient shows evidence of underfilling with likely fluid responsiveness versus congestion or another hemodynamic problem.
Recall: This is the first topic in the course, so build your baseline framework here: identify the task, extract cues, decide whether the problem is flow, filling, or perfusion, then act within RN scope.
Exam takeaway: Separate filling from flow so you do not treat every hypotensive patient with more fluid.
flowchart TD
A[Bedside question] --> B{Problem is mainly?}
B --> C[Low filling = low preload]
B --> D[Low flow = low cardiac output]
C --> E[Possible causes: bleeding, dehydration, vasodilation with venous pooling]
D --> F[Possible causes: poor contractility, dysrhythmia, extreme tachycardia, severe valve problem]
C --> G[Clues: flat neck veins, low urine output, dry trend, possible preload response]
D --> H[Clues: weak pulse, fatigue, low CI trend, organ hypoperfusion]
G --> I[Need reassessment before fluid decision]
H --> I Nursing Priority: Assess first: ABCs, mental status, pulse quality, blood pressure trend, urine output, and signs of congestion. Intervene: optimize positioning, ensure monitoring accuracy, implement ordered fluids or titration only if appropriate and within protocol. Delegate: routine intake/output collection or repeat noninvasive vitals may go to assistive personnel, but hemodynamic interpretation stays with the RN. Escalate: persistent hypotension, worsening mentation, chest pain, new pulmonary edema, or signs of shock require immediate provider notification or rapid response per policy.
B Worked example
A 67-year-old man in the ICU after major abdominal surgery has coronary artery disease, type 2 diabetes, and chronic hypertension. He is pale and restless. HR 122/min, BP 88/54 mm Hg, RR 24/min, SpO2 95% on 2 L nasal cannula, urine output 15 mL in the last hour. His temperature is 37.8°C, and a morning chest x-ray mentions mild bibasilar atelectasis. The nurse is asked which hemodynamic concept best explains the likely immediate problem.
Identify the task: The stem asks for the hemodynamic problem driving poor perfusion.
Extract key facts: Postoperative setting, tachycardia, hypotension, oliguria, restlessness, pallor. The chest x-ray note is distracting noise; mild atelectasis does not explain the perfusion pattern.
Apply rule: These cues fit possible low preload with resulting low stroke volume and low cardiac output until proven otherwise.
Eliminate distractors: “Afterload” would be a poor first explanation because the pattern is more suggestive of underfilling than high resistance. “Contractility failure” is possible later in the differential, but no clue is stronger than postoperative low circulating volume. “Oxygenation failure” is tempting because of the chest x-ray, but the oxygen saturation is acceptable.
Verify: The safest RN thinking is that reduced preload may be lowering stroke volume and cardiac output; the nurse should reassess for bleeding, check trends, and escalate or implement ordered resuscitation.
C Exam trap
Common wrong answer: “The patient has low cardiac output, so preload is not relevant.” WHY IT IS TEMPTING: The stem shows obvious hypoperfusion, and candidates jump straight to the final effect. SINGLE CLUE THAT ELIMINATES IT: The exam often wants the upstream determinant. In an underfilled ventricle, low preload is the actionable mechanism leading to reduced stroke volume.
D Checkpoint
Which finding most strongly supports low preload as a contributor to reduced cardiac output in an adult ICU patient?
- A. Tachycardia with low urine output after several hours of high nasogastric losses
- B. New S3 gallop with bilateral crackles after repeated fluid boluses
- C. Bounding pulses and warm flushed skin during early sepsis
- D. Hypertension with widened pulse pressure during pain and agitation
Correct answer: A
- A: Tempting because it points to volume loss; correct because GI losses plus tachycardia and oliguria support reduced filling and possible preload responsiveness.
- B: Tempting because CO may still be poor; wrong because S3 and crackles after boluses suggest volume intolerance, not low preload.
- C: Tempting because perfusion is abnormal; wrong because warm distributive findings point more toward vasodilation than isolated low preload.
- D: Tempting because BP changes affect hemodynamics; wrong because pain-related hypertension does not indicate underfilling.
1.1.1.4 Determinants and bedside markers: when low preload helps explain the whole picture
A Explanation
The next decision conflict is: Does this patient appear underfilled, or is there another reason perfusion is poor? At the bedside, preload depends on venous return, intravascular volume, venous tone, diastolic filling time, and ventricular compliance. Low preload can come from bleeding, dehydration, diuresis, third spacing, vasodilation with venous pooling, or obstructed return. High preload can occur with fluid overload, ventricular failure, and valvular dysfunction. The resolving rule is that preload must be judged by pattern recognition, not one isolated pressure value.
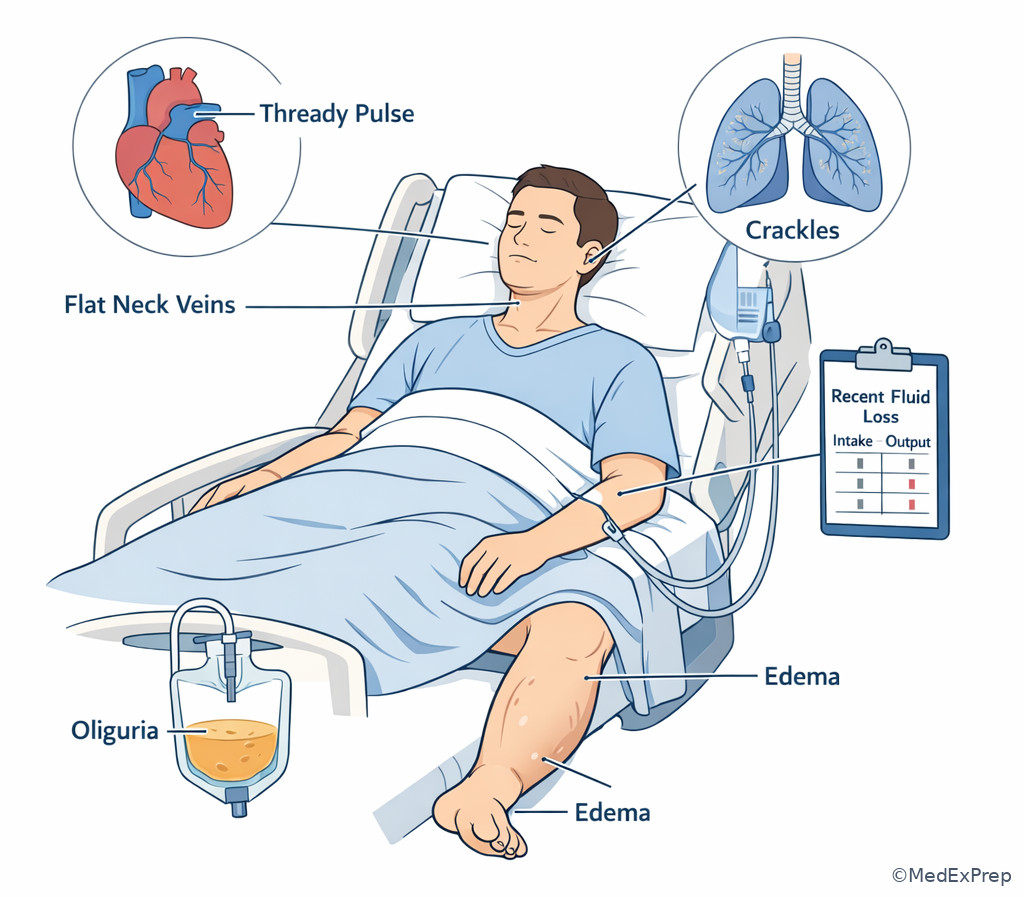
Clues that support low preload include recent fluid losses, bleeding risk, orthostatic-type trend if measurable, low CVP trend if available, flat neck veins, cool extremities, thready pulse, delayed capillary refill, falling urine output, and possible improvement after a small ordered fluid challenge. Clues that argue against more fluid include crackles, pulmonary edema, rising oxygen requirement, increasing work of breathing, JVD, edema with high filling pressures, or no improvement in perfusion despite prior boluses. See Fig 2.
WHY THIS IS TESTED: The exam expects the RN to avoid reflexive fluid administration when lung congestion or pump failure is the stronger clue.
Common pitfall: Edema does not guarantee adequate preload. Critically ill patients can be third-spaced and intravascularly depleted at the same time.
High-Yield Connection: This concept is tested alongside Afterload, Contractility, And MAP. Know both underfilling clues and vasodilatory clues for exam day — they are frequently paired in stems.
Exam takeaway: Use congestion clues to reject more volume even when blood pressure is low.
flowchart LR
A[Hypotension or low perfusion] --> B{Which pattern dominates?}
B --> C[Underfilled pattern]
B --> D[Congestion pattern]
C --> E[Losses, bleeding, low UO, cool skin, thready pulse]
C --> F[May improve with ordered volume]
D --> G[Crackles, JVD, rising O2 need, edema, S3]
D --> H[More fluid may worsen gas exchange]
E --> I[Reassess response]
H --> I Exam takeaway: Organize preload assessment around volume losses, venous return, and congestion findings rather than a single monitor value.
Memory anchor: “FILL” for underfilling clues — Fluid losses, Inadequate urine, Low-pressure trend, Light/flat neck veins.
Nursing Priority: Assess first: volume loss history, lung sounds, oxygen requirement, neck veins, edema, urine output, and mental status. Intervene: maintain accurate I&O, verify line patency and pressure transducer setup if present, and implement ordered fluid trial only after reassessing for congestion. Delegate: weights and basic output measurements may be delegated per policy, but interpretation of preload adequacy remains RN work. Escalate: worsening crackles, new frothy sputum, persistent hypotension, or no improvement after ordered intervention.
B Worked example
A 74-year-old woman with heart failure with reduced ejection fraction, chronic kidney disease, and atrial fibrillation is admitted with urosepsis. She received 2 liters of crystalloid in the ED. Four hours later she is confused, BP 86/50 mm Hg, HR 118/min, RR 30/min, SpO2 89% on 4 L nasal cannula, urine output 20 mL/hr. Crackles are now heard halfway up both lung fields, and the chest x-ray report mentions pulmonary vascular congestion. Lactate is 4.1 mmol/L. A novice nurse says, “Her pressure is low, so she obviously needs more fluid.”
Identify task: Determine the safest next nursing interpretation and priority action.
Extract key facts: Hypotension and oliguria suggest poor perfusion, but new hypoxemia, tachypnea, and diffuse crackles after fluids argue against more volume.
Apply rule: Low blood pressure alone does not prove low preload. The dominant pattern is now fluid intolerance or pump limitation, not simple underfilling.
Eliminate distractors: The sepsis label is tempting and may push candidates toward more boluses, but respiratory congestion is the single clue that changes the decision. Holding all interventions would also be wrong; the RN must reassess, support oxygenation, and escalate promptly.
Verify: The safest bedside action is to address airway/breathing, position upright if tolerated, reassess response, and notify the provider or rapid response per severity rather than assuming more fluid.
C Exam trap
Common wrong answer: “Continue fluid boluses because lactate is elevated.” WHY IT IS TEMPTING: Elevated lactate and hypotension fit shock, and fluids are often associated with shock treatment. SINGLE CLUE THAT ELIMINATES IT: New bilateral crackles with worsening oxygenation after prior fluids point away from additional preload as the safest immediate answer.
D Checkpoint
Which finding most strongly argues against another fluid bolus as the priority nursing expectation?
- A. Urine output 20 mL/hr
- B. Heart rate 116/min
- C. New crackles with increasing oxygen requirement after prior fluids
- D. Lactate 3.8 mmol/L
Correct answer: C
- A: Tempting because oliguria reflects hypoperfusion; wrong because it does not tell you whether more fluid is safe.
- B: Tempting because tachycardia may indicate hypovolemia; wrong because it is nonspecific.
- C: Tempting because you might focus only on breathing; correct because congestion after prior fluids is the strongest clue that more preload may worsen the patient.
- D: Tempting because elevated lactate supports shock; wrong because it identifies poor perfusion, not the safest specific intervention.
- The formula for cardiac output is ___ × ___.
- True or False: Peripheral edema always means adequate intravascular preload.
- Name 3 bedside findings that suggest fluid intolerance rather than underfilling.
1.1.1.5 Monitoring preload and output: what numbers help, what numbers mislead
A Explanation
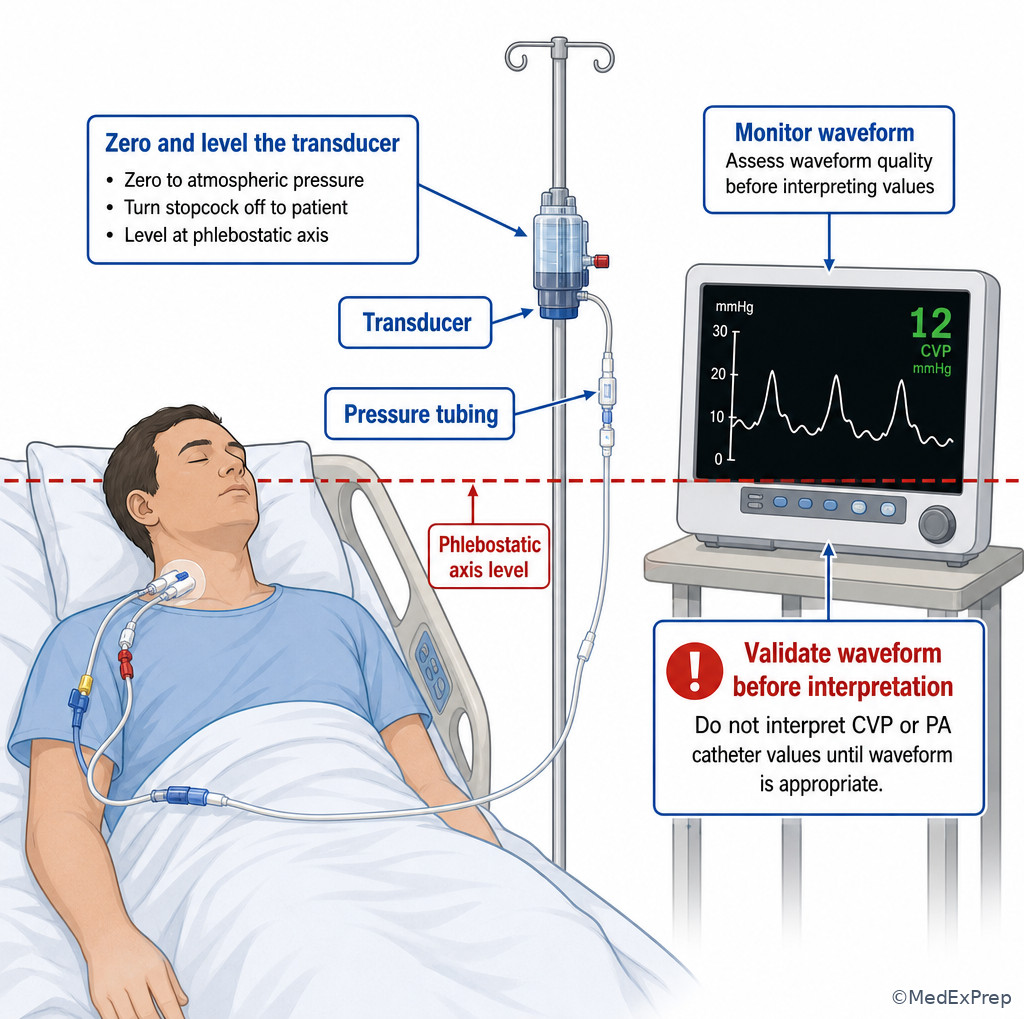
The next decision conflict is: Should I trust the number, or should I trust the trend and clinical picture? In CCRN-style hemodynamics, the correct move is usually to integrate both. Heart rate, blood pressure, MAP, urine output, peripheral perfusion, lactate, mental status, CVP trend, and if available CI and PAOP can all contribute. The single rule is this: no single preload marker is sufficient by itself. Static numbers such as CVP may be abnormal for many reasons, including intrathoracic pressure changes, right ventricular dysfunction, or measurement error.
CVP can be useful as a trend when interpreted with the whole picture, especially in the same patient over time. A very low CVP in a patient with losses and poor perfusion may support underfilling. A high CVP with JVD and edema may support venous congestion, but it still does not tell you left-sided filling or whether the patient will benefit from fluid. PAOP, when a pulmonary artery catheter is present and the waveform is valid, helps estimate left ventricular preload more directly than CVP. Cardiac index better reflects flow than blood pressure alone. See Fig 4.
WHY THIS IS TESTED: Many exam distractors offer a “normal” or “abnormal” number that seems decisive. The better answer usually uses trend + patient response + consistency of the data.
Key rule: A patient can maintain a near-normal blood pressure through vasoconstriction while cardiac output is falling. End-organ cues may reveal deterioration earlier than the cuff pressure.
Exam takeaway: Treat discordant numbers by validating the line, checking the trend, and matching the value to the bedside assessment.
flowchart TD
A[New hemodynamic value] --> B[Validate setup and waveform]
B --> C[Compare with prior trend]
C --> D[Match to bedside findings]
D --> E{Consistent?}
E -->|Yes| F[Use for nursing prioritization]
E -->|No| G[Reassess line, patient position, timing, and escalation]
F --> H[Track response to intervention] Exam takeaway: Validate leveling, zeroing, and waveform quality before acting on invasive pressure values.
High-Yield Connection: This concept overlaps directly with Pulmonary Artery Catheter Data. Know both the filling-pressure numbers and the nursing safety checks for line accuracy; exam stems often combine them.
Nursing Priority: Assess first: whether the invasive reading is technically valid and whether it fits the patient’s clinical state. Intervene: re-level/zero per policy, obtain repeat data if appropriate, and correlate with urine output, lactate, and mental status. Delegate: invasive-line interpretation cannot be delegated. Escalate: sudden value changes with instability, dampened or abnormal waveform suggesting malfunction, or sustained low perfusion despite intervention.
B Worked example
A 58-year-old man with pancreatitis, obesity, and chronic obstructive pulmonary disease is mechanically ventilated in the ICU. He has a central line and arterial line. The monitor shows CVP 14 mm Hg, BP 90/58 mm Hg, HR 124/min, urine output 10–15 mL/hr, and rising lactate. The respiratory therapist notes high PEEP. The novice interpretation is, “CVP is high, so he definitely has too much preload.”
Identify task: Interpret whether one invasive value is enough to reject low effective preload.
Extract key facts: High PEEP can elevate intrathoracic pressure and influence CVP. The patient also has poor perfusion and critical illness that may distort static filling measures.
Apply rule: A static CVP alone does not settle the preload question. The value must be validated and interpreted in context.
Eliminate distractors: Automatically giving diuretics would be unsafe because the “high” CVP may not represent true fluid overload. Automatically flooding with fluid is also unsafe without considering respiratory status and other data. The best RN response is to confirm setup, integrate the trend, and escalate discordant findings.
Verify: This is a classic item where the exam rewards trend-based nursing judgment over single-number reflexes.
C Exam trap
Common wrong answer: “CVP is elevated, so preload is adequate.” WHY IT IS TEMPTING: Static filling pressure seems objective and easier than trend interpretation. SINGLE CLUE THAT ELIMINATES IT: Mechanical ventilation, PEEP, right-heart factors, and measurement setup can all distort the reading; the patient’s persistent hypoperfusion means one number is not enough.
D Checkpoint
Which nursing interpretation is most appropriate when a new invasive pressure value does not match the bedside picture?
- A. Treat the number as definitive because invasive data are more reliable than assessment findings
- B. Validate setup and waveform, compare with prior trend, and correlate with perfusion findings
- C. Ignore the number completely and use only urine output
- D. Ask the provider to choose the medical plan before doing further nursing reassessment
Correct answer: B
- A: Tempting because invasive monitoring appears precise; wrong because technical or physiologic factors can mislead.
- B: Tempting because it takes more work; correct because CCRN reasoning favors validated trend integration.
- C: Tempting because urine output reflects perfusion; wrong because it throws away useful hemodynamic data.
- D: Tempting because the patient is unstable; wrong because the RN should first reassess and validate within scope while escalating.
1.1.1.6 Preload responsiveness versus fluid overload: choosing the safer bedside action
A Explanation
The central application question is: Will more volume likely help, or is more volume likely to harm? Preload responsiveness means stroke volume or cardiac output is likely to rise meaningfully with additional volume. It does not mean every hypotensive patient should receive fluid. A patient may be hypotensive from vasodilation, bradyarrhythmia, poor contractility, tamponade, tension physiology, or severe right ventricular failure. The single rule that resolves these stems is: choose fluid only when underfilling is plausible and congestion risk does not dominate.
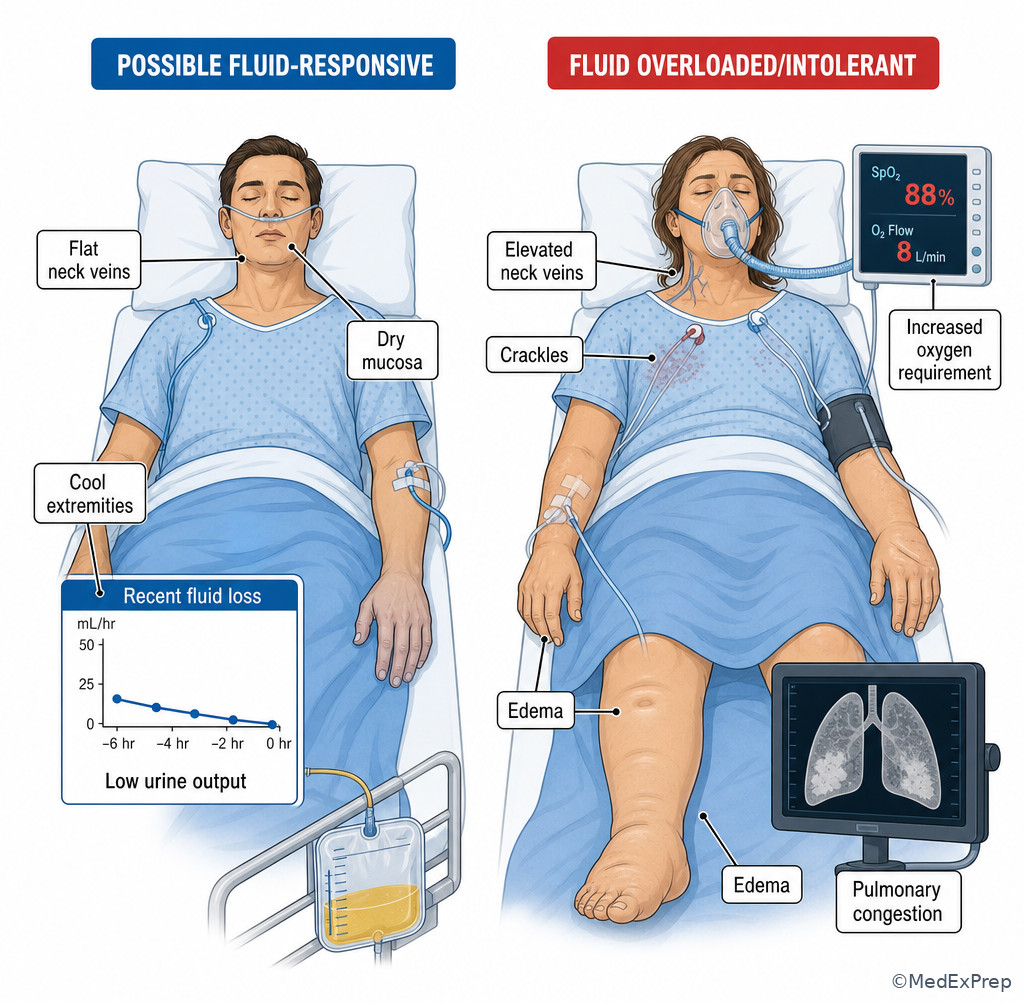
Helpful bedside clues include recent losses, low filling trends, improvement after a small ordered challenge, and absence of worsening respiratory congestion. Clues to reject more fluid include increasing crackles, high oxygen need, frothy sputum, rising PAOP if available, severe ventricular dysfunction, or prior boluses with no perfusion improvement. Dynamic assessments may be used by the team depending on setting and equipment, but for CCRN nursing reasoning, the key is not to overlearn one test and forget the bedside pattern. See Fig 5.
WHY THIS IS TESTED: These are high-stakes patient safety decisions. The exam wants the RN who protects both perfusion and the lungs.
Memory anchor: “Dry helps fluid; wet rejects fluid.” If the dominant picture is dry underfilling without congestion, fluid may help. If the dominant picture is wet lungs and rising oxygen need, more fluid is usually the wrong priority.
Exam takeaway: Choose volume only when underfilling is plausible and pulmonary congestion is not the stronger signal.
flowchart TD
A[Low perfusion or hypotension] --> B{Signs of pulmonary congestion?}
B -->|Yes| C[Reject reflexive fluid]
C --> D[Support oxygenation, reassess, escalate]
B -->|No| E{Recent losses or underfilling clues?}
E -->|Yes| F[Consider ordered fluid trial and monitor response]
E -->|No| G[Look for other causes: afterload, contractility, rhythm, obstruction]
F --> H[Reassess BP, UO, lungs, mentation]
G --> H Exam takeaway: Visual contrast helps separate underfilled shock from worsening pulmonary congestion at the bedside.
Nursing Priority: Assess first: oxygenation, breath sounds, work of breathing, urine output, perfusion, and recent intake/losses. Intervene: if ordered and appropriate, administer volume carefully and monitor response; if congestion dominates, optimize oxygenation and notify the provider. Delegate: transport or basic measurements may be delegated only when the patient is stable; unstable reassessment remains RN-level. Escalate: no response to fluid, worsening respiratory distress, or suspicion that another hemodynamic problem is driving instability.
B Worked example
A 62-year-old man with ischemic cardiomyopathy, prior CABG, and chronic kidney disease is admitted after GI bleeding. He received one unit of packed red blood cells and 500 mL crystalloid. Now BP is 92/60 mm Hg, HR 108/min, urine output 25 mL/hr, skin is cool, lungs are clear, and he is mildly dizzy when turned. Hemoglobin is 7.5 g/dL, but the distractor clue is that he has 2+ chronic pedal edema from baseline heart failure. The nurse must decide whether the hemodynamic pattern still supports possible underfilling.
Identify task: Choose volume-thinking versus overload-thinking.
Extract key facts: Recent blood loss, cool skin, oliguria, clear lungs, and no new oxygen need support underfilling. Chronic edema is noise because it does not define current intravascular status.
Apply rule: A patient can be chronically edematous yet acutely intravascularly depleted.
Eliminate distractors: Reject the assumption that edema means “no more fluid ever.” Also reject waiting passively, because he remains borderline perfused.
Verify: Continued close reassessment for preload response is appropriate, with escalation and ordered treatment based on the larger bleeding/perfusion picture.
C Exam trap
Common wrong answer: “He has edema, so he cannot be underfilled.” WHY IT IS TEMPTING: Candidates equate visible excess fluid with adequate intravascular volume. SINGLE CLUE THAT ELIMINATES IT: Acute blood loss with clear lungs and poor perfusion points to possible intravascular depletion despite chronic extravascular fluid accumulation.
D Checkpoint
Which cue best supports possible preload responsiveness rather than fluid intolerance?
- A. Rising crackles and new pink frothy sputum
- B. Clear lungs, recent fluid loss, low urine output, and cool extremities
- C. Increasing JVD and worsening oxygen saturation after prior bolus
- D. Persistent hypotension with wide warm pulses in early vasodilation
Correct answer: B
- A: Tempting because the patient is unstable; wrong because these are overload/congestion clues.
- B: Tempting because it sounds “too simple”; correct because it is the classic underfilled pattern.
- C: Tempting because pressure is still low; wrong because worsening JVD and oxygenation argue against more fluid.
- D: Tempting because fluids are often given in vasodilation; wrong because the warm vasodilated pattern suggests the pressure problem may not be isolated low preload.
- True or False: A low BP alone proves low preload.
- The bedside pattern “clear lungs + recent losses + oliguria” should make you think ___.
- Name 2 clues that should make you reject another fluid bolus.
1.1.1.7 Integrating preload, output, and perfusion into the RN priority framework
A Explanation
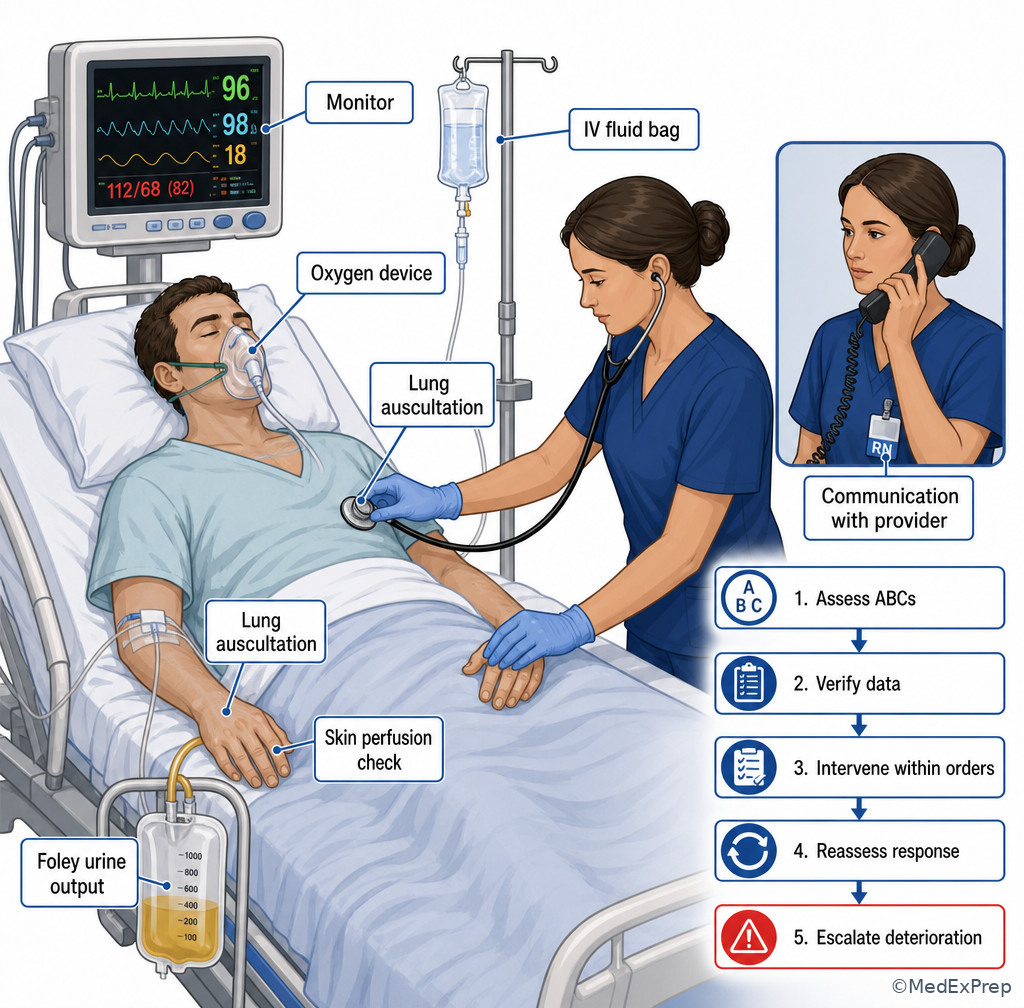
The final integration question is the one CCRN nurses answer constantly: What is my safest next nursing action right now? When low output or low preload is suspected, the RN does not jump into provider-only decisions. Instead, the RN prioritizes ABCs, validates data, identifies whether perfusion is worsening, implements ordered nursing interventions, monitors response, and escalates early. The rule that resolves scope-based questions is: the RN should stabilize, reassess, and communicate the hemodynamic pattern clearly.
For example, if the patient is hypotensive with poor urine output and cool extremities but no congestion, the nursing response may include confirming line accuracy, reviewing fluid balance, assessing for losses or bleeding, giving ordered fluid, and evaluating response. If the patient is hypotensive with crackles and rising oxygen need, breathing support and urgent escalation take priority over more fluid. If the numbers are conflicting, line validation and repeated assessment come before confident interpretation. See Fig 6.
WHY THIS IS TESTED: Many exam distractors are technically reasonable actions, but one is the highest-priority nursing action based on ABCs, scope, and immediate safety.
Recall: In the upcoming topic Afterload, Contractility, And MAP, you will separate low-output states caused by weak pump function or abnormal resistance from true underfilling. Here, your job is to recognize when preload is the likely lever and when it is not.
Exam takeaway: The safest RN answer is the action that protects ABCs, verifies the pattern, and escalates deterioration within scope.
flowchart TD
A[Abnormal BP or poor perfusion] --> B[Assess ABCs and mental status]
B --> C{Respiratory congestion present?}
C -->|Yes| D[Support oxygenation and escalate]
C -->|No| E[Check losses, UO, perfusion, line accuracy]
E --> F{Underfilling likely?}
F -->|Yes| G[Implement ordered volume and reassess]
F -->|No| H[Consider other hemodynamic causes and notify provider]
D --> I[Trend response]
G --> I
H --> I Exam takeaway: Sequence the bedside response as assess, verify, intervene within scope, then evaluate and escalate.
Nursing Priority: Assess first: airway, breathing, circulation, mentation, perfusion, and monitor accuracy. Intervene: implement ordered therapies, position for breathing support if congested, maintain strict I&O, and trend hemodynamic response. Delegate: UAP may obtain routine vitals or assist with comfort measures if stable; focused hemodynamic assessment, patient teaching, and escalation remain with the RN. Escalate: new shock signs, sustained oliguria, lactate rise, worsening respiratory distress, or any unstable pattern beyond nursing-scope correction.
B Worked example
A 69-year-old woman with severe aortic stenosis, hypertension, and chronic diuretic use is one day post valve procedure. She becomes drowsier, BP 82/46 mm Hg, HR 96/min, RR 22/min, SpO2 93% on 2 L, urine output 12 mL over the last hour. Her CVP reading suddenly drops from 8 to 2 mm Hg. A nursing assistant reports the patient “looks sweaty.” A tempting clue is that she also has mild ankle edema. The priority question asks for the most appropriate nursing action.
Identify task: Choose the best next nursing response, not a provider-level definitive treatment plan.
Extract key facts: Hypotension, oliguria, diaphoresis, worsening mentation, possible low filling trend. The edema is chronic noise and does not outweigh the acute pattern.
Apply rule: The RN should first assess ABCs, confirm line validity, check for bleeding or losses, and escalate the unstable change while preparing to implement ordered resuscitation.
Eliminate distractors: Waiting for the next scheduled vitals is unsafe. Delegating the reassessment is unsafe. Independently selecting a vasoactive strategy is outside RN role unless under protocol and order structure.
Verify: The best answer will emphasize immediate reassessment, verification, and escalation within scope.
C Exam trap
Common wrong answer: “Call for a diuretic because the patient has edema.” WHY IT IS TEMPTING: Edema pulls attention toward fluid excess. SINGLE CLUE THAT ELIMINATES IT: The acute instability pattern is hypotension, oliguria, diaphoresis, and decreased alertness — a low-perfusion emergency, not a chronic edema management problem.
D Checkpoint
An adult ICU patient becomes hypotensive and oliguric. The monitor shows a new low filling-pressure trend, but the patient also has mild chronic lower-extremity edema. What is the most appropriate RN interpretation?
- A. Chronic edema proves current preload is excessive, so further reassessment is unnecessary
- B. The acute low-perfusion pattern matters more; reassess and correlate the hemodynamic trend before acting
- C. Ignore the change because edema and low pressure cannot occur together
- D. Immediately choose the definitive vasoactive regimen without provider involvement
Correct answer: B
- A: Tempting because edema looks like obvious volume excess; wrong because chronic edema does not define acute intravascular status.
- B: Tempting because it delays a fast fix; correct because RN priority is reassessment, validation, and correlation with perfusion.
- C: Tempting if you think edema rules out underfilling; wrong because third spacing and intravascular depletion can coexist.
- D: Tempting because the patient is unstable; wrong because choosing the definitive medical regimen is outside RN role unless directed by orders/protocol.
Tables
| Key fact/value | High-yield meaning | Nursing use |
|---|---|---|
| ( CO = HR times SV ) | Flow depends on rate and volume ejected per beat | Explain why tachycardia may help initially but harm filling if excessive |
| Cardiac index | CO adjusted for body size | Prefer this over raw CO when available |
| Urine output < 0.5 mL/kg/hr | Possible poor renal perfusion | Trend with BP, mentation, and lactate |
| CVP | Right-sided filling estimate; limited as a static number | Use as a trend, not a standalone answer |
| PAOP/PCWP | Left-sided filling estimate when measured correctly | Interpret with waveform validity and lung findings |
| Lactate rise | Suggests inadequate tissue perfusion | Does not tell you by itself whether fluid is the right fix |
| Clear lungs after losses | Supports possible underfilling | May support ordered volume with close reassessment |
| Crackles/JVD/rising O2 need | Supports congestion/fluid intolerance | Reject reflexive fluid bolus thinking |
| Comparison point | Low preload / possible fluid responsive | Fluid overloaded / intolerant | Vasodilated but not clearly underfilled |
|---|---|---|---|
| Skin | Cool, pale, clammy often | May be cool if low output; edema may be present | Often warm, flushed early |
| Lungs | Often clear | Crackles, pulmonary congestion | May be clear initially |
| Neck veins | Flat/less full | Distended | Variable |
| Urine output | Low | Low if perfusion poor | Low if shock progresses |
| Response to fluid | May improve if truly underfilled | Minimal perfusion gain; respiratory status worsens | May be limited if vasodilation is dominant |
| Exam priority | Assess losses and trend response | Protect breathing and escalate | Consider afterload/MAP topic linkage |
| Differential pattern | Looks similar because | Single clue that separates it | Safer RN direction |
|---|---|---|---|
| Low preload vs cardiogenic congestion | Both may have low BP and low urine output | Crackles/JVD/S3 point away from more fluid | Support breathing, reassess, escalate |
| Low preload vs distributive vasodilation | Both may be hypotensive | Warm flushed skin and wide pulses suggest vasodilation | Do not assume fluid is the only answer |
| Low preload vs measurement artifact | Sudden filling-pressure change may look dramatic | Waveform/setup inconsistency or transducer error | Validate equipment before acting |
| Low preload vs chronic edema | Visible swelling biases candidates | Acute losses and clear lungs can still mean underfilling | Use current perfusion pattern, not baseline edema |
| Low output from tachyarrhythmia vs low preload | Both can reduce BP and urine output | Rhythm disturbance is the main trigger | Address rhythm/perfusion pattern and escalate |
| Monitoring target | What to track | How often in instability | What improvement looks like |
|---|---|---|---|
| Blood pressure/MAP trend | Direction and consistency, not one reading | Continuous or very frequent per policy | Stabilizing pressure with improved perfusion signs |
| Urine output | Hourly output trend | Hourly | Gradual return toward adequate output |
| Respiratory status | Oxygen need, crackles, work of breathing | Frequent reassessment after fluids | No worsening congestion, improved tolerance |
| Mental status | Agitation, confusion, alertness | Frequent | Improved responsiveness or reduced restlessness |
| Hemodynamic lines | Waveform quality, leveling, trend | At each interpretation point | Valid data that match clinical response |
| Lactate and labs | Trend, not isolated abnormality | Per orders/protocol | Downtrend with better organ perfusion |
Exam Traps & Differentiators
- Most common wrong answer and why: “Hypotension means give fluid.” This is tempting because volume is a familiar response to shock; the single best discriminator is whether congestion or another hemodynamic problem is the stronger pattern.
- Looks similar but isn’t: Chronic edema versus acute adequate preload. Edema reflects total/extravascular fluid burden, not necessarily current intravascular filling.
- If the stem says recent GI loss, bleeding risk, clear lungs, thready pulses, oliguria think possible low preload.
- If the stem says new crackles, rising oxygen need, frothy sputum, JVD after fluids think fluid intolerance or congestion.
- If the stem says invasive value suddenly changed but the bedside picture does not fit think validate line setup and waveform first.
- If the stem says warm flushed skin with low pressure think vasodilation may be dominant; do not assume isolated low preload.
- If the stem says low urine output despite “okay” blood pressure think perfusion may still be inadequate; trend more than the cuff alone.
Exam takeaway: New respiratory compromise after fluids is a key clue that more preload may be unsafe.
Exam takeaway: Third spacing can coexist with poor effective preload, so do not let visible edema mislead you.
Common traps & distractors: The exam often pairs this lesson with upcoming confusion points from Afterload, Contractility, And MAP and Pulmonary Artery Catheter Data. If a stem emphasizes warm vasodilated skin, think beyond preload. If it emphasizes line readings, confirm technical validity before choosing a fluid-based answer.
Algorithm / Approach
Rapid Review
- Cardiac output → minute-to-minute flow; preload is only one contributor.
- Preload → end-diastolic filling/stretch, not total body fluid status.
- Hypotension → insufficient clue by itself; look for lungs, urine output, and skin pattern.
- Oliguria → early perfusion warning even when cuff pressure looks “acceptable.”
- Edema → does not rule out intravascular depletion.
- Crackles after bolus → stronger cue for fluid intolerance than for underfilling.
- Warm wide pulses → think vasodilation before isolated low preload.
- CVP → trend tool, not a standalone verdict.
- PAOP → more useful for left-sided filling, but still must match the clinical picture.
- Tachycardia → may preserve CO briefly, then reduce filling if extreme.
- Clear lungs + recent losses → stronger fluid-responsiveness pattern.
- New oxygen need + JVD → stronger congestion pattern.
- Discordant hemodynamic number → validate waveform and setup first.
- Best RN answer → assess, verify, intervene within orders, reassess, escalate.
Memory anchor: “FLOW asks how much leaves; FILL asks how much enters.” Use this when stems blur cardiac output and preload.
Self-check quiz
1.1.1.8 Question 1
A 63-year-old postoperative ICU patient with hypertension and type 2 diabetes has HR 118/min, BP 90/54 mm Hg, urine output 15 mL/hr, cool extremities, and clear lungs after several hours of high NG output. Which nursing interpretation is most appropriate?
- A. The patient most likely has possible low preload contributing to reduced cardiac output
- B. The patient most likely has fluid overload because blood pressure is low
- C. The patient most likely has adequate preload because oxygen saturation is normal
- D. The patient most likely has a line artifact because tachycardia is present
1.1.1.9 Question 2
A 70-year-old patient with heart failure, chronic kidney disease, and sepsis remains hypotensive after fluids. The nurse notes new bilateral crackles, rising oxygen requirement, and increasing JVD. Which action is the best initial nursing response?
- A. Prepare to give another fluid bolus because urine output is low
- B. Prioritize oxygenation, reassess respiratory status, and notify the provider of likely fluid intolerance
- C. Delay action until the next scheduled chest x-ray confirms pulmonary edema
- D. Delegate the assessment to assistive personnel while reviewing the chart
1.1.1.10 Question 3
A 58-year-old mechanically ventilated patient with pancreatitis, obesity, and high PEEP has BP 88/50 mm Hg, HR 122/min, urine output 12 mL/hr, and lactate 4.0 mmol/L. The CVP is 15 mm Hg. Which nursing action is most appropriate?
- A. Conclude preload is adequate because the CVP is elevated and document the finding
- B. Validate the transducer setup and waveform, compare the CVP with the trend, and correlate with perfusion findings
- C. Ignore the CVP and focus only on urine output because invasive data are unreliable
- D. Independently hold all hemodynamic interventions until a PA catheter is placed
1.1.1.11 Question 4
A 65-year-old man with chronic systolic heart failure and baseline pedal edema is admitted after a GI bleed. He is cool, pale, BP 92/58 mm Hg, HR 110/min, urine output 20 mL/hr, and lungs are clear. Which cue most strongly supports possible intravascular underfilling despite the edema?
- A. Chronic lower-extremity edema
- B. Clear lungs with recent blood loss and poor perfusion findings
- C. History of heart failure
- D. Age older than 60 years
1.1.1.12 Question 5
A 72-year-old patient with pneumonia, atrial fibrillation, and hypertension has BP 84/46 mm Hg, HR 128/min, warm flushed skin, and wide peripheral pulses. Lungs are currently clear, and urine output has begun to fall. Which nursing interpretation is most appropriate?
- A. Isolated low preload is proven, so fluid is the only likely hemodynamic issue
- B. The warm vasodilated pattern suggests another contributor besides preload may be present
- C. Adequate urine output can be assumed because the lungs are clear
- D. The patient is stable because oxygenation is not yet worsening
1.1.1.13 Question 6
A 69-year-old patient one day after cardiac surgery becomes diaphoretic and less responsive. BP is 80/44 mm Hg, HR 104/min, urine output 10 mL/hr, and the CVP appears to drop from 9 to 3 mm Hg. Mild chronic ankle edema is documented from baseline. Which nursing action requires the highest priority?
- A. Ask the UAP to repeat the blood pressure in 30 minutes while the RN finishes another task
- B. Assess ABCs immediately, verify the pressure setup, check for acute losses, and escalate the unstable change
- C. Request a diuretic because baseline edema suggests excess preload
- D. Wait for the surgeon to make rounds before taking further action
1.1.1.14 Question 7
A 61-year-old woman with severe cardiomyopathy, chronic kidney disease, and recent sepsis resuscitation has BP 86/52 mm Hg, HR 118/min, RR 32/min, SpO2 88% on 6 L nasal cannula, diffuse crackles, and urine output 18 mL/hr. Which option is the safest next nursing action?
- A. Administer another rapid fluid bolus because urine output remains low
- B. Increase oxygen support, position to improve breathing, reassess, and urgently notify the provider
- C. Delegate respiratory reassessment to UAP while preparing routine documentation
- D. Focus on hourly weights before addressing the oxygenation problem
1.1.1.15 Question 8
A 55-year-old ICU patient with pancreatitis, third spacing, chronic hypertension, and obesity has rising lactate, BP 90/56 mm Hg, urine output 15 mL/hr, and peripheral edema. Lungs are clear, and the patient has large ongoing abdominal drain losses. Which interpretation best reflects high-level CCRN reasoning?
- A. Peripheral edema rules out low effective preload
- B. Clear lungs plus active fluid losses mean intravascular underfilling may still be present
- C. Rising lactate proves the problem is primarily respiratory
- D. The RN should independently determine the definitive medical management plan
Answer key
1.1.1.16 Question 1 Answer: A
A. Correct. This is tempting because the pattern is classic for volume loss; it is correct because high NG losses, hypotension, tachycardia, oliguria, cool extremities, and clear lungs support possible low preload lowering stroke volume and output. The single stem clue is high NG output with clear lungs. Priority reasoning uses circulation/perfusion first. Sources: AACN adult critical care hemodynamic principles; Lewis Medical-Surgical Nursing; ANA Standards of Practice.
B. Incorrect. This is tempting because low BP may make candidates think “hemodynamic instability equals overload” in complex ICU patients. It is incorrect because nothing suggests congestion; low BP alone does not indicate fluid overload. The discriminating clue is absence of crackles or JVD. Sources: Lewis; NCSBN clinical judgment framework.
C. Incorrect. This is tempting because normal oxygen saturation can falsely reassure. It is incorrect because adequate oxygenation does not prove adequate preload or perfusion. The single clue is urine output 15 mL/hr with cool skin. Sources: Saunders NCLEX review; ANA Standards.
D. Incorrect. This is tempting because tachycardia can accompany monitor artifact or anxiety. It is incorrect because the whole clinical pattern is internally consistent with low perfusion; there is no line-specific clue suggesting artifact. The discriminator is multiple organ perfusion cues, not just one monitor change. Sources: AACN review texts; NCSBN prioritization principles.
1.1.1.17 Question 2 Answer: B
A. Incorrect. This is tempting because low urine output often prompts more fluid. It is incorrect because breathing is now the highest priority; new crackles, JVD, and rising oxygen need indicate likely fluid intolerance. The discriminating clue is new respiratory congestion after fluids. Priority reasoning: ABCs place breathing ahead of further volume. Sources: Lewis; NCSBN prioritization; ANA Standards.
B. Correct. This is tempting because it seems to “delay” circulation treatment, but it is correct because the patient shows pulmonary congestion and hypoxemia. The nurse should support oxygenation, reassess, and escalate the likely adverse response to fluids. The key clue is rising oxygen requirement with crackles. Sources: AACN critical care standards; Lewis.
C. Incorrect. This is tempting because confirmation feels safer. It is incorrect because the patient is unstable now, and nursing action should not wait for scheduled imaging. The discriminator is current bedside deterioration. Sources: NCSBN clinical judgment model; ANA Standards.
D. Incorrect. This is tempting because the RN may want help, but focused respiratory/hemodynamic assessment in an unstable ICU patient cannot be delegated away. The clue is acute instability requiring RN judgment. Sources: ANA delegation standards; NCSBN scope principles.
1.1.1.18 Question 3 Answer: B
A. Incorrect. This is tempting because invasive numbers seem authoritative. It is incorrect because CVP is a limited static marker and may be affected by high PEEP and other factors; documenting and stopping there ignores the unstable patient. The discriminator is ventilation with high PEEP plus hypoperfusion. Sources: AACN hemodynamic monitoring content; Lewis.
B. Correct. This is correct because the safest RN action is to validate the setup, compare trends, and correlate the value with bedside perfusion before deciding what the value means. The single clue is discordance risk from high PEEP and critical illness. Priority reasoning follows assessment before implementation. Sources: AACN; ANA Standards.
C. Incorrect. This is tempting because urine output is clinically important. It is incorrect because throwing away invasive data is as unsafe as overtrusting them; the nurse should integrate, not ignore. The clue is need for trend correlation. Sources: NCSBN judgment framework; Lewis.
D. Incorrect. This is tempting because the patient may eventually need more invasive evaluation. It is incorrect because the RN still must assess, validate current data, and escalate; withholding all action is not safe. The clue is active instability requiring immediate nursing reassessment. Sources: ANA Standards; NCSBN prioritization.
1.1.1.19 Question 4 Answer: B
A. Incorrect. This is tempting because edema visually suggests volume excess. It is incorrect because edema does not define intravascular filling, especially during acute blood loss. The single clue is edema is chronic baseline, not the acute discriminator. Sources: Lewis; AACN hemodynamics review.
B. Correct. This is correct because recent blood loss, clear lungs, and poor perfusion point toward possible intravascular underfilling despite chronic edema. The discriminator is acute loss plus no congestion. Priority reasoning centers on circulation and current pattern recognition. Sources: AACN; NCSBN prioritization.
C. Incorrect. This is tempting because heart failure increases concern for overload. It is incorrect because diagnosis history alone does not outweigh the acute bedside pattern. The clue is current clear lungs and hypoperfusion after bleeding. Sources: Lewis; Saunders.
D. Incorrect. This is tempting only because older adults are higher risk. It is incorrect because age does not discriminate preload state. The clue is specific hemodynamic findings matter more than age. Sources: NCSBN clinical judgment framework.
1.1.1.20 Question 5 Answer: B
A. Incorrect. This is tempting because hypotension and falling urine output often trigger fluid thinking. It is incorrect because the warm flushed skin and wide pulses suggest vasodilation, so preload is not proven to be the only issue. The clue is warm vasodilated pattern. Sources: AACN review; Lewis.
B. Correct. This is correct because the exam wants recognition that vasodilation may be the dominant contributor. The nurse should not assume isolated low preload. The single discriminating clue is warm flushed skin with wide pulses. Priority reasoning uses analysis before intervention. Sources: AACN; NCSBN.
C. Incorrect. This is tempting because clear lungs can falsely reassure. It is incorrect because urine output cannot be assumed; the stem says it is falling. The clue is declining renal perfusion despite clear lungs. Sources: Lewis; ANA Standards.
D. Incorrect. This is tempting because the respiratory picture is not yet severe. It is incorrect because the patient is hypotensive with evolving hypoperfusion and therefore not stable. The clue is falling urine output with low BP. Sources: NCSBN prioritization principles.
1.1.1.21 Question 6 Answer: B
A. Incorrect. This is tempting because repeat vitals are appropriate in stable patients. It is incorrect because the patient is acutely unstable with altered responsiveness and oliguria, so delaying RN assessment violates ABC and safety priorities. The clue is new decreased responsiveness. Sources: NCSBN prioritization; ANA delegation standards.
B. Correct. This is correct because the RN must immediately assess ABCs, verify the hemodynamic data, evaluate for acute causes such as bleeding, and escalate the unstable change. The single stem clue is shock signs plus sudden filling-pressure drop. Sources: AACN hemodynamic monitoring; ANA Standards.
C. Incorrect. This is tempting because edema can bias the nurse toward excess fluid. It is incorrect because the edema is mild and chronic, while the acute pattern suggests low perfusion and possible underfilling or another urgent cause. The clue is acute instability outweighs baseline edema. Sources: Lewis; NCSBN judgment framework.
D. Incorrect. This is tempting because the surgeon should be informed. It is incorrect because waiting without immediate nursing assessment and escalation is unsafe. The clue is time-sensitive hemodynamic deterioration. Sources: ANA Standards; NCSBN.
1.1.1.22 Question 7 Answer: B
A. Incorrect. This is tempting because low urine output suggests poor perfusion and fluids are often considered. It is incorrect because the patient has diffuse crackles and hypoxemia; breathing is the immediate priority, and more fluid may worsen respiratory failure. The discriminator is SpO2 88% with diffuse crackles. Sources: Lewis; NCSBN prioritization.
B. Correct. This is correct because the patient is fluid intolerant or congested, and the RN should support oxygenation, position for breathing, reassess, and urgently notify the provider. The single clue is wet lungs with worsening oxygenation. Priority reasoning: ABCs first. Sources: AACN adult critical care review; ANA Standards.
C. Incorrect. This is tempting because the RN may seek assistance. It is incorrect because respiratory assessment and hemodynamic prioritization in an unstable ICU patient must stay with the RN. The clue is acute breathing compromise. Sources: ANA delegation standards.
D. Incorrect. This is tempting because weights are useful for fluid status. It is incorrect because they are not the priority over immediate oxygenation and escalation. The clue is current respiratory distress. Sources: NCSBN prioritization principles.
1.1.1.23 Question 8 Answer: B
A. Incorrect. This is tempting because peripheral edema is visually compelling. It is incorrect because third spacing and peripheral edema can coexist with low effective circulating volume. The discriminating clue is large ongoing drain losses with clear lungs. Sources: AACN review; Lewis.
B. Correct. This is correct because ongoing losses, clear lungs, low urine output, and rising lactate support the possibility of intravascular underfilling despite edema. The single clue is active losses plus no congestion. Priority reasoning centers on circulation and pattern recognition. Sources: AACN; NCSBN.
C. Incorrect. This is tempting because lactate is associated with severe illness. It is incorrect because lactate suggests hypoperfusion, not specifically a respiratory cause. The clue is lactate is a perfusion marker, not a preload-vs-respiratory diagnosis by itself. Sources: Lewis; Saunders.
D. Incorrect. This is tempting because the case is complex. It is incorrect because the RN does not independently choose the definitive medical plan; the RN assesses, intervenes within scope, and escalates. The clue is scope-of-practice boundary. Sources: ANA Standards; NCSBN scope rules.