Why it matters
- BCPS questions rarely ask whether you can list all problems; they ask which problem is most important to address now.
- In real practice, the best recommendation is often not the most elegant guideline optimization; it is the safest action that prevents imminent harm.
- Polypharmacy cases include deliberate noise: abnormal but stable labs, chronic undertreatment, minor adherence issues, and one true red flag that should move to the top.
- Prioritization is the bridge between assessment and action: without it, pharmacists may recommend correct therapies in the wrong order.
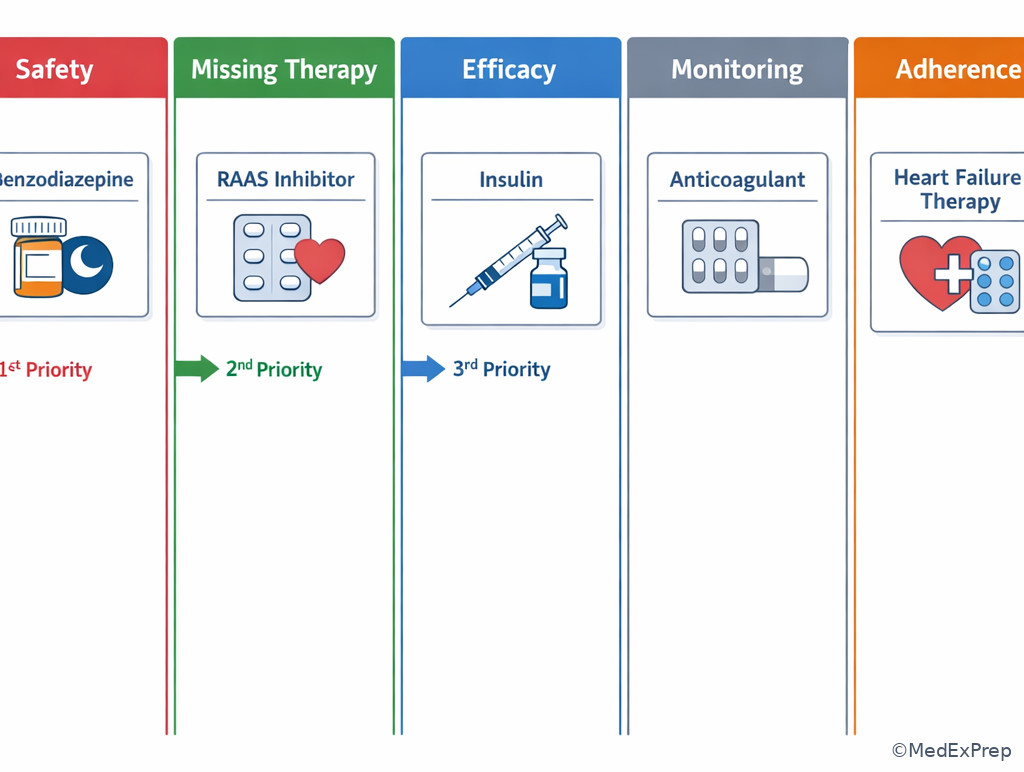
Key rule: When multiple problems are present, rank them in this order unless the stem gives a stronger clue: immediate safety threat, time-sensitive omission, major uncontrolled efficacy issue, monitoring gap, then adherence/convenience optimization.
Key Terms & Must-Know Facts
1.1.1.1 Key terms
- Medication-related problem (MRP): any issue involving indication, efficacy, safety, adherence, or convenience that affects therapeutic outcomes.
- Priority problem: the issue whose correction changes immediate patient risk most.
- Immediacy: how urgently action is needed to prevent harm.
- Severity: the magnitude of likely harm if the problem is not addressed.
- Reversibility: whether prompt action can prevent or limit injury.
- Time-sensitive omission: a needed therapy not given when delay worsens outcomes.
- Contraindication: a patient factor that makes a drug unsafe or unacceptable.
- Monitoring gap: absent or delayed follow-up needed to use a drug safely or effectively.
- Duplicate therapy: unnecessary overlap of agents with similar pharmacologic effect or toxicity.
- Transition discrepancy: mismatch between intended and actual medication list across care settings.
- High-alert medication: a drug with increased risk of significant patient harm when used in error.
- Deprescribing candidate: a medication whose harms, burden, or lack of benefit outweigh current value.
1.1.1.2 Must-know facts
- Safety problems outrank chronic efficacy gaps unless the efficacy gap is itself time-critical.
- Not every abnormal lab is the top priority; the key is whether it changes today's medication risk.
- Drug interaction questions often test whether you recognize a severe interaction before suggesting routine optimization.
- In transitions of care, omission of critical chronic drugs and unintended continuation of acute inpatient drugs are both high-yield.
- Board stems frequently include a tempting guideline-based improvement that should be deferred until a dangerous medication problem is stabilized.
- Monitoring gaps become high priority when the medication has a narrow therapeutic index or current signs of toxicity.
- Adherence matters, but it usually does not outrank active bleeding risk, severe hypoglycemia risk, toxic drug levels, or a contraindicated order.
- Prioritization depends on the patient in front of you, not the drug class in isolation.
| Priority domain | Ask yourself | Usually ranks | Typical examples |
|---|---|---|---|
| Safety | Can this cause serious harm soon? | Highest | Active drug toxicity, contraindicated anticoagulant, duplicate anticoagulation, severe interaction |
| Indication omission | Is a needed therapy missing now? | High if time-sensitive | No VTE prophylaxis when indicated, missed stress-dose steroid in adrenal insufficiency, no antimicrobial coverage in sepsis |
| Efficacy | Is current therapy failing? | Middle to high | Persistent severe hypertension, uncontrolled pain, inadequate empiric antimicrobial regimen |
| Monitoring | Is safe use impossible without follow-up? | Middle | No INR check, absent potassium/SCr after RAAS therapy change, no vancomycin level plan |
| Adherence/convenience | Will regimen complexity reduce success? | Lower unless driving harm now | Cost barrier, duplicate dosing times, inhaler technique issue |
Core content
Exam takeaway: Use urgency plus severity to decide what must be addressed before routine optimization.
flowchart TD
A[Medication list + patient context] --> B{Immediate harm risk?}
B -->|Yes| C[Prioritize safety problem first]
B -->|No| D{Needed therapy missing and time-sensitive?}
D -->|Yes| E[Address omission next]
D -->|No| F{Current therapy ineffective?}
F -->|Yes| G[Optimize efficacy]
F -->|No| H[Close monitoring or adherence gap]
H --> I[Plan follow-up and simplification] See Fig 1 for the core sequence that organizes most prioritization questions.
1.1.1.3 Foundational triage: what makes one medication problem more urgent than another?
A Explanation
The decision conflict is usually choose the problem that can hurt the patient soon versus reject the problem that is important but not urgent. The single rule that resolves the conflict is: prioritize by immediate risk of clinically meaningful harm, not by how incomplete the regimen looks. If a patient has uncontrolled chronic disease and also has a dangerous duplicate therapy, the duplicate therapy comes first. If a patient needs long-term optimization but also has an omitted time-sensitive therapy, the omission may become first priority.
WHY THIS IS TESTED: exam writers want to know whether you can avoid “guideline enthusiasm” when a safety issue should interrupt routine optimization. In complex stems, students often chase A1c, LDL-C, or heart failure intensification while missing a toxic dose, contraindication, or unmonitored high-alert drug.
Use four ranking questions: (1) Will harm occur before the next routine follow-up? (2) How severe is that harm? (3) Is harm preventable if I act now? (4) Is the problem active or only theoretical? Active bleeding risk, severe hypoglycemia risk, marked overanticoagulation, or a dangerous interaction outrank a mildly suboptimal chronic regimen. Stable undertreatment usually follows after urgent safety stabilization.
Memory anchor: Think SOME for ranking: Safety first, Omission if time-sensitive, Monitoring gaps with risk, Efficacy/adherence optimization afterward.
Pharmacist Action: NOTICE high-alert drugs, toxicity clues, contraindications, and rapidly changing labs. SAY “My top concern is the issue most likely to cause preventable harm before the next review.” MONITOR the parameter linked to near-term harm now, then set interval follow-up for lower-priority problems. HOLD/CLARIFY/ESCALATE when a medication poses immediate safety risk or the order conflicts with key patient factors.
B Worked example
A 72-year-old man with atrial fibrillation, stage 3b CKD, type 2 diabetes, and HFrEF is admitted for volume overload. Home medications include apixaban 5 mg twice daily, metformin 1,000 mg twice daily, carvedilol 12.5 mg twice daily, and lisinopril 20 mg daily. The admission team accidentally continues therapeutic enoxaparin 1 mg/kg subcutaneously every 12 hours “for bridge” while apixaban is also continued. His A1c is 8.6%, potassium is 5.0 mEq/L, and SCr is 1.8 mg/dL. The team asks which medication-related problem should be addressed first.
Reasoning chain: Identify task: prioritize the most important problem. Extract key facts: concurrent full-dose apixaban plus therapeutic enoxaparin = duplicate anticoagulation; CKD increases bleeding risk; A1c is elevated but chronic; potassium is only mildly high. Apply rule: immediate safety threat outranks chronic glycemic optimization or future RAAS monitoring. Eliminate distractors: intensifying diabetes therapy is tempting because A1c is abnormal; adjusting lisinopril for potassium is tempting because CKD is present; however, neither poses the same near-term bleed risk as duplicate anticoagulation. Verify: recommend immediate clarification/discontinuation of unintended duplicate therapeutic anticoagulation.
C Exam trap
Common wrong answer: “Address the elevated A1c by adding another antihyperglycemic agent.” WHY IT IS TEMPTING: uncontrolled diabetes is visible, common, and guideline-driven. The SINGLE CLUE that eliminates it: concurrent therapeutic anticoagulants create a present, preventable bleeding hazard that can cause harm before glycemic changes matter.
D Checkpoint
Question: A hospitalized patient with CAD, T2DM, and chronic anemia is receiving aspirin 81 mg daily, clopidogrel 75 mg daily, and newly ordered ibuprofen 800 mg three times daily for pain. Hemoglobin is stable at 10.1 g/dL, A1c is 8.1%, and LDL-C is 94 mg/dL. Which medication-related problem is the highest priority for pharmacist clarification?
- A. Continue current regimen and recommend outpatient A1c reassessment.
Tempting because diabetes is not at goal and may require future action, but wrong because it ignores a same-day bleeding-risk interaction. - B. Clarify high-dose ibuprofen use with dual antiplatelet therapy.
Tempting because NSAIDs plus antiplatelets increase GI and bleeding risk; correct because this is the most immediate preventable safety issue. - C. Recommend high-intensity statin intensification immediately.
Tempting because LDL-C remains above secondary prevention targets, but wrong because lipid optimization is not the most urgent problem in this stem. - D. Start iron supplementation for chronic anemia first.
Tempting because anemia is present and may worsen symptoms, but wrong because stable chronic anemia does not outrank an avoidable bleeding-risk drug combination.
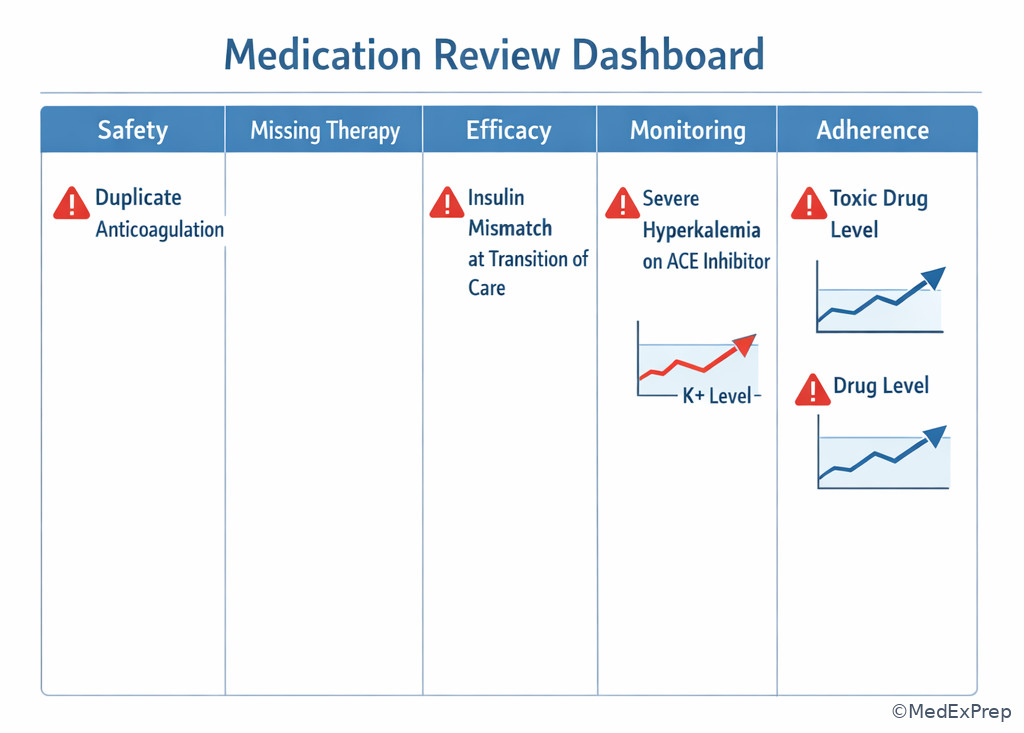
Exam takeaway: Visualize the first-pass screen as a safety-first dashboard rather than a complete guideline checklist.
1.1.1.4 High-risk safety signals: when should toxicity, interactions, and contraindications move to the top?
A Explanation
Now the conflict becomes choose active harm versus reject “potentially important but currently stable” issues. The single finding that resolves this is evidence of current or imminent toxicity: symptoms, critical labs, dangerous combinations, excessive dose for renal/hepatic function, or high-alert medication misuse. A safety issue rises to the top when delay could lead to bleeding, arrhythmia, respiratory depression, severe hypotension, renal failure, hypoglycemia, or other major harm.
WHY THIS IS TESTED: many BCPS stems feature a medication that is appropriate in general but inappropriate in this patient because of one discriminator: renal function, interacting drug, duplication, active adverse effect, or contraindicating comorbidity. The exam tests whether you spot that single variable before choosing a familiar therapy.
High-yield safety categories include: anticoagulation and antiplatelet overlap, insulin/sulfonylurea-induced hypoglycemia risk, QT-prolonging combinations in susceptible patients, nephrotoxic or renally cleared drugs in acute kidney injury, opioid plus benzodiazepine coexposure with oversedation, and drug-disease mismatches such as nonselective beta-blocker in unstable bronchospasm or NSAID in decompensated heart failure/active GI risk. Monitoring matters because some “stable” drugs become urgent once a lab or symptom turns unsafe.
Do not overcall every interaction. The key is clinical consequence now. A theoretical interaction with no short-term harm usually does not outrank a documented toxic concentration or symptomatic adverse effect. See Fig 2 for a safety screening algorithm that compresses this distinction.
Exam takeaway: A current toxicity clue or dangerous interaction makes the safety issue the first action item.
High-Yield Connection: This concept is tested alongside Drug Interaction Management and Adverse Event Assessment. Know both the interaction mechanism and the practical next action; exam stems often pair the two.
Pharmacist Action: NOTICE renal/hepatic mismatch, active adverse-effect symptoms, and dangerous combinations. SAY “This medication may be appropriate in general, but not for this patient at this dose/right now.” MONITOR toxicity markers such as bleeding, glucose, QT risk factors, sedation score, SCr, or drug level at the clinically relevant interval. HOLD/CLARIFY/ESCALATE when a high-alert medication has an unsafe dose, duplication, or contraindication.
B Worked example
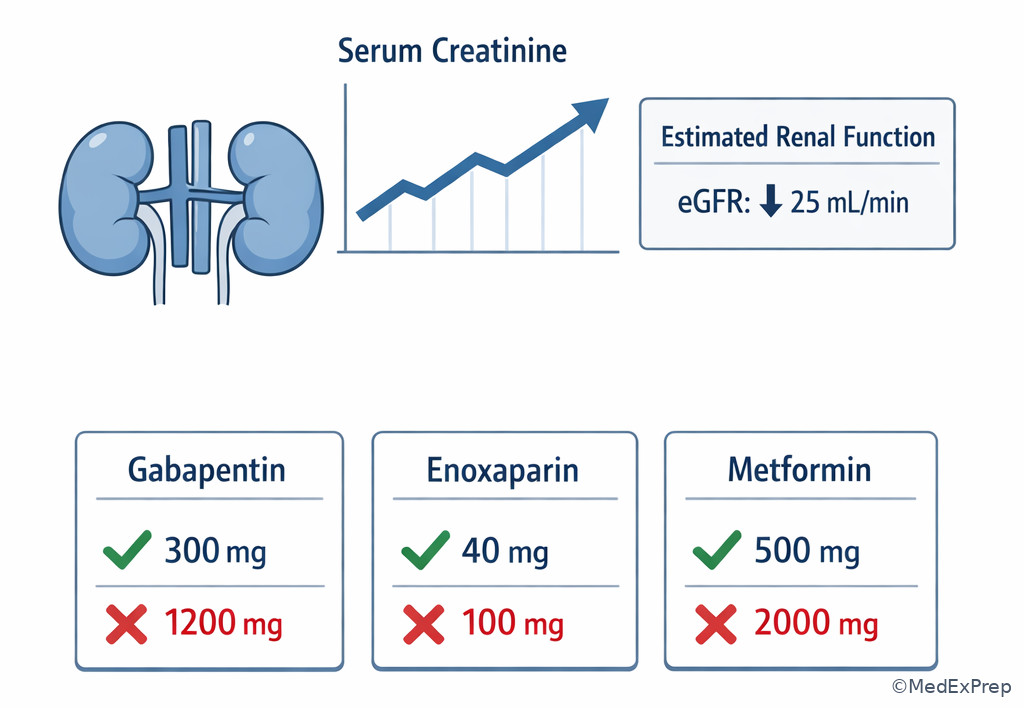
A 66-year-old woman with chronic pain, COPD, CKD stage 4, and insomnia is admitted after a fall. Home medications include oxycodone ER 20 mg twice daily, oxycodone IR 10 mg every 4 hours as needed, gabapentin 600 mg three times daily, and temazepam 30 mg nightly. She is somnolent but arousable, respiratory rate is 10/min, SCr is 2.3 mg/dL, and potassium is 4.4 mEq/L. A distracting clue in the chart notes that her blood pressure remains uncontrolled on amlodipine 5 mg daily.
Reasoning chain: Identify task: highest-priority medication problem. Extract key facts: sedation, low respiratory rate, opioid plus benzodiazepine, renally cleared gabapentin at a likely excessive dose for stage 4 CKD, recent fall. Apply rule: active harm from CNS/respiratory depressants outranks chronic blood pressure optimization. Eliminate distractors: increasing amlodipine is tempting because hypertension is uncontrolled; adjusting insomnia treatment seems secondary but remains part of the same safety cluster. Verify: immediate pharmacist recommendation should focus on oversedation risk—clarify/hold contributing sedatives, assess need for dose reduction and monitoring, and escalate concern promptly.
C Exam trap
Common wrong answer: “Increase antihypertensive therapy because uncontrolled blood pressure increases long-term stroke risk.” WHY IT IS TEMPTING: hypertension is a familiar chronic target with clear guideline thresholds. The SINGLE CLUE that eliminates it: respiratory rate 10/min with somnolence indicates active sedative toxicity, which is a same-day safety problem.
D Checkpoint
Question: Which medication-related problem most warrants immediate pharmacist escalation in a patient receiving warfarin 5 mg daily, trimethoprim-sulfamethoxazole DS twice daily started yesterday, and acetaminophen 650 mg every 6 hours as needed, with an INR now 4.8 but no bleeding?
- A. Continue the regimen and recheck INR in 1 week.
Tempting because there is no overt bleeding, but wrong because the interaction has already produced supratherapeutic anticoagulation that needs prompt action. - B. Escalate the warfarin dose because the antibiotic may reduce gut flora vitamin K production unpredictably.
Tempting only if the interaction is misunderstood; wrong because TMP-SMX typically increases warfarin effect and INR. - C. Clarify the TMP-SMX/warfarin interaction and recommend immediate anticoagulation management adjustment.
Tempting because it directly addresses mechanism and risk; correct because the elevated INR reflects clinically meaningful interaction-related toxicity risk. - D. Prioritize acetaminophen discontinuation alone because it is the main cause of the INR rise at this dose.
Tempting because acetaminophen can influence INR in some patients, but wrong because TMP-SMX is the stronger, more immediate interaction clue in this stem.
- The highest-priority medication problem is usually the one with the greatest risk of preventable near-term harm.
- True or False: A theoretical interaction without current clinical consequence always outranks symptomatic toxicity. False.
- Name 3 high-alert medication categories that frequently rise to the top: anticoagulants, insulin, opioids.
Exam takeaway: Distinguish active drug harm from chronic disease optimization when both appear in the same stem.
flowchart LR
A[Potential issue found] --> B{Active toxicity or critical lab?}
B -->|Yes| C[Safety issue is first]
B -->|No| D{Short delay changes outcome?}
D -->|Yes| E[Time-sensitive omission or efficacy issue]
D -->|No| F[Routine optimization]
F --> G[Adherence simplification and monitoring plan] 1.1.1.5 Indication and omission: when does a missing therapy outrank other problems?
A Explanation
The conflict here is choose a missing therapy now versus reject it because another active problem still comes first. The rule is: a medication omission rises near the top when delay worsens near-term outcomes and there is no more urgent active safety problem preventing initiation. Time-sensitive omission differs from routine optimization. Missing VTE prophylaxis in a high-risk hospitalized patient, omitted antimicrobial coverage in severe infection, or interrupted chronic levetiracetam in a patient with seizure history can be urgent. Missing ezetimibe in a stable outpatient with LDL-C above goal usually is not.
WHY THIS IS TESTED: candidates often under-prioritize omissions because there is no “bad drug” to stop. However, the absence of needed therapy can be as dangerous as an inappropriate drug—especially in acute care, transitions of care, and protocol-driven prevention settings.
To rank omission problems, ask: What is the consequence of waiting? Is the indication confirmed or only possible? Is there a contraindication to starting therapy? Is another issue preventing safe initiation? A missing beta-blocker in stable HFrEF may matter, but it does not outrank life-threatening hyperkalemia. A missing prophylactic anticoagulant in an immobilized patient with active bleeding risk, however, may need rejection because safety changes the recommendation.
Recall: This is the first lesson in the course, so there is no prior topic to review. Build this framework now because upcoming lessons on Functional And Cognitive Assessment and Goals Of Care Alignment will change prioritization when self-management limitations or time-to-benefit considerations are present.
See Fig 3 for a choose-versus-reject algorithm that helps decide when omission becomes the top issue.
Exam takeaway: A missing medication becomes top priority only when the indication is confirmed, time-sensitive, and not blocked by a more urgent safety issue.
Memory anchor: For omissions, use NOW: Need confirmed, Outcome worsens with delay, Without a safety blocker.
Pharmacist Action: NOTICE absent prophylaxis, unintended discontinuation at transition, and missed chronic high-impact therapies. SAY “This patient has a confirmed indication, and delay changes near-term benefit.” MONITOR the outcome marker tied to the omitted therapy, such as clot prevention, seizure recurrence, infection response, or hemodynamic stability. HOLD/CLARIFY/ESCALATE if a contraindication or competing urgent safety issue changes whether initiation is appropriate.
B Worked example
A 58-year-old man with obesity, prior DVT, and metastatic colon cancer is hospitalized with limited mobility for bowel obstruction managed nonoperatively. Home medications include morphine ER 30 mg twice daily, ondansetron 8 mg every 8 hours as needed, and omeprazole 40 mg daily. Platelets are 210,000/mm3, hemoglobin is 11.4 g/dL, SCr is 0.9 mg/dL, and there is no active bleeding. The team asks you to review the profile because his bowel regimen is incomplete and no pharmacologic VTE prophylaxis has been ordered.
Reasoning chain: Identify task: choose the most important problem. Extract key facts: active cancer, prior DVT, immobility, no prophylaxis, no bleeding contraindication. The missing bowel regimen matters, but constipation prevention is not the most dangerous omission here. Apply rule: confirmed, time-sensitive, high-impact omission without blocker rises above comfort-related optimization. Eliminate distractors: adding senna is reasonable; changing ondansetron to reduce constipation is plausible; yet omission of VTE prophylaxis carries more immediate morbidity. Verify: recommend pharmacologic VTE prophylaxis, assuming no institution-specific contraindication.
C Exam trap
Common wrong answer: “Prioritize opioid-induced constipation prevention because the patient already has bowel obstruction risk.” WHY IT IS TEMPTING: the stem foregrounds GI symptoms and opioid use. The SINGLE CLUE that eliminates it: cancer plus immobility plus prior DVT creates a time-sensitive thrombosis prevention need with greater near-term harm potential.
D Checkpoint
Question: A patient with HFrEF, CKD stage 3, and type 2 diabetes is admitted for community-acquired pneumonia. Home empagliflozin and lisinopril were held due to acute illness; ceftriaxone and azithromycin were started appropriately. On day 3, he is hemodynamically stable, eating, and SCr has returned to baseline. Which medication-related problem is now the highest priority?
- A. Restart evidence-based chronic therapy that was unintentionally not resumed once the acute barrier resolved.
Tempting and correct because the omission has become actionable now that the safety blocker has cleared. - B. Increase azithromycin dose to improve atypical coverage.
Tempting because pneumonia treatment is ongoing, but wrong because the regimen is already appropriate and there is no clue of treatment failure. - C. Add a proton pump inhibitor for stress ulcer prophylaxis.
Tempting in hospitalized patients, but wrong because routine prophylaxis is not indicated from the information given and does not outrank resuming needed chronic therapy. - D. Permanently discontinue all renally active chronic medications after any AKI episode.
Tempting because AKI creates caution, but wrong because recovery to baseline changes the risk-benefit balance and blanket discontinuation is not patient-specific.
Exam takeaway: Missing therapy becomes high priority when the indication is clear and the prior safety barrier has resolved.
1.1.1.6 Monitoring gaps and transitions of care: when are missing labs, follow-up, or reconciliation errors the real top problem?
A Explanation
The conflict is choose a missing monitoring or reconciliation step versus reject it because the regimen itself seems acceptable. The rule is: monitoring gaps become high priority when safe use depends on timely data, and transition discrepancies become high priority when they create active risk of omission, duplication, or unintended continuation. A good medication can be a dangerous plan if follow-up is absent.
WHY THIS IS TESTED: BCPS stems frequently hide the main problem in the process rather than the drug choice itself. The medication may be correct, but there is no INR follow-up, no potassium/SCr plan after RAAS intensification, no tacrolimus trough strategy, or no reconciliation after discharge from the ICU. Candidates who focus only on “what drug would you pick?” miss the operational safety failure.
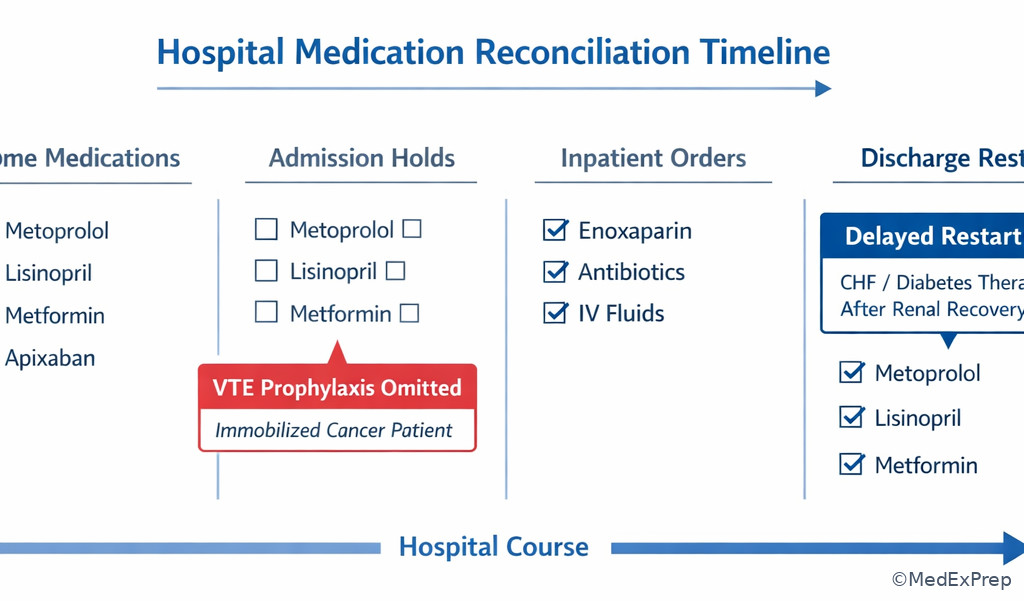
High-priority monitoring examples include warfarin without INR plan, insulin regimen changes without glucose follow-up, diuretic or RAAS changes without renal/electrolyte monitoring in at-risk patients, and TDM drugs without timing strategy. High-priority reconciliation problems include accidental continuation of inpatient-only agents such as VTE prophylaxis or stress-ulcer prophylaxis at discharge, failure to restart essential chronic medicines, and duplications created by formulary substitutions. See Fig 4 for a reconciliation-centered risk screen.
Exam takeaway: Reconciliation errors move to the top when they cause unintended omission, duplication, or unsafe continuation at care transitions.
High-Yield Connection: This concept overlaps with Medication Reconciliation And Optimization and Therapeutic Drug Monitoring Principles. Know how process errors create pharmacotherapy harm even when the drug selection itself looks reasonable.
Pharmacist Action: NOTICE absent follow-up for narrow therapeutic index drugs and mismatches between home and discharge lists. SAY “The regimen is incomplete until the monitoring or reconciliation step is attached.” MONITOR the relevant parameter at the interval the drug requires, not a generic “outpatient follow-up.” HOLD/CLARIFY/ESCALATE when discharge or transfer creates duplication, omission, or continuation of a temporary medication without indication.
B Worked example
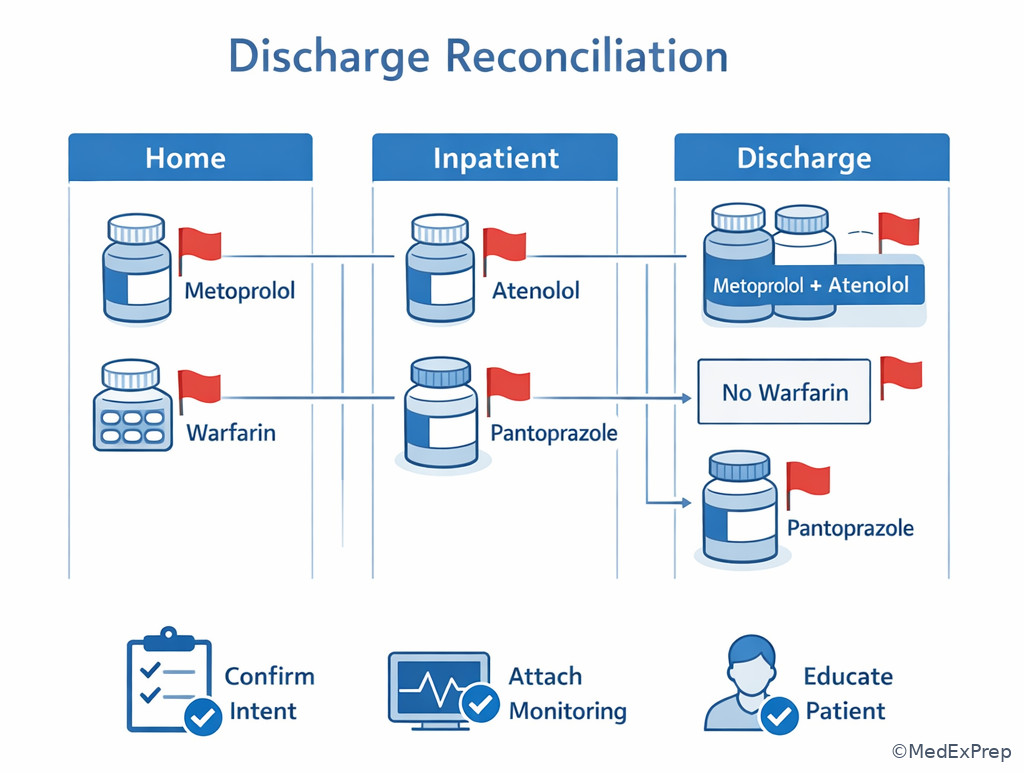
A 70-year-old woman with mechanical mitral valve, CKD stage 3a, osteoarthritis, and GERD is being discharged after treatment for cellulitis. Her discharge medication list includes warfarin 5 mg nightly, cephalexin 500 mg four times daily for 5 days, pantoprazole 40 mg daily, and enoxaparin 40 mg subcutaneously daily “continue until ambulatory.” The discharge summary does not mention an INR follow-up date. She is ambulatory at baseline and has no current VTE prophylaxis indication beyond hospitalization. A distracting note mentions persistent mild edema on exam.
Reasoning chain: Identify task: highest-priority discharge medication problem. Extract key facts: mechanical valve requires therapeutic anticoagulation management; no INR follow-up; enoxaparin prophylaxis continuation may be unintended and duplicative in context; mild edema is not central. Apply rule: transition discrepancy causing anticoagulation risk plus absent monitoring rises above nonurgent symptom management. Eliminate distractors: addressing edema or GERD therapy is lower value. Verify: clarify anticoagulation plan immediately—both unintended continuation of enoxaparin and absent INR follow-up are major discharge safety issues.
C Exam trap
Common wrong answer: “Treat the edema by intensifying diuretic therapy before discharge.” WHY IT IS TEMPTING: discharge stems often invite symptom-based optimization. The SINGLE CLUE that eliminates it: anticoagulation management for a mechanical valve without follow-up and with possible duplicate anticoagulant exposure carries greater immediate risk.
D Checkpoint
Question: Which reconciliation issue is most important to clarify before discharge in a patient whose home regimen included metoprolol succinate 100 mg daily, but the discharge list now includes both metoprolol tartrate 50 mg twice daily and metoprolol succinate 100 mg daily?
- A. Delay discharge until lipid panel results are available.
Tempting because complete data can help future optimization, but wrong because it does not address the active duplication risk. - B. Clarify duplicate beta-blocker therapy created by formulation mismatch.
Tempting and correct because unintended duplication at transition can immediately cause bradycardia or hypotension. - C. Add a calcium channel blocker because blood pressure may remain elevated.
Tempting if hypertension control is imperfect, but wrong because further intensification should not precede fixing a duplicate beta-blocker error. - D. Continue both formulations temporarily for “coverage” until outpatient follow-up.
Tempting because the total daily dose appears familiar, but wrong because two formulations were not intended as combination therapy in this context.
- The most dangerous discharge discrepancy is often duplicate therapy or unintended continuation of a temporary inpatient medication.
- True or False: A correct anticoagulant order without a clear monitoring/follow-up plan can still be a high-priority problem. True.
- Name 3 reconciliation risks: omission, duplication, wrong formulation/strength.
Exam takeaway: Compare home, inpatient, and discharge lists to detect omission, duplication, and temporary-drug carryover.
flowchart TD
A[Home list] --> D[Compare]
B[Inpatient list] --> D
C[Discharge list] --> D
D --> E{Mismatch type}
E --> F[Omission of essential chronic drug]
E --> G[Duplication or formulation mix-up]
E --> H[Continuation of temporary inpatient drug]
F --> I[Correct before discharge]
G --> I
H --> I 1.1.1.7 Integration: a complete ranking framework for polypharmacy and board-style cases
A Explanation
The final conflict is choose the single best next medication-related action in a patient with many legitimate problems. The resolving rule is to combine urgency with expected impact and feasibility: first address what is dangerous now, then what loses benefit if delayed, then what improves long-term outcomes, then what improves execution. This is not just classification; it is sequencing.
WHY THIS IS TESTED: board-style questions are built so that several answers are good ideas. The best answer is the one the pharmacist should act on first, given the current facts. That requires you to resist “comprehensive care mode” and make a single prioritized recommendation.
A useful sequence is: 1) active safety threat; 2) time-sensitive omission; 3) uncontrolled high-impact efficacy problem; 4) monitoring failure with foreseeable harm; 5) adherence/cost/convenience improvements; 6) lower-value preventive fine-tuning. But the stem can invert middle steps. For example, severe uncontrolled pain in a palliative context may outrank long-term statin intensification. Upcoming lessons on Goals Of Care Alignment will modify your ranking when prognosis and burden change the net value of treatment.
When stuck, ask what would make you call the team now rather than leave a note for routine follow-up. That operational instinct often identifies the correct priority. See Fig 5 for the integrated algorithm.
Exam takeaway: In multi-problem cases, choose the recommendation you would escalate now because delay changes harm most.
Common distractor pattern: if one answer would improve long-term guideline concordance and another would prevent imminent harm, the imminent-harm answer is usually correct.
Pharmacist Action: NOTICE which recommendation requires same-day communication versus routine documentation. SAY “I recommend addressing issue X first because it carries the highest near-term risk/benefit impact.” MONITOR the parameter that confirms the first intervention worked, then queue lower-priority optimizations in sequence. HOLD/CLARIFY/ESCALATE whenever the top-ranked issue cannot be safely managed by routine follow-up.
B Worked example
A 76-year-old woman with HFrEF, atrial fibrillation, CKD stage 3, osteoporosis, and mild cognitive impairment is seen after hospital discharge. Medications include furosemide 40 mg daily, sacubitril/valsartan 49/51 mg twice daily, spironolactone 25 mg daily, apixaban 5 mg twice daily, empagliflozin 10 mg daily, amiodarone 200 mg daily, omeprazole 40 mg daily, and zolpidem 10 mg nightly. She also continued clonazepam 0.5 mg twice daily from a prior prescription. BP is 102/64 mm Hg, HR 58 bpm, potassium is 5.6 mEq/L, SCr rose from 1.2 to 1.7 mg/dL, and she reports two recent falls. LDL-C is 84 mg/dL, and her vaccines are not up to date.
Reasoning chain: Identify task: top medication problem. Extract key facts: hyperkalemia and renal worsening on RAAS/MRA therapy; falls with concurrent sedatives; amiodarone plus apixaban creates interaction considerations but not the strongest immediate clue here; vaccines and LDL-C are distractors. Apply rule: active safety threats come first. Between hyperkalemia/AKI risk and sedative-related falls, the stem's objective data point to urgent medication safety review of potassium-raising regimen and renal decline, while also recognizing sedative deprescribing as high priority. Eliminate distractors: vaccine and lipid optimization are valid but lower. Verify: recommend immediate clarification of hyperkalemia/renal deterioration in the heart failure regimen, with rapid follow-up and reassessment of concurrent fall-promoting sedatives.
C Exam trap
Common wrong answer: “Update preventive care first because vaccines are overdue and LDL-C remains above ideal secondary-prevention targets.” WHY IT IS TEMPTING: preventive care gaps are visible and guideline-based. The SINGLE CLUE that eliminates it: potassium 5.6 mEq/L with rising SCr indicates an active safety concern in a high-risk regimen.
D Checkpoint
Question: In a patient with multiple identified MRPs, which principle best selects the first recommendation?
- A. Always address the condition with the most guideline-directed therapies first.
Tempting because guideline intensity feels comprehensive, but wrong because urgency and safety override regimen completeness. - B. Always fix the oldest chronic problem first because it has existed the longest.
Tempting because longstanding problems seem important, but wrong because duration does not equal current risk. - C. Address the problem most likely to cause preventable clinically meaningful harm before the next routine review.
Tempting and correct because it captures urgency, severity, and opportunity for benefit. - D. Start with cost and adherence because these underlie most long-term treatment failure.
Tempting because adherence is foundational, but wrong because it usually follows urgent safety and time-sensitive treatment issues.
Exam takeaway: In complex regimens, the best recommendation is the first justified action, not the longest problem list.
Exam takeaway: Duplicate anticoagulation is a classic immediate-priority problem even when chronic disease targets remain unmet.
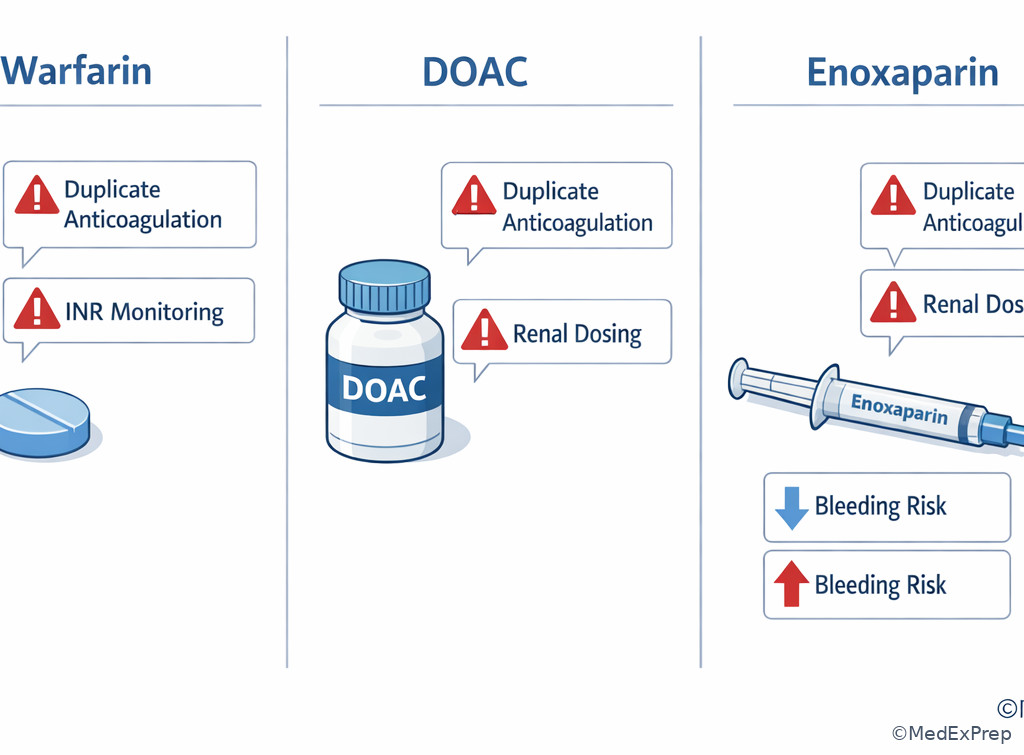
Exam takeaway: Dose appropriateness depends on patient-specific renal function, and the mismatch may outrank routine efficacy optimization.
Exam Traps & Differentiators
Most common wrong answer and why: choosing the chronic disease target that is “not at goal” rather than the active safety issue. This is tempting because guideline targets are easy to recognize; it is wrong because prioritization asks what matters first, not what matters eventually.
| Looks similar | But prioritize this when... | Do not prioritize first when... |
|---|---|---|
| Uncontrolled A1c vs hypoglycemia risk | Hypoglycemia risk or recurrent lows are present | A1c is above goal but there is no acute harm |
| Heart failure optimization vs hyperkalemia on therapy | Potassium/SCr changes create safety concern now | Need for GDMT intensification is chronic and labs are stable |
| Pain control vs oversedation | Respiratory depression, falls, or somnolence is present | Pain remains undertreated but sedative toxicity is absent |
| Preventive therapy gap vs duplicate anticoagulation | Bleeding hazard from overlap exists | Prevention is important but not time-sensitive today |
| Medication cost issue vs omitted VTE prophylaxis | Missed prophylaxis changes inpatient near-term risk | Cost barrier affects outpatient persistence but no same-day danger exists |
If the stem says “somnolent,” “recent falls,” “INR now elevated,” “on both home and bridge anticoagulation,” “no follow-up arranged for warfarin/tacrolimus/vancomycin,” or “drug was held during acute illness and never resumed,” think safety or time-sensitive omission before routine optimization.
- If the stem says duplicate formulations or duplicate class entries, think reconciliation error first.
- If the stem says critical lab after a medication change, think active medication safety problem, not maintenance gap.
- If the stem says indication confirmed + no contraindication + delay worsens outcome, think missing therapy may outrank chronic fine-tuning.
- If the stem says discharge medication list, think omission, duplication, inpatient carryover, and missing monitoring plan.
- If the stem says mildly abnormal chronic value alongside one dangerous interaction, think the interaction is the tested priority.
Recall: In upcoming Functional And Cognitive Assessment, cognitive impairment, caregiver support, and regimen complexity will explain why some adherence problems become higher priority than they first appear. In upcoming Goals Of Care Alignment, prognosis and treatment burden will alter what “best next step” means in frail or palliative patients.
| Stem clue | Tempting wrong move | Single discriminator | Best first focus |
|---|---|---|---|
| INR 4.8 after TMP-SMX | Wait because no bleeding yet | Supratherapeutic INR after major interaction | Immediate anticoagulation safety management |
| A1c 8.5% plus active duplicate anticoagulation | Add diabetes drug | Present bleed risk beats chronic glycemic gap | Stop/clarify duplicate anticoagulation |
| Discharge list contains both metoprolol formulations | Address BP goal first | Transition duplication can cause acute bradycardia | Fix reconciliation mismatch |
| No VTE prophylaxis in immobile cancer patient | Prioritize bowel regimen | Confirmed high-risk omission without blocker | Recommend prophylaxis |
| Somnolence on opioid plus benzodiazepine | Increase antihypertensive for high BP | Respiratory/CNS depression is active harm | Address sedative toxicity risk |
Exam takeaway: Transition stems commonly hide the priority problem in list mismatch rather than disease-state management.
Algorithm / Approach
Exam takeaway: Ask what requires same-day communication; that answer is often the highest-priority recommendation.
flowchart TD
A[Review medication profile] --> B{Need to call now?}
B -->|Yes| C[Safety issue or critical omission]
B -->|No| D{Will waiting worsen outcomes soon?}
D -->|Yes| E[Address high-impact efficacy or monitoring gap]
D -->|No| F[Adherence/cost/convenience optimization]
C --> G[Recommend change + monitoring]
E --> G
F --> G Rapid Review
- Duplicate anticoagulation → immediate bleed-risk clarification beats chronic disease optimization.
- Critical lab after medication change → active safety signal, not routine monitoring trivia.
- Omitted VTE prophylaxis in high-risk immobile adult → time-sensitive missing therapy.
- Discharge list with home and inpatient versions of same class → think reconciliation duplication.
- Somnolence + opioid/benzodiazepine + low respiratory rate → toxicity first, hypertension later.
- Missing INR plan with warfarin → regimen incomplete and unsafe despite correct drug choice.
- Mildly abnormal A1c beside severe interaction → chronic efficacy issue is a distractor.
- Held chronic therapy after AKI that has resolved → omission may become next priority once blocker clears.
- Temporary inpatient drug on discharge list → continuation error until proven intentional.
- Long-term preventive gap → important, but rarely first if a near-term harm signal is present.
- Priority question → ask what would make you contact the team now.
- Monitoring gap on narrow therapeutic index drug → may outrank efficacy fine-tuning.
Memory anchor: CALL NOW = the correct first priority is often the issue that would make you call now, not the one you would document for routine follow-up.
Self-check quiz
1.1.1.8 Question 1
A 69-year-old man with atrial fibrillation, CKD stage 3, and type 2 diabetes is admitted on apixaban 5 mg by mouth twice daily. Admission orders also include enoxaparin 80 mg subcutaneously every 12 hours. His A1c is 8.4%, BP is 146/84 mm Hg, and SCr is 1.7 mg/dL. Which pharmacist recommendation is most appropriate first?
- A. Increase metformin to improve glycemic control
- B. Clarify unintended duplicate therapeutic anticoagulation
- C. Add amlodipine 5 mg daily for blood pressure control
- D. Start high-intensity statin therapy immediately
1.1.1.9 Question 2
A 64-year-old woman taking warfarin 5 mg by mouth nightly for a mechanical valve is prescribed trimethoprim-sulfamethoxazole DS by mouth twice daily for cystitis. Her INR today is 4.9, hemoglobin is stable, and she has no bleeding. Which medication-related problem should be prioritized?
- A. Supratherapeutic anticoagulation from a major interaction
- B. Need for stronger GERD therapy while on antibiotics
- C. Need to intensify blood pressure treatment because stroke risk is high
- D. Need for chronic osteoporosis therapy review
1.1.1.10 Question 3
A 58-year-old man with obesity, metastatic cancer, prior DVT, and normal renal function is hospitalized with limited mobility. He receives morphine ER 30 mg by mouth twice daily, pantoprazole 40 mg daily, and ondansetron 8 mg IV every 8 hours as needed. Platelets are 220,000/mm3, hemoglobin is 11.2 g/dL, and no pharmacologic VTE prophylaxis has been ordered. Which is the most appropriate pharmacist recommendation?
- A. Prioritize a bowel regimen because opioid constipation is predictable
- B. Recommend pharmacologic VTE prophylaxis if no contraindication exists
- C. Add a second antiemetic because ondansetron may be insufficient
- D. Convert pantoprazole to famotidine for cost savings
1.1.1.11 Question 4
A 73-year-old woman with COPD, chronic pain, insomnia, and CKD stage 4 takes oxycodone ER 20 mg by mouth twice daily, gabapentin 600 mg by mouth three times daily, and temazepam 30 mg by mouth nightly. She is somnolent, had a fall overnight, respiratory rate is 10/min, and BP is 158/88 mm Hg. Which medication problem is highest priority?
- A. Uncontrolled blood pressure requiring antihypertensive intensification
- B. Sedative burden with active oversedation risk
- C. Need for sleep optimization because insomnia remains undertreated
- D. Need to add bowel prophylaxis for chronic opioid use
1.1.1.12 Question 5
A 62-year-old man with HFrEF, diabetes, and recent AKI had lisinopril and empagliflozin held on admission. He now completes antibiotic therapy for pneumonia, is eating, BP is stable, potassium is 4.4 mEq/L, and SCr returned to baseline. Current medications are metoprolol succinate 50 mg by mouth daily and furosemide 40 mg by mouth daily. Which issue is now most important?
- A. Restart needed chronic therapies once the acute safety barrier has resolved
- B. Intensify loop diuretic therapy because all HFrEF patients should diurese more
- C. Add a proton pump inhibitor for stress ulcer prophylaxis
- D. Continue holding all renally active drugs indefinitely after any AKI
1.1.1.13 Question 6
A 77-year-old woman with HFrEF, CKD stage 3, atrial fibrillation, and osteoporosis is seen 5 days after discharge. Medications are sacubitril/valsartan 49/51 mg by mouth twice daily, spironolactone 25 mg by mouth daily, furosemide 40 mg by mouth daily, apixaban 5 mg by mouth twice daily, amiodarone 200 mg by mouth daily, zolpidem 10 mg by mouth nightly, and clonazepam 0.5 mg by mouth twice daily. Potassium is 5.7 mEq/L, SCr increased from 1.1 to 1.8 mg/dL, BP is 104/66 mm Hg, and she reports two falls. Which pharmacist concern should be prioritized first?
- A. Hyperkalemia and renal deterioration on the current heart failure regimen
- B. LDL-C remains above ideal secondary prevention targets
- C. Vaccinations are not up to date
- D. Calcium/vitamin D counseling is incomplete
1.1.1.14 Question 7
A 71-year-old man with a mechanical mitral valve, GERD, CKD stage 3a, and osteoarthritis is preparing for discharge. Medications include warfarin 5 mg by mouth nightly, cephalexin 500 mg by mouth four times daily, pantoprazole 40 mg by mouth daily, and enoxaparin 40 mg subcutaneously daily continued from admission. He is ambulatory, has no active bleeding, and no INR follow-up is documented. Which pharmacist action is most appropriate?
- A. Focus first on adding a bowel regimen because antibiotics and immobility increase constipation risk
- B. Clarify the discharge anticoagulation plan and arrange timely INR follow-up
- C. Increase pantoprazole because warfarin increases GI risk
- D. Delay action until the outpatient clinic receives the discharge summary
1.1.1.15 Question 8
A 68-year-old man with CAD, atrial fibrillation, CKD stage 3, and type 2 diabetes is discharged after NSTEMI management. His list includes aspirin 81 mg by mouth daily, clopidogrel 75 mg by mouth daily, apixaban 5 mg by mouth twice daily, ibuprofen 800 mg by mouth three times daily as needed, metoprolol succinate 100 mg by mouth daily, and omeprazole 20 mg by mouth daily. Hemoglobin is 10.4 g/dL and stable, A1c is 8.2%, and BP is 142/86 mm Hg. Which problem most requires immediate clarification?
- A. Persistent hyperglycemia requiring outpatient diabetes intensification
- B. High bleeding-risk analgesic choice in the setting of multiple antithrombotics
- C. Need to intensify antihypertensive therapy before discharge
- D. Need to replace omeprazole with an H2 blocker for convenience
Answer key
1.1.1.16 Question 1: B. Clarify unintended duplicate therapeutic anticoagulation
A. Tempting because A1c 8.4% signals uncontrolled diabetes and chronic optimization is usually appropriate. Incorrect for this scenario because metformin titration does not outrank active duplicate anticoagulation. Single stem clue: apixaban plus treatment-dose enoxaparin. Source: Lexicomp; DiPiro; antithrombotic safety guidance supports avoiding unintended concurrent therapeutic anticoagulants.
B. Tempting because both agents are common in thromboembolic prevention and “bridging” language can sound appropriate. Correct because concurrent full-dose anticoagulants create immediate bleeding risk, especially with CKD. Single stem clue: enoxaparin 80 mg every 12 hours while apixaban continues. Source: Lexicomp; AHFS Drug Information.
C. Tempting because BP 146/84 mm Hg is above goal and amlodipine is a plausible same-class hypertension option. Incorrect because chronic BP management is not the first action when a same-day safety issue is present. Single stem clue: duplicate anticoagulation outranks mildly elevated BP. Source: ACC/AHA hypertension guidance; DiPiro.
D. Tempting because CAD risk reduction commonly includes statin intensification. Incorrect because preventive therapy improvement does not supersede an active medication safety hazard. Single stem clue: immediate bleed risk. Source: cholesterol guidelines; DiPiro.
1.1.1.17 Question 2: A. Supratherapeutic anticoagulation from a major interaction
A. Tempting because INR elevation without bleeding can feel less urgent than visible symptoms. Correct because TMP-SMX markedly potentiates warfarin, and INR 4.9 signals current excess anticoagulation risk needing prompt management. Single stem clue: TMP-SMX started with INR now 4.9. Source: Lexicomp interaction monograph; warfarin management references.
B. Tempting because antibiotics may worsen GI symptoms and PPIs are common. Incorrect because GERD optimization does not affect the main near-term danger. Single stem clue: elevated INR after major interaction. Source: Lexicomp; AHFS.
C. Tempting because valve patients are high-risk for stroke and blood pressure matters long term. Incorrect because hypertension management is lower urgency than interaction-driven overanticoagulation. Single stem clue: current INR toxicity signal. Source: guideline-based chronic risk management principles; DiPiro.
D. Tempting because older adults often need fracture prevention review. Incorrect because this is a longitudinal issue, not the first safety problem. Single stem clue: same-day anticoagulation interaction. Source: osteoporosis guidance; Lexicomp.
1.1.1.18 Question 3: B. Recommend pharmacologic VTE prophylaxis if no contraindication exists
A. Tempting because opioid constipation is predictable and preventable. Incorrect because the omission of VTE prophylaxis in an immobile cancer patient with prior DVT has greater near-term consequence. Single stem clue: cancer + immobility + prior DVT + no prophylaxis. Source: ASH/ACCP thromboprophylaxis guidance; DiPiro.
B. Tempting because prevention questions may be underestimated when no current event has occurred. Correct because this is a confirmed, time-sensitive missing therapy without an evident contraindication. Single stem clue: high-risk inpatient profile and absent prophylaxis. Source: VTE prophylaxis guidelines; AHFS.
C. Tempting because nausea can worsen quality of care and antiemetic escalation is plausible. Incorrect because there is no evidence of uncontrolled emesis, and the omission problem is more consequential. Single stem clue: no prophylactic anticoagulant ordered. Source: supportive care references; DiPiro.
D. Tempting because cost-conscious substitutions are part of pharmacist practice. Incorrect because formulary or cost issues are low priority in this stem. Single stem clue: active prevention gap with high morbidity potential. Source: medication-use systems principles; DiPiro.
1.1.1.19 Question 4: B. Sedative burden with active oversedation risk
A. Tempting because BP 158/88 mm Hg is elevated and antihypertensive intensification seems straightforward. Incorrect because active oversedation with respiratory depression risk is more urgent. Single stem clue: respiratory rate 10/min with somnolence and recent fall. Source: Lexicomp opioid and benzodiazepine warnings; Beers-related geriatric safety principles.
B. Tempting because several agents contribute and the pattern fits a high-risk medication syndrome. Correct because opioid plus benzodiazepine plus likely renally excessive gabapentin in CKD creates immediate CNS/respiratory harm risk. Single stem clue: somnolence, fall, low respiratory rate. Source: FDA boxed warning on opioid/benzodiazepine combination; Lexicomp renal dosing.
C. Tempting because insomnia treatment is part of the regimen. Incorrect because the issue is not undertreated insomnia; it is excessive sedation from treatment. Single stem clue: oversedation, not insomnia. Source: Lexicomp; AHFS.
D. Tempting because opioid bowel prophylaxis is often appropriate. Incorrect because it does not address the problem most likely to cause immediate harm. Single stem clue: low respiratory rate. Source: supportive care references; DiPiro.
1.1.1.20 Question 5: A. Restart needed chronic therapies once the acute safety barrier has resolved
A. Tempting because restart decisions after AKI can feel risky. Correct because the original reason for holding therapy has resolved: hemodynamics stable, eating, potassium acceptable, and SCr back to baseline. Single stem clue: the prior safety barrier is gone. Source: heart failure and diabetes guidance; DiPiro; Clinical Pharmacology/Lexicomp disease-state dosing considerations.
B. Tempting because HFrEF management often includes diuretic assessment. Incorrect because no signs of congestion or diuretic failure are provided, and the more important issue is unintentional persistence of held chronic therapy. Single stem clue: meds held for AKI were never resumed despite recovery. Source: HFrEF guidelines; DiPiro.
C. Tempting because hospitalized patients often accumulate acid suppression. Incorrect because stress ulcer prophylaxis is not the key unmet need here and may itself become unnecessary continuation. Single stem clue: resolved acute illness with missing evidence-based chronic therapy. Source: ASHP stress ulcer prophylaxis principles; DiPiro.
D. Tempting because clinicians fear recurrent kidney injury. Incorrect because indefinite discontinuation of all renally active drugs is not patient-specific and sacrifices benefit once the acute issue resolves. Single stem clue: creatinine returned to baseline. Source: HF/CKD medication optimization principles; DiPiro.
1.1.1.21 Question 6: A. Hyperkalemia and renal deterioration on the current heart failure regimen
A. Tempting because multiple safety concerns exist and this one has objective lab evidence. Correct because potassium 5.7 mEq/L plus creatinine rise on RAAS/MRA therapy represents an active safety issue that may require immediate adjustment and monitoring. Single stem clue: hyperkalemia with worsening renal function. Source: heart failure guideline monitoring recommendations; Lexicomp drug-specific monitoring.
B. Tempting because secondary prevention lipid goals matter in CAD/HFrEF populations. Incorrect because LDL optimization is preventive and not the issue most likely to cause harm before the next routine review. Single stem clue: critical potassium/SCr changes. Source: cholesterol guidelines; DiPiro.
C. Tempting because vaccines reduce morbidity and are often forgotten after discharge. Incorrect because immunization catch-up is not more urgent than lab-defined medication safety risk. Single stem clue: potassium 5.7 mEq/L. Source: immunization guidance; DiPiro.
D. Tempting because osteoporosis prevention is appropriate in an older patient with falls. Incorrect because counseling gaps do not outrank active medication-related hyperkalemia and renal deterioration. Single stem clue: objective current lab abnormality caused or worsened by the regimen. Source: osteoporosis guidance; DiPiro.
1.1.1.22 Question 7: B. Clarify the discharge anticoagulation plan and arrange timely INR follow-up
A. Tempting because discharge bowel regimens are commonly needed. Incorrect because constipation prevention does not outrank anticoagulation errors in a mechanical-valve patient. Single stem clue: enoxaparin continuation plus no INR follow-up. Source: warfarin monitoring references; Lexicomp.
B. Tempting because several smaller discharge issues are present, but this option targets the highest-risk one. Correct because the patient may have unintended ongoing anticoagulant overlap and lacks essential INR follow-up for a narrow therapeutic index drug. Single stem clue: mechanical valve + warfarin + continued enoxaparin + absent INR plan. Source: warfarin management guidance; AHFS; Lexicomp.
C. Tempting because GI protection can matter in anticoagulated patients. Incorrect because acid suppression changes do not address the central discharge safety problem. Single stem clue: anticoagulation process failure, not uncontrolled reflux. Source: GI prophylaxis references; DiPiro.
D. Tempting because some tasks can be handed off to outpatient care. Incorrect because a harmful reconciliation or monitoring error should be corrected before discharge, not deferred. Single stem clue: immediate transition-of-care risk. Source: transitions-of-care medication safety principles; ASHP resources.
1.1.1.23 Question 8: B. High bleeding-risk analgesic choice in the setting of multiple antithrombotics
A. Tempting because A1c 8.2% suggests outpatient diabetes intensification may be appropriate. Incorrect because chronic glycemic optimization does not outrank a same-day high bleeding-risk medication choice. Single stem clue: aspirin + clopidogrel + apixaban + ibuprofen. Source: Lexicomp interaction data; antithrombotic safety principles.
B. Tempting because NSAID prescribing frequently appears in pain management, yet here it is the major safety trap. Correct because ibuprofen adds GI and bleeding risk in a patient already on multiple antithrombotic agents. Single stem clue: concurrent triple antithrombotic exposure with NSAID. Source: Lexicomp; ACC antithrombotic consensus principles; DiPiro.
C. Tempting because BP remains above ideal and post-ACS secondary prevention often requires aggressive risk factor control. Incorrect because hypertension adjustment is not the most urgent issue. Single stem clue: dangerous analgesic/antithrombotic combination. Source: hypertension and ACS secondary prevention guidance.
D. Tempting because PPI selection may matter with antiplatelet therapy. Incorrect because convenience-oriented acid suppression changes do not compare with the immediate bleeding hazard from NSAID use. Single stem clue: ibuprofen on top of multiple antithrombotics. Source: Lexicomp; DiPiro.