Why it matters
- The BCACP exam tests broad ambulatory care competence, so the safest first step is recognizing what type of task the stem is asking before chasing details.
- Many wrong answers look clinically reasonable but belong to a different setting, a different role, or a different blueprint domain.
- A domain-first mental model improves time management: you identify the likely tested skill, then apply the correct guideline or monitoring rule.
- Understanding the public blueprint prevents overstudying obscure content while underpreparing core longitudinal outpatient decisions.
Exam takeaway: Match the stem to a domain first, then choose the ambulatory pharmacist action that best fits.
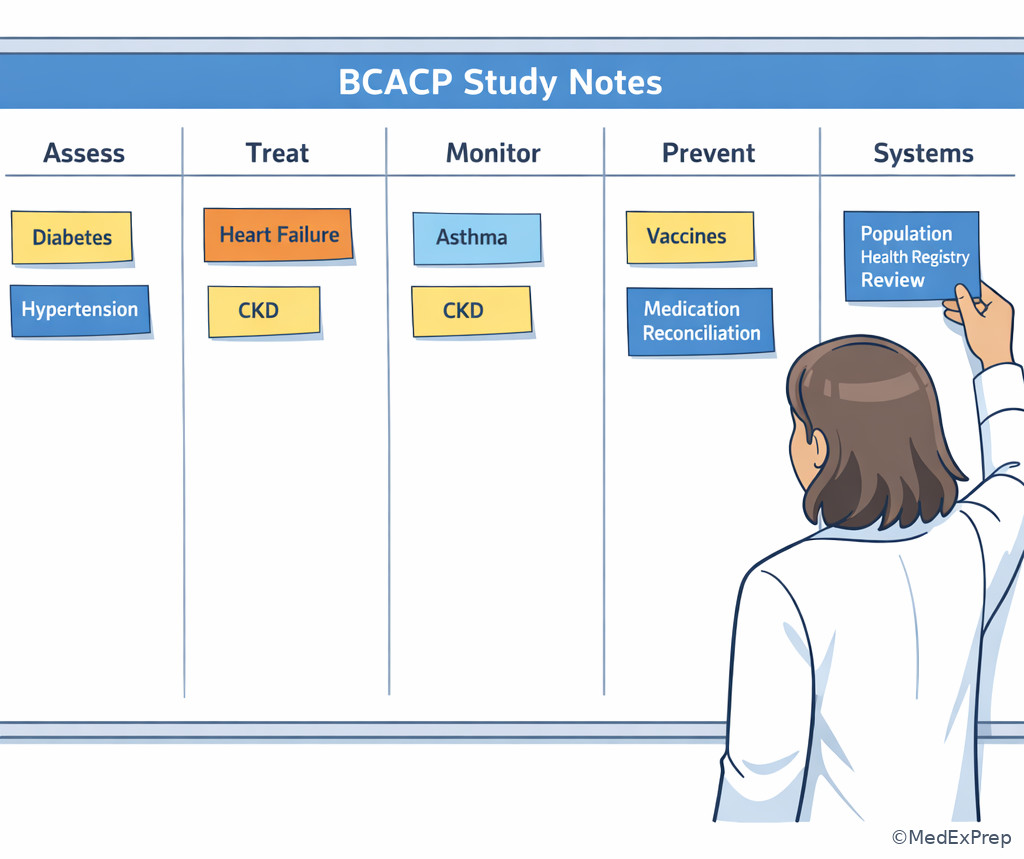
flowchart TD
A[Read stem] --> B{What is being tested?}
B --> C[Medication optimization]
B --> D[Monitoring and follow-up]
B --> E[Preventive care or screening]
B --> F[Transitions or reconciliation]
B --> G[Population health or systems]
C --> H[Choose regimen, dose, safety checks]
D --> H
E --> H
F --> H
G --> H
H[Answer within ambulatory pharmacist scope] Use this frame throughout the lesson. See Fig 1.
Key Terms & Must-Know Facts
1.1.1.1 Key terms
- Blueprint domain: major tested competency area listed in the public BCACP framework
- Subskill: a teachable outpatient task nested under broad blueprint language
- Longitudinal care: ongoing outpatient follow-up rather than one-time acute stabilization
- Medication optimization: initiating, adjusting, simplifying, or stopping therapy to improve outcomes
- Monitoring plan: what to track, when to recheck, and what threshold triggers action
- Transitions of care: medication reconciliation and follow-up after movement between care settings
- Population health: panel-based gap closure, outreach, and quality metric improvement
- Preventive care: immunizations, screening support, risk reduction, and early intervention
- Escalation: referral or collaboration when symptoms, instability, or authority limits exceed pharmacist scope
- Question task: the exact thing the item asks you to decide
- Noise: nonessential details included to distract from the tested rule
- Best next step: the highest-priority ambulatory action for that scenario
1.1.1.2 Must-know facts
- The public blueprint gives broad tested areas; do not invent hidden domain weights or unsupported details.
- BCACP prioritizes outpatient medication management, monitoring, prevention, follow-up, and system-aware decision-making.
- Many stems combine domains; choose the answer based on the primary decision conflict.
- If authority is not explicit, frame actions as recommendations, collaboration, education, follow-up, or escalation.
- In ambulatory care questions, feasibility, adherence, access, safety, and follow-up are often the discriminating clues.
- Outpatient red flags should trigger referral or urgent escalation rather than solo medication tweaking.
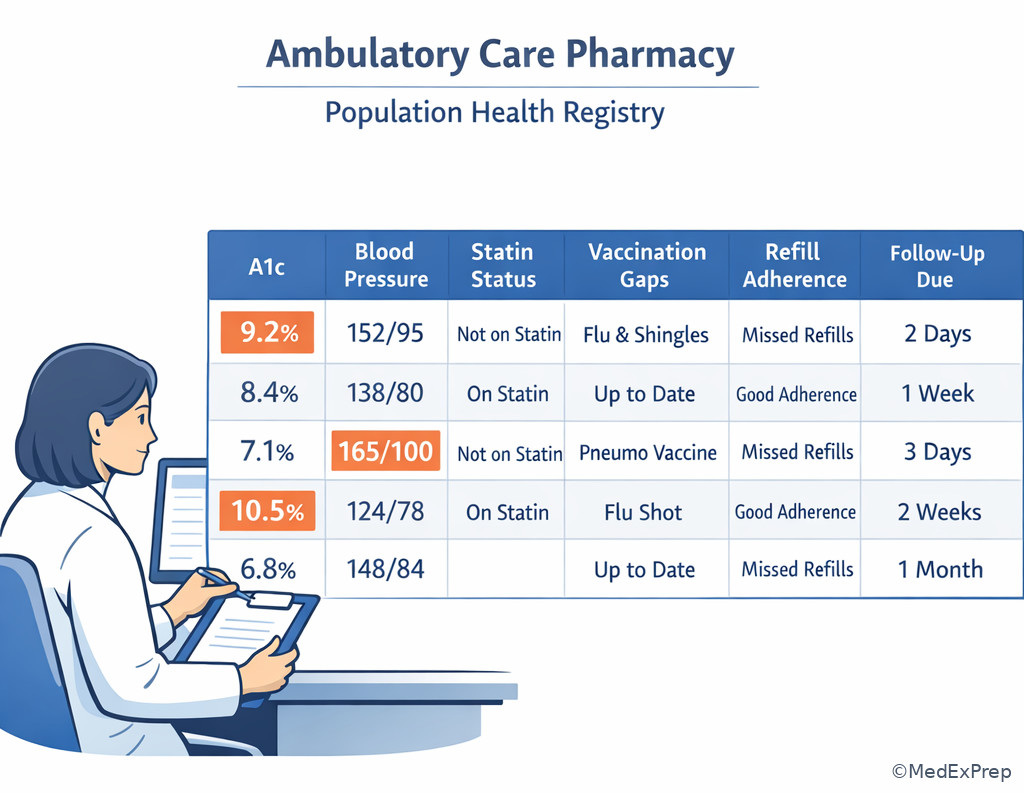
- Quality and population health content commonly appears as care-gap closure, registry review, and panel prioritization.
- Transitions content often tests discrepancy detection, omission, duplication, and unsafe continuation after discharge.
| Blueprint language | What it usually means on exam day | Typical pharmacist task |
|---|---|---|
| Patient assessment | Interpret meds, labs, vitals, risks, barriers | Identify medication-related problems |
| Therapeutic decision-making | Choose or modify drug therapy | Recommend initiation, titration, de-escalation |
| Monitoring and safety | Track efficacy, toxicity, interactions, follow-up | Build monitoring plan and action thresholds |
| Preventive care | Risk reduction and vaccinations | Close preventive care gaps |
| Transitions of care | Post-discharge or cross-setting medication review | Reconcile, clarify, educate, follow up |
| Population health / quality | Panel-level care improvement | Prioritize outreach and metric-based intervention |
Core content
1.1.1.3 Foundational blueprint architecture: what the public domains actually tell you
A Explanation
The first decision conflict is broad framework versus overreading. Students often want a hidden list of exact test percentages or a secret hierarchy of topics. Reject that impulse. The public BCACP blueprint is designed to tell you the major competency categories, not to function as a minute-by-minute prediction tool. Your job is to convert broad labels into ambulatory care pharmacist subskills: medication selection, dose optimization, lab interpretation, preventive care, follow-up timing, reconciliation, adherence strategy, and escalation when the situation exceeds scope.
WHY THIS IS TESTED: exam items are written from broad competency statements, so candidates who can translate blueprint wording into practical outpatient tasks identify the tested rule faster than candidates who memorize isolated facts.
The choose-versus-reject rule here is simple: choose an interpretation anchored in real ambulatory medication-management tasks; reject any interpretation that assumes unpublished blueprint detail or non-ambulatory physician authority. See Fig 2 for a clean summary of how broad domains become study actions.
Exam takeaway: Translate broad blueprint wording into a concrete ambulatory pharmacist task before choosing an answer.
flowchart LR A[Public domain] --> B[Assessment] A --> C[Therapy optimization] A --> D[Monitoring] A --> E[Prevention] A --> F[Systems and population health] B --> G[Extract labs vitals meds risks] C --> H[Choose adjust stop simplify] D --> I[Set follow-up and safety plan] E --> J[Close care gaps] F --> K[Prioritize panel-level action]
B Worked example
A 58-year-old man with type 2 diabetes, hypertension, and obesity comes for an ambulatory pharmacy visit after a health-system quality initiative flagged him for uncontrolled risk factors. Current medications are metformin 1000 mg by mouth twice daily, lisinopril 20 mg by mouth daily, and atorvastatin 20 mg by mouth nightly. His A1c is 8.6%, BP is 146/88 mm Hg, and he reports missing evening doses twice weekly because of shift work. A recent dental infection treated with amoxicillin is noted in the chart. The study question asks which blueprint domain is most directly being activated by this outreach encounter.
Reasoning chain: Identify task: this is not asking for a diagnosis; it asks what competency area the encounter represents. Extract key facts: quality initiative, risk-factor review, medication adherence issue, chronic disease gaps. Apply rule: panel-based outreach and gap closure point to population health/quality, even though disease management details are present. Eliminate distractors: acute infection management is noise; the dental antibiotic is not the tested issue. Verify: the ambulatory pharmacist action is systematic identification and optimization of care gaps at both patient and panel level.
C Exam trap
D Checkpoint
Question: A clinic registry identifies patients with ASCVD who are on moderate-intensity statins despite repeated LDL-C elevation. Which blueprint-oriented task is most directly being tested when the pharmacist reviews the list and recommends therapy intensification?
- A. Population health and medication optimization
- B. Acute stabilization of cardiovascular disease
- C. Independent diagnostic cardiology evaluation
- D. Inpatient formulary stewardship
Option A: tempting because it fits registry review and is correct because the task is panel-based gap closure with outpatient regimen optimization. Option B: tempting because ASCVD sounds high risk, but wrong because no acute instability is described. Option C: tempting because lipid management overlaps with diagnosis and risk assessment, but wrong because the pharmacist is not independently diagnosing cardiac disease. Option D: tempting because formulary and systems work sound operationally similar, but wrong because the scenario is ambulatory registry outreach, not inpatient medication-use policy.
1.1.1.4 Foundational ambulatory scope signals within the blueprint
A Explanation
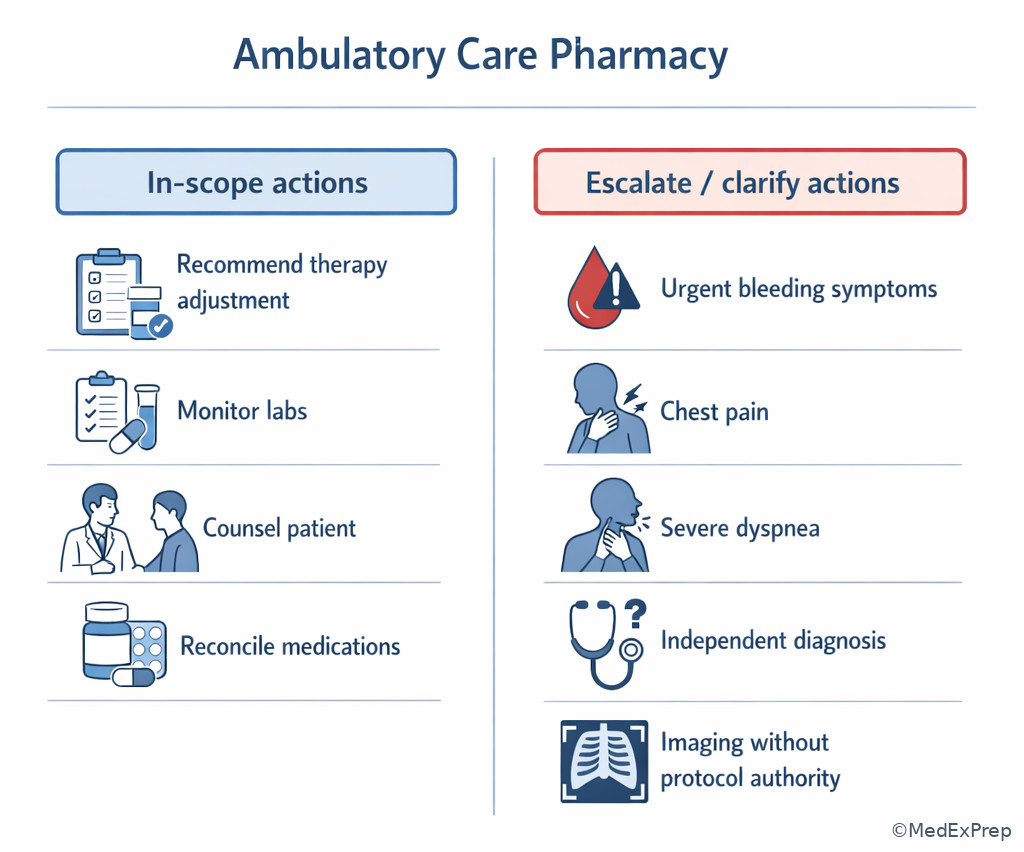
The second decision conflict is ambulatory pharmacist action versus out-of-role action. BCACP candidates are expected to make evidence-based medication recommendations, build monitoring plans, counsel, reconcile medications, and support prevention and quality improvement. They are not expected to act as unrestricted prescribers or attending physicians unless the stem explicitly grants protocol-based authority. This matters because many distractors are not clinically absurd; they are simply mismatched to candidate role.
WHY THIS IS TESTED: the exam wants safe, setting-appropriate decisions. In an outpatient case, the best answer often includes recommendation, collaboration, follow-up interval, documentation, adherence intervention, or escalation for red flags. See Fig 3.
Choose answers framed as medication-management actions within ambulatory workflow. Reject answers that imply independent diagnosis, hospital admission management, procedure ordering without protocol, or emergency attending-level control. Because this is the first lesson in the course, think of this as the prelude to the upcoming topic on Ambulatory Pharmacist Scope Boundaries, where the role lines will be sharpened further.
Exam takeaway: If the stem does not grant authority, select recommendation, monitoring, counseling, or escalation rather than independent prescribing or diagnosis.
flowchart TD
A[Answer choice] --> B{Within ambulatory pharmacist role?}
B -->|Yes| C[Recommend optimize monitor counsel reconcile]
B -->|No| D[Reject]
D --> E[Independent diagnosis]
D --> F[Admit or manage ICU]
D --> G[Order procedures without protocol]
D --> H[Ignore red-flag escalation] B Worked example
A 74-year-old woman with HFpEF, CKD stage 3a, and osteoarthritis calls the ambulatory care clinic two days after discharge. Her discharge list includes furosemide 40 mg by mouth daily, losartan 50 mg by mouth daily, apixaban 5 mg by mouth twice daily, and ibuprofen 600 mg by mouth three times daily as needed that she restarted from home. She reports lightheadedness and black stools. Her husband asks the pharmacist to “just change the blood thinner dose right now.” The stem asks for the most appropriate pharmacist action.
Reasoning chain: Identify task: safe outpatient action within scope. Extract key facts: anticoagulant use, possible GI bleeding, NSAID interaction, post-discharge setting, red-flag symptoms. Apply rule: urgent red flags exceed routine medication optimization; best action is escalation and collaboration, not independent dose change. Eliminate distractors: simply counseling to separate doses or switching to aspirin is unsafe and misses probable bleeding. Verify: ambulatory pharmacist should urgently refer/escalate and communicate the suspected medication-related harm to the care team.
C Exam trap
D Checkpoint
Question: Which answer choice most clearly stays inside the BCACP ambulatory pharmacist role when protocol authority is not stated?
- A. Recommend adding a GLP-1 receptor agonist, document rationale, and arrange follow-up in 4 weeks
- B. Independently diagnose heart failure stage and write the new prescription
- C. Admit the patient directly for uncontrolled blood pressure
- D. Order abdominal CT imaging for unexplained weight loss without protocol authority
Option A: tempting and correct because it reflects recommendation, documentation, and follow-up planning within ambulatory medication management. Option B: tempting because treatment selection often requires staging context, but wrong because the action assumes unrestricted prescriber and diagnostic authority. Option C: tempting because severe disease can require escalation, but wrong because direct admission management exceeds the usual pharmacist candidate role unless explicit systems authority is given. Option D: tempting because weight loss may need workup, but wrong because ordering imaging without protocol authority is out of role.
- True or False: If protocol authority is not stated, “recommend and coordinate follow-up” is usually safer than “independently prescribe.”
- The most common scope error in BCACP stems is confusing ambulatory medication management with acute physician-level management.
- Name 3 in-scope action verbs: recommend, monitor, counsel.
1.1.1.5 Applied domain recognition: how mixed stems hide the primary tested objective
A Explanation
The next decision conflict is multiple true facts versus the primary tested objective. Real ambulatory cases mix adherence problems, lab interpretation, preventive care gaps, cost barriers, and disease-state management in one paragraph. Your job is not to solve every problem at once. Your job is to identify the stem’s main ask. If the question asks for the best monitoring plan, do not choose the most elegant treatment intensification. If it asks for the most appropriate next step after discharge, do not anchor on long-term population-health strategy.
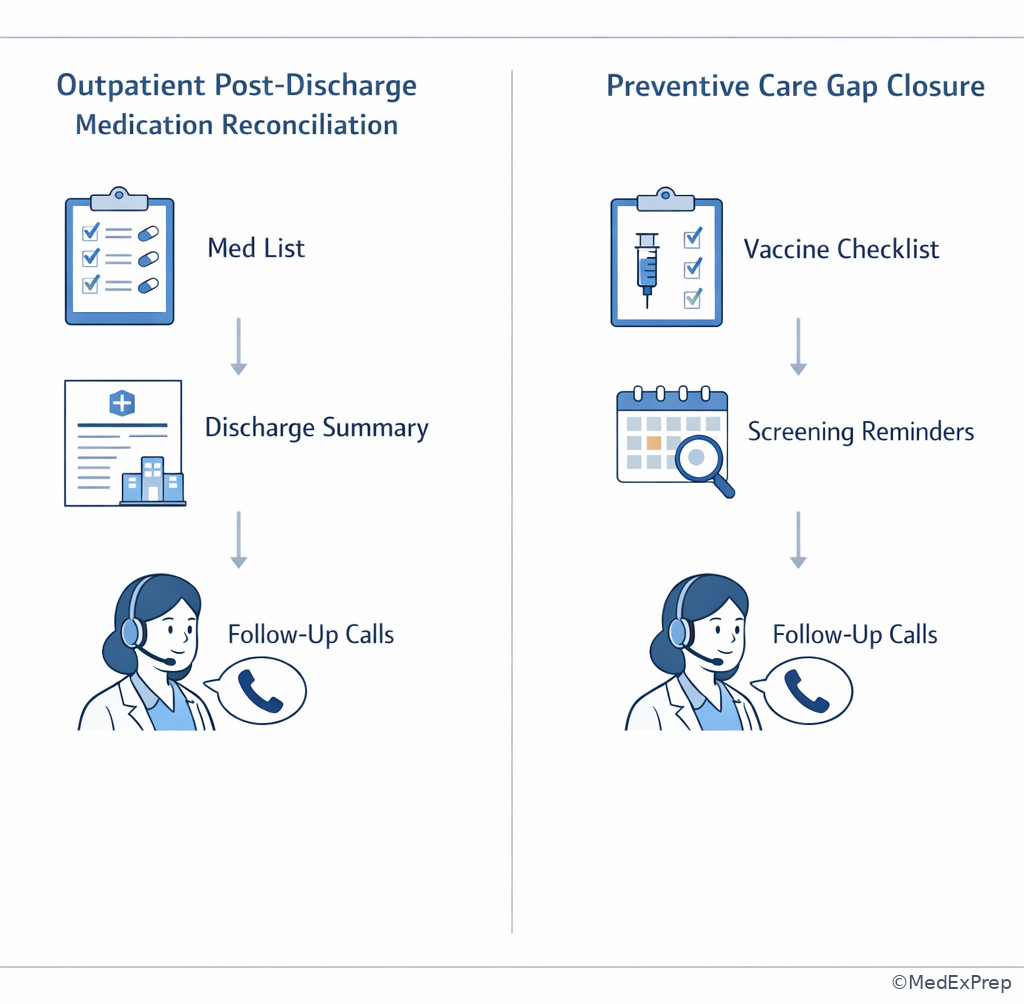
WHY THIS IS TESTED: mixed-domain stems reward prioritization. Test writers add realistic noise so candidates must distinguish the dominant domain from secondary details. See Fig 4.
The resolving rule is: find the action verb in the stem, then match it to the blueprint bucket. “Most important to monitor” points to monitoring/safety. “Best next step after hospitalization” often points to transitions and reconciliation. “Best panel intervention” points to quality/population health. “Best regimen optimization” points to therapeutic decision-making. This is the bridge to the upcoming topic Outpatient Case Decision Framework.
Exam takeaway: The action verb in the question stem determines which domain should drive your answer.
flowchart TD
A[Question stem] --> B{Action verb}
B --> C[Monitor]
B --> D[Optimize regimen]
B --> E[Reconcile after transition]
B --> F[Close preventive gap]
B --> G[Prioritize population action]
C --> H[Monitoring domain]
D --> I[Therapeutic domain]
E --> J[Transitions domain]
F --> K[Preventive care domain]
G --> L[Quality systems domain] B Worked example
A 63-year-old man with HFrEF, type 2 diabetes, and COPD presents for a pharmacist visit 10 days after hospitalization. Medications include carvedilol 12.5 mg by mouth twice daily, sacubitril/valsartan 49/51 mg by mouth twice daily, spironolactone 25 mg by mouth daily, empagliflozin 10 mg by mouth daily, tiotropium inhalation daily, and albuterol as needed. BP is 104/66 mm Hg, serum potassium is 5.3 mEq/L, and he says he has not received the updated discharge medication list from his outside cardiologist. He also asks whether he should get pneumococcal vaccination this year. The item asks for the most appropriate next step in the pharmacist’s post-discharge process.
Reasoning chain: Identify task: post-discharge process, not vaccination, not long-term HF optimization. Extract key facts: recent hospitalization, possible discrepancy, incomplete discharge list, high-risk regimen, potassium elevation. Apply rule: transitions of care domain dominates; medication reconciliation and clarification come first. Eliminate distractors: vaccine review is appropriate but secondary; immediate uptitration of HF therapy is premature until the discharge regimen is confirmed. Verify: the best ambulatory action is to obtain and reconcile discharge medications, clarify discrepancies, and coordinate timely follow-up/monitoring.
C Exam trap
D Checkpoint
Question: A stem asks for the “most important parameter to monitor 1–2 weeks after starting losartan 50 mg by mouth daily in a patient with CKD and hypertension.” Which domain should lead your answer?
- A. Monitoring and safety
- B. Preventive care
- C. Population health
- D. Diagnostic radiology coordination
Option A: tempting and correct because the action verb is monitor and the scenario centers on medication follow-up. Option B: tempting because CKD patients need preventive care too, but wrong because the asked task is short-interval lab monitoring after therapy initiation. Option C: tempting because CKD patients may be managed through panel registries, but wrong because this is an individual follow-up decision. Option D: tempting because CKD workup can involve diagnostics, but wrong because imaging is unrelated to the medication-monitoring ask.
1.1.1.6 Integration across domains: study strategy and question triage for BCACP
A Explanation
The final foundational integration conflict is studying by disease state alone versus studying by blueprint function. Disease-state review is necessary, but BCACP rewards candidates who can also think functionally: assess, optimize, monitor, prevent, reconcile, and manage population care. The highest-yield study plan is dual-coded. For each major ambulatory disease state, ask: What are the common assessment findings? What optimization choices are most tested? What monitoring errors are common? What prevention gaps matter? What transitions issues appear? What population-health metric or care gap is paired with this condition?
WHY THIS IS TESTED: the exam is not just a pharmacology inventory. It tests how an ambulatory care pharmacist uses evidence over time in real outpatient systems. See Fig 5.
Choose a study plan that cross-links diseases to functions. Reject a plan that memorizes drug lists without follow-up strategy, access barriers, or system-level application. This is especially important in ambulatory care because the “best answer” frequently depends on what is feasible to monitor, affordable to obtain, and safe to implement in longitudinal follow-up.
Exam takeaway: Organize each disease state by assessment, therapy, monitoring, prevention, and systems tasks to mirror how BCACP stems are built.
Exam takeaway: Registry-driven care-gap review commonly tests quality improvement and population health skills in ambulatory practice.
B Worked example
A PGY2 ambulatory care resident building a BCACP study schedule plans to spend three weeks memorizing antihyperglycemic drug mechanisms and one day on follow-up, preventive care, and medication reconciliation. Their preceptor asks for the most appropriate blueprint-aligned revision. The resident also mentions that they recently struggled with questions involving payer barriers and post-discharge discrepancies, despite knowing the drug classes well.
Reasoning chain: Identify task: choose the best study strategy based on public domains. Extract key facts: disease-state memorization is strong; systems, follow-up, and transitions are weak. Apply rule: the public blueprint spans more than pharmacology recall. Eliminate distractors: doubling down on memorization of mechanisms alone ignores the actual weakness pattern. Verify: the best revision is to pair each disease state with monitoring, preventive care, access/adherence, transitions, and quality-improvement tasks.
C Exam trap
D Checkpoint
Question: Which study plan best mirrors the public BCACP blueprint?
- A. Review each disease by assessment, regimen selection, monitoring, preventive care, and common ambulatory systems issues
- B. Memorize inpatient guideline algorithms first because they are more detailed
- C. Focus only on rare specialty diseases because they are harder
- D. Study pharmacology mechanisms without follow-up intervals or adherence barriers
Option A: tempting and correct because it reflects the functional structure of the blueprint and ambulatory practice. Option B: tempting because inpatient guidelines can feel more specific, but wrong because BCACP prioritizes outpatient longitudinal care. Option C: tempting because difficulty may feel high yield, but wrong because the public blueprint emphasizes broad ambulatory competencies, not rarity chasing. Option D: tempting because mechanisms are foundational, but wrong because stems often hinge on implementation, safety, and follow-up rather than mechanism alone.
- Fill in the blank: A dual-coded BCACP study plan links each disease state to both content facts and functional ambulatory tasks.
- True or False: If you know the drug class but not the follow-up plan, you are still fully prepared for BCACP mixed stems.
- Name the 5 A-T-M-P-S study buckets.
Exam Traps & Differentiators
Most common wrong answer and why: choosing a clinically true statement that does not answer the actual task. In BCACP stems, several options may be reasonable in general, but only one matches the primary domain, pharmacist scope, and outpatient priority.
| Looks similar | But the stem is really testing | Single discriminator |
|---|---|---|
| Preventive care advice | Transitions of care | Recent discharge, med discrepancies, or pending reconciliation |
| Regimen intensification | Monitoring and safety | Question asks what to monitor or which lab matters next |
| Patient-level disease management | Population health | Registry, dashboard, outreach list, metric gap, or panel review |
| Independent prescribing | Pharmacist recommendation/collaboration | No explicit protocol authority in stem |
| Outpatient management | Urgent escalation | Red flags, instability, bleeding, severe symptoms, or acute deterioration |
| Interesting disease detail | Main action verb | “Best monitoring,” “best next step,” “requires clarification,” or “best outreach” |
If the stem says...
- “Registry,” “outreach,” “panel,” or “quality initiative” → think population health / systems.
- “After discharge,” “med list discrepancy,” or “hospital medication changes” → think transitions of care / reconciliation.
- “Most important to monitor in 1–2 weeks” → think monitoring and safety.
- “No protocol authority stated” → think recommend, collaborate, document, or escalate.
- “Black stools,” “worsening dyspnea at rest,” “confusion,” or “severe symptomatic change” → think urgent escalation beyond routine ambulatory adjustment.
Exam takeaway: Red-flag symptoms and absent authority language should push you toward escalation or recommendation, not independent physician-level action.
Exam takeaway: When discharge discrepancies are present, reconciliation takes priority over routine preventive care tasks.
Related future confusion to anticipate: the upcoming topic Ambulatory Pharmacist Scope Boundaries will make a frequent confusable pair with this lesson. Here you learn blueprint recognition; there you will sharpen role-based answer elimination.
Tables
| Study bucket | Questions it answers | Common outputs |
|---|---|---|
| Assessment | What matters in the profile? | Medication-related problem list |
| Therapy optimization | What should be started, adjusted, or stopped? | Regimen recommendation |
| Monitoring | What should be tracked and when? | Lab/vital/follow-up plan |
| Preventive care | What care gap should be closed? | Vaccine or risk-reduction recommendation |
| Transitions | What discrepancy or safety issue must be clarified? | Reconciled med list and follow-up |
| Population health | Which patients should be prioritized? | Panel outreach plan |
| Common answer framing | Usually acceptable | Usually reject |
|---|---|---|
| Recommend therapy change to prescriber/team | Yes | Only reject if urgent escalation is required first |
| Independently diagnose and prescribe without stated authority | No | Reject as out of role |
| Build monitoring plan with follow-up interval | Yes | Reject only if wrong parameter or unsafe timing |
| Provide counseling and adherence support | Yes | Reject if it ignores a red flag |
| Urgently refer/escalate for instability | Yes when red flags present | Reject if stem is routine and stable |
| Manage inpatient ICU-style treatment | No | Reject as setting mismatch |
| Domain trigger in stem | Primary domain | Common distractor domain | How to choose correctly |
|---|---|---|---|
| “Most appropriate outreach strategy” | Population health | Individual therapy change | Choose panel prioritization logic |
| “Best next step after hospitalization” | Transitions of care | Routine prevention | Reconcile and clarify before routine gap closure |
| “Most important lab to recheck” | Monitoring/safety | Treatment intensification | Follow the monitoring ask, not the treatment urge |
| “Best regimen optimization” | Therapeutic decision-making | Monitoring only | Choose the modification that best fits patient factors |
| “Which action is within scope?” | Role/scope application | Physician-level intervention | Prefer recommendation, counseling, or escalation |
Exam takeaway: Compact domain-to-task cards improve rapid stem triage during timed review.
Algorithm / Approach
Exam takeaway: Identify the task, match the domain, apply scope limits, then choose the safest ambulatory action.
See Fig 6 as your default first-pass method for early BCACP questions.
Rapid Review
- Blueprint domain → broad competency bucket, not hidden exam secrets
- Assessment task → extract meds, labs, vitals, barriers, and risks before answering
- Therapy optimization → choose regimen change only if the stem actually asks for treatment
- Monitoring question → best answer usually includes parameter plus timing
- Transitions stem → recent discharge and med discrepancy outrank routine prevention
- Population health trigger → registry, dashboard, outreach, or care-gap list
- Scope boundary → absent authority language favors recommendation over independent prescribing
- Urgent red flag → escalation beats routine ambulatory fine-tuning
- Noise detail → tempting only if it changes the tested task
- Mixed-domain stem → action verb identifies the primary domain
- Study strategy → pair every disease with A-T-M-P-S, not drug facts alone
- Best answer on BCACP → outpatient-safe, patient-specific, and feasible to follow longitudinally
Self-check quiz
1. A 52-year-old man with hypertension and dyslipidemia is reviewed by an ambulatory care pharmacist after a clinic registry flags overdue follow-up. Current medications are amlodipine 10 mg by mouth daily and rosuvastatin 10 mg by mouth nightly. The question asks which public BCACP domain is most directly reflected by registry review and outreach prioritization. What is the most appropriate answer?
- A. Population health and quality improvement
- B. Emergency cardiovascular stabilization
- C. Independent diagnostic cardiology practice
- D. Inpatient antimicrobial stewardship
2. A 61-year-old woman with type 2 diabetes and CKD stage 3 takes metformin 1000 mg by mouth twice daily and losartan 50 mg by mouth daily. A study stem asks for the “most important parameter to monitor within 1–2 weeks after a medication change.” Which public blueprint bucket should drive the answer?
- A. Monitoring and safety
- B. Preventive care
- C. Population outreach design
- D. Hospital admission triage
3. A 68-year-old man with HFrEF, atrial fibrillation, and CKD stage 3 was discharged 5 days ago. Current medications are apixaban 5 mg by mouth twice daily, sacubitril/valsartan 49/51 mg by mouth twice daily, metoprolol succinate 100 mg by mouth daily, and furosemide 40 mg by mouth daily. He brings two conflicting medication lists and says he restarted ibuprofen 400 mg by mouth three times daily from home. The stem asks for the most appropriate next step in the pharmacist’s process. Which answer is best?
- A. Perform medication reconciliation and clarify discrepancies before routine optimization
- B. Intensify heart failure therapy immediately without reviewing the discharge record
- C. Focus on future vaccine recommendations first
- D. Independently reduce apixaban to 2.5 mg by mouth twice daily
4. A 47-year-old woman with obesity, hypertension, and migraine presents for an ambulatory pharmacy visit. Current medications are hydrochlorothiazide 25 mg by mouth daily and topiramate 50 mg by mouth twice daily. The question asks which study method best aligns with the public BCACP blueprint. Which option is most appropriate?
- A. Study each disease state by assessment, therapy, monitoring, prevention, and system barriers
- B. Memorize drug mechanisms only and defer follow-up plans until the last week
- C. Focus on inpatient order sets because they are more detailed
- D. Ignore transitions and population health because they are less pharmacologic
5. A 72-year-old woman with osteoarthritis, CKD stage 3a, and prior VTE takes rivaroxaban 20 mg by mouth daily, lisinopril 20 mg by mouth daily, and acetaminophen 650 mg by mouth every 8 hours as needed. She calls reporting melena and dizziness after self-starting naproxen 440 mg by mouth twice daily. The stem asks for the most appropriate pharmacist action when authority is not explicitly stated. Which answer is best?
- A. Urgently escalate/referral for possible bleeding and communicate the medication concern
- B. Recommend continuing rivaroxaban and adding a proton pump inhibitor without escalation
- C. Independently reduce rivaroxaban to 10 mg daily
- D. Schedule routine follow-up in 3 months and counsel on NSAID avoidance
6. A 59-year-old man with type 2 diabetes, ASCVD, and obesity takes metformin 1000 mg by mouth twice daily, empagliflozin 25 mg by mouth daily, semaglutide 1 mg subcutaneously weekly, lisinopril 20 mg by mouth daily, and atorvastatin 80 mg by mouth nightly. His clinic uses a dashboard showing overdue retinal exam, missing influenza vaccine, and LDL-C still above goal. The question asks which issue most clearly places the case in a population health domain rather than an individual therapy-only domain. Which option is best?
- A. Use of a dashboard to identify and prioritize care gaps across a panel
- B. Presence of multiple cardiovascular medications
- C. Need for LDL-C intensification in a single patient
- D. Need to counsel on semaglutide adverse effects
7. A 66-year-old woman with COPD, osteoporosis, and hypertension is seen after urgent care treatment for pneumonia. Current medications are tiotropium inhalation daily, albuterol inhalation as needed, prednisone 40 mg by mouth daily for 5 days, amoxicillin/clavulanate 875/125 mg by mouth twice daily for 7 days, and losartan 100 mg by mouth daily. She also asks whether she should receive pneumococcal vaccination now. The stem asks for the best next step after urgent care transition. Which answer is most appropriate?
- A. Reconcile urgent care medications and confirm intended duration before routine preventive interventions
- B. Administer all due vaccines immediately and defer medication review
- C. Independently discontinue losartan because infection is present
- D. Build a long-term osteoporosis treatment plan before reviewing antibiotics
8. A pharmacist candidate is practicing timed questions. One stem includes metformin 1000 mg by mouth twice daily, insulin glargine 30 units subcutaneously nightly, lisinopril 10 mg by mouth daily, A1c 9.1%, blood pressure 128/76 mm Hg, recent discharge after cellulitis, and a note that the discharge summary is missing. The actual question asks for the “most appropriate next step in the ambulatory pharmacist’s process.” Which approach best reflects blueprint-first reasoning?
- A. Identify the question as a transitions task and reconcile medications before intensifying diabetes therapy
- B. Increase insulin glargine immediately because the A1c is above goal
- C. Focus on blood pressure because hypertension is a common BCACP topic
- D. Order wound imaging because cellulitis was the reason for hospitalization
Answer key
1.1.1.7 1. Question 1
Correct answer: A. Population health and quality improvement. PK/PD is not the key issue here; the discriminator is task type. The clinic registry and outreach framing identify panel-based care-gap management, a common ambulatory systems function reflected in the BCACP blueprint. This is consistent with public BCACP competency themes emphasizing longitudinal outpatient quality and medication optimization. Sources: ACCP ambulatory care competencies; DiPiro; ASHP ambulatory care practice resources.
- A: tempting because registry language is a direct clue; correct because dashboard or outreach-list work is classic population health and quality-improvement activity. Single clue: “registry flags overdue follow-up.”
- B: tempting because cardiovascular disease can become urgent, but incorrect because no instability or emergency management is described. Single clue: routine outreach rather than acute symptoms.
- C: tempting because dyslipidemia and hypertension involve risk assessment, but incorrect because the action is not independent diagnosis or specialty evaluation. Single clue: ambulatory pharmacist registry review.
- D: tempting because stewardship is also system-based, but incorrect because the medications and setting do not involve inpatient antibiotics. Single clue: no antimicrobial context.
1.1.1.8 2. Question 2
Correct answer: A. Monitoring and safety. The stem explicitly asks which parameter should be followed after a medication change; that wording makes monitoring the lead domain. Public BCACP framing commonly rewards the candidate who matches the action verb to the domain before interpreting details. Sources: ACCP guidance; DiPiro.
- A: tempting because CKD and medication changes always imply follow-up; correct because the asked task is monitoring. Single clue: “most important parameter to monitor within 1–2 weeks.”
- B: tempting because CKD patients need preventive interventions, but incorrect because prevention is not the immediate ask. Single clue: short-interval recheck language.
- C: tempting because chronic disease can be tracked at panel level, but incorrect because this is one patient’s post-change follow-up. Single clue: individual monitoring window.
- D: tempting because CKD can worsen and require higher-level care, but incorrect because no acute instability or admission decision is presented. Single clue: stable ambulatory follow-up framing.
1.1.1.9 3. Question 3
Correct answer: A. Perform medication reconciliation and clarify discrepancies before routine optimization. Drug-mechanism knowledge is secondary here; the key is transitions of care. The patient has conflicting lists after discharge and a new NSAID interaction risk with apixaban. The safest ambulatory process is to reconcile medications, clarify intended regimens, and then optimize therapy. Sources: ASHP transitions of care guidance; ACCP ambulatory care resources; FDA labeling for apixaban interaction/bleeding risk.
- A: tempting because it may feel slower than direct action; correct because conflicting lists after discharge make reconciliation the highest-priority process step. Single clue: “two conflicting medication lists.”
- B: tempting because HFrEF optimization matters and guideline-directed therapy is high yield, but incorrect because regimen intensification before reconciling the discharge plan is unsafe. Single clue: missing clarity on what the patient should currently be taking.
- C: tempting because vaccines are important in chronic cardiopulmonary disease, but incorrect because preventive care is secondary to transition-related safety risk. Single clue: recent discharge with discrepancies.
- D: tempting because NSAID plus anticoagulant use raises bleeding concern and dose change feels proactive, but incorrect because independent dose reduction is out of role and may not address the true problem. Single clue: no stated protocol authority and need for reconciliation first.
1.1.1.10 4. Question 4
Correct answer: A. Study each disease state by assessment, therapy, monitoring, prevention, and system barriers. This mirrors the public blueprint and the A-T-M-P-S framework taught in the lesson. BCACP preparation is strongest when disease content is linked to ambulatory tasks and follow-up implementation. Sources: ACCP/ASHP ambulatory care competencies; DiPiro.
- A: tempting because it is broader and more work; correct because it matches how mixed-domain ambulatory stems are written. Single clue: the public blueprint is functional, not mechanism-only.
- B: tempting because mechanisms feel foundational, but incorrect because mechanism knowledge alone misses follow-up, access, safety, and systems tasks. Single clue: blueprint breadth beyond pharmacology recall.
- C: tempting because inpatient algorithms are detailed, but incorrect because BCACP emphasizes longitudinal outpatient care. Single clue: ambulatory scope and setting.
- D: tempting because transitions and population health may feel less “drug-focused,” but incorrect because they remain explicitly relevant ambulatory competencies. Single clue: post-discharge and care-gap processes are exam-relevant.
1.1.1.11 5. Question 5
Correct answer: A. Urgently escalate/referral for possible bleeding and communicate the medication concern. Pharmacologically, rivaroxaban plus naproxen increases bleeding risk; melena and dizziness are red flags that move the case out of routine ambulatory adjustment and into urgent escalation. Guideline-concordant pharmacist action is to recognize probable medication-related harm, instruct urgent evaluation, and communicate with the care team. Sources: FDA rivaroxaban labeling; Lexicomp; ASHP ambulatory care guidance.
- A: tempting because escalation can feel less “pharmacy-specific,” but correct because it is the safest in-scope action in a suspected anticoagulant-related bleed. Single clue: melena and dizziness.
- B: tempting because GI protection sounds helpful, but incorrect because adding a PPI without escalation delays evaluation of a potential active bleed. Single clue: red-flag symptoms already present.
- C: tempting because lower anticoagulant dose seems safer, but incorrect because dose reduction is not the right response to suspected active bleeding and assumes authority not granted. Single clue: urgent safety issue, not maintenance dosing question.
- D: tempting because NSAID counseling is appropriate, but incorrect because routine follow-up misses immediate harm. Single clue: symptomatic possible bleed requiring urgent action.
1.1.1.12 6. Question 6
Correct answer: A. Use of a dashboard to identify and prioritize care gaps across a panel. The domain discriminator is not the medications themselves but the workflow structure. A dashboard or registry indicates population-health operations rather than a purely individual therapy question. Sources: ACCP ambulatory care framework; ASHP ambulatory care practice standards.
- A: tempting because dashboards are a systems clue; correct because panel identification and prioritization are defining population-health functions. Single clue: “clinic uses a dashboard showing care gaps.”
- B: tempting because multiple cardiometabolic drugs imply complex management, but incorrect because polytherapy alone does not define population health. Single clue: system-level dashboard language matters more.
- C: tempting because LDL-C intensification is high yield, but incorrect because it describes an individual treatment task rather than the specific domain shift being asked. Single clue: panel-based prioritization.
- D: tempting because counseling is pharmacist work, but incorrect because counseling is patient-level care, not the domain cue asked here. Single clue: registry workflow rather than encounter counseling.
1.1.1.13 7. Question 7
Correct answer: A. Reconcile urgent care medications and confirm intended duration before routine preventive interventions. Pharmacologically, prednisone and amoxicillin/clavulanate are short-course transition medications where duration errors are common. The stem asks for the best next step after an urgent care transition, making reconciliation primary and vaccination secondary. Sources: ASHP transitions guidance; Lexicomp; DiPiro.
- A: tempting because it delays prevention briefly; correct because transition safety takes priority when new short-course therapies and cross-setting communication are involved. Single clue: “after urgent care transition.”
- B: tempting because COPD and older age increase vaccine importance, but incorrect because preventive care does not outrank unresolved transition medication issues. Single clue: current urgent care medication changes require confirmation first.
- C: tempting because clinicians may think about holding certain chronic drugs during illness, but incorrect because independent discontinuation is out of role and not the primary task. Single clue: no authority stated and no losartan-specific emergency provided.
- D: tempting because osteoporosis matters in a patient receiving steroids, but incorrect because long-term bone management is not the next step after urgent care treatment. Single clue: immediate transition process question.
1.1.1.14 8. Question 8
Correct answer: A. Identify the question as a transitions task and reconcile medications before intensifying diabetes therapy. The missing discharge summary is the pivotal clue. Although the A1c is above goal and insulin titration may eventually be needed, the blueprint-first approach prioritizes the explicit post-discharge process task. Sources: ASHP transitions of care guidance; ACCP ambulatory care competencies; DiPiro.
- A: tempting because it may feel process-heavy, but correct because the stem asks for the most appropriate next step in ambulatory pharmacist workflow after discharge. Single clue: “recent discharge” plus “discharge summary is missing.”
- B: tempting because A1c 9.1% suggests uncontrolled diabetes and insulin titration is a common pharmacist action, but incorrect because therapy intensification should wait until the transition record is clarified. Single clue: missing discharge information.
- C: tempting because hypertension is common on BCACP and the blood pressure is provided, but incorrect because BP is already controlled and is not the task driver. Single clue: the BP value is distractor noise.
- D: tempting because hospitalization for cellulitis may have involved ongoing infection concerns, but incorrect because imaging without protocol authority is out of role and not the main ambulatory process need. Single clue: pharmacist-scope next-step framing.