Why it matters
- Many Step 2 CK questions are not really asking for the diagnosis first; they are asking whether the patient is too unstable to wait.
- ABCs determine the order of actions across trauma, sepsis, overdose, respiratory failure, GI bleed, anaphylaxis, obstetric emergencies, and pediatric illness.
- The most common exam error is choosing a “good test” or a “correct diagnosis” before treating an immediately life-threatening physiology problem.
- This topic is the foundation for upcoming lessons on shock and sepsis; if you miss acuity recognition, you will miss the management question even if you know the disease.
Key Terms & Must-Know Facts
1.1.1.1 Key terms
- Acuity: how immediately dangerous the patient's current condition is
- ABCs: airway, breathing, circulation
- Primary survey: rapid first-pass evaluation for life threats
- Airway compromise: inability to protect or maintain a patent airway
- Respiratory failure: inadequate oxygenation and/or ventilation
- Hypoxemia: low arterial oxygen level
- Ventilation failure: inadequate carbon dioxide elimination
- Perfusion: effective blood flow to organs
- Hemodynamic instability: poor circulation causing organ hypoperfusion
- Altered mental status: a red flag for hypoxia, hypoperfusion, toxin, metabolic derangement, or CNS event
- Rapid response activation: urgent escalation for deterioration before arrest
- Definitive airway: secured airway, usually endotracheal tube
- Bag-mask ventilation: temporizing support when breathing is inadequate
- Supplemental oxygen: immediate support for hypoxemia, not a substitute for airway control
- Resuscitation: immediate interventions to restore oxygen delivery and perfusion
1.1.1.2 Must-know facts
- On Step 2 CK, stabilize before you characterize.
- Stridor, gurgling, inability to handle secretions, and worsening mental status all threaten the airway.
- Tachypnea can be compensatory; bradypnea or shallow breathing is more ominous for ventilatory failure.
- Normal pulse oximetry does not exclude impending respiratory exhaustion.
- Hypotension is late; cool clammy skin, confusion, oliguria, and delayed capillary refill may show shock earlier.
- If a patient is pulseless or apneic, transition from ABC assessment to resuscitation protocol immediately.
- Two large-bore IVs are standard early circulation access in unstable adults.
- Do not send an unstable patient to CT before bedside stabilization.
- Airway problems kill faster than diagnostic uncertainty.
- Upcoming topics on shock and sepsis build on the same first move: recognize unstable physiology fast.
| Domain | Immediate bedside clue | What it means on exam day | Most appropriate next step |
|---|---|---|---|
| Airway | Stridor, gurgling, drooling, facial trauma, cannot speak full sentence | Threatened airway | Call for airway support; prepare definitive airway |
| Breathing | Cyanosis, severe work of breathing, silent chest, bradypnea | Impending respiratory failure | Oxygen, ventilation support, identify reversible cause |
| Circulation | Hypotension, cool extremities, weak pulses, confusion | Shock until proven otherwise | IV access, fluids or blood as indicated, monitor closely |
| Disability | Acute change in mental status, unresponsiveness, seizure | Possible hypoxia, hypoperfusion, glucose/toxin/CNS emergency | Check glucose; treat life threats while evaluating |
| Exposure | Rash, bleeding, trauma, burns, temperature extremes | Cause may be visible only after exposure | Fully expose while preventing hypothermia |
Core content
1.1.1.3 Foundational triage: is the patient sick or not sick?
A Explanation
The first exam decision is not “What is the diagnosis?” but “Is this patient unstable enough that stabilization comes before diagnostic precision?” The decision conflict is workup now versus resuscitate now. The single rule that resolves it: if there is evidence of threatened airway, inadequate breathing, poor perfusion, or rapidly worsening mental status, you stabilize first.
WHY THIS IS TESTED: board stems often include enough diagnostic detail to tempt you into choosing CT, cultures, bronchodilators, antibiotics, or specialty consultation before first addressing a failing airway or collapsing circulation.
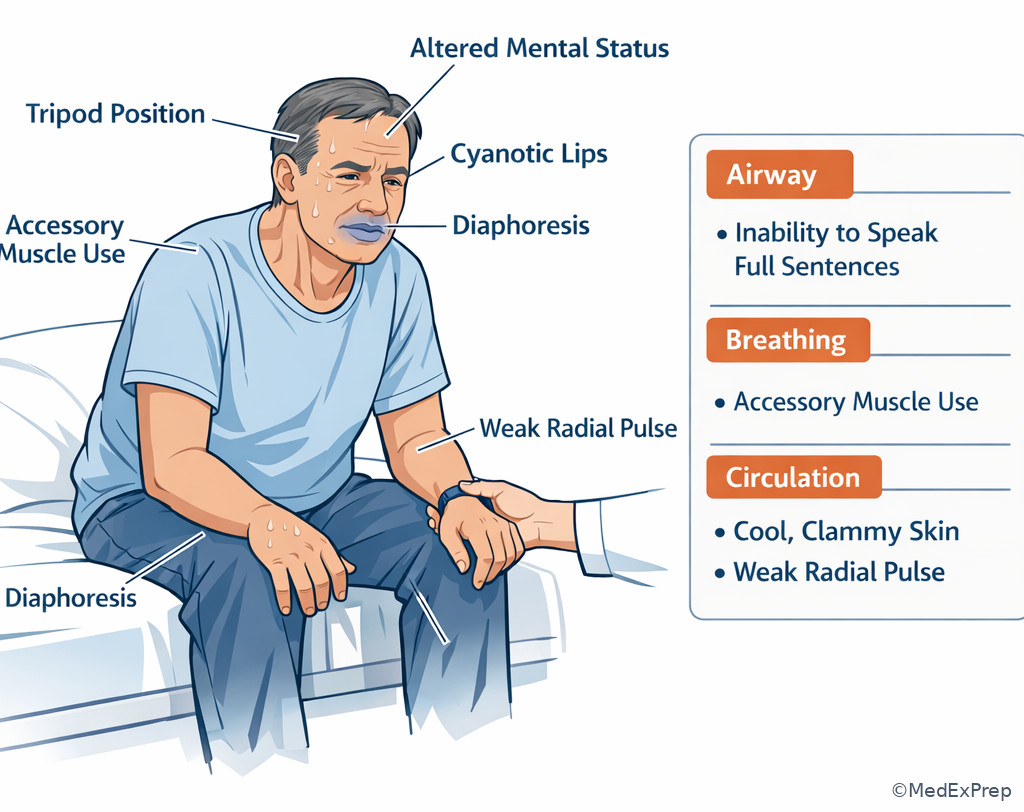
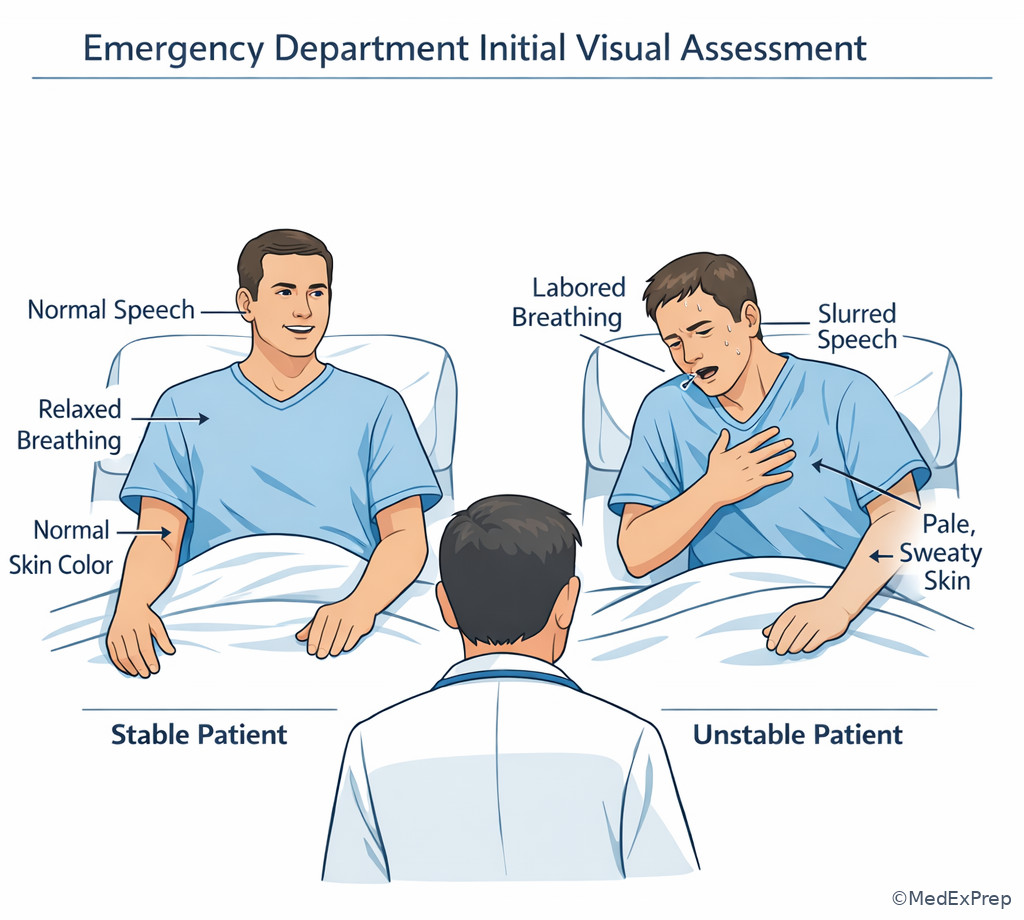
Initial impression is fast and visual: appearance, work of breathing, speech, skin, pulse quality, and mental status. A patient speaking in full sentences with normal mentation and warm perfused skin is usually more stable than one who is restless, diaphoretic, pale, or too dyspneic to talk. The most dangerous mistake is being reassured by one “normal” value, such as an oxygen saturation of 96%, when the patient is tiring, obtunded, or unable to clear secretions.
See Fig 1 for the rapid triage logic that compresses this first-pass decision. Also see Fig 2 for how airway, breathing, and circulation diverge into different immediate actions.
B Worked example
A 68-year-old man with COPD, coronary artery disease, and chronic kidney disease presents with “shortness of breath.” He is anxious, diaphoretic, and speaking in 1–2 word phrases. Temperature is 37.0 C, blood pressure 146/88 mm Hg, pulse 128/min, respiratory rate 34/min, oxygen saturation 95% on room air. He has diffuse wheezing, but also uses accessory muscles and cannot finish sentences. A venous bicarbonate returns at 24 mEq/L, which looks reassuring.
Reasoning chain: Identify task: most appropriate next step. Extract key facts: severe work of breathing, inability to speak, tachypnea, accessory muscle use. Apply rule: apparent oxygen saturation does not override bedside signs of impending respiratory failure. Eliminate distractors: chest x-ray and ABG may be useful later; CT angiography is tempting because tachycardia and dyspnea suggest PE, but he first needs stabilization. Verify: immediate oxygen and inhaled bronchodilator therapy with close reassessment; if fatigue worsens, prepare ventilatory support.
C Exam trap
D Checkpoint
Question: A 59-year-old woman with diabetes and hypertension presents with abdominal pain and vomiting. She is pale, confused, and repeatedly asks for water. BP is 84/52 mm Hg, HR 132/min, RR 24/min, oxygen saturation 98% on room air. Which is the most appropriate next step?
- CT abdomen with contrast
- Two large-bore IV lines and immediate resuscitation
- Serum lipase measurement
- Urgent GI consultation before treatment
Answer: B
- A: Tempting because abdominal catastrophe is plausible; wrong because hypotension and confusion require stabilization before transport or contrast imaging.
- B: Right because shock physiology takes priority over diagnostic refinement.
- C: Tempting because pancreatitis is possible; wrong because a lab does not address poor perfusion.
- D: Tempting because a consultant may be needed; wrong because initial resuscitation cannot wait for consultant evaluation.
Exam takeaway: Use visible instability rather than diagnostic certainty to decide whether resuscitation comes before workup.
flowchart TD
A[Patient arrives] --> B{Immediate danger signs?}
B -->|Yes| C[Threatened airway]
B -->|Yes| D[Respiratory distress or failure]
B -->|Yes| E[Poor perfusion or shock]
B -->|Yes| F[Altered mental status]
B -->|No| G[Proceed with focused history and exam]
C --> H[Call for help and secure airway]
D --> I[Oxygen or ventilation support]
E --> J[IV access and resuscitation]
F --> K[Check glucose and support ABCs]
H --> L[Then targeted diagnostics]
I --> L
J --> L
K --> L Exam takeaway: Match the failing physiologic domain to the first intervention rather than choosing a test too early.
flowchart LR
A[Red flag patient] --> B{Which domain is failing most?}
B --> C[Airway]
B --> D[Breathing]
B --> E[Circulation]
C --> C1[Stridor drooling gurgling cannot protect airway]
C1 --> C2[Prepare definitive airway]
D --> D1[Severe work of breathing cyanosis silent chest bradypnea]
D1 --> D2[Oxygen and ventilation support]
E --> E1[Hypotension weak pulses cool skin confusion]
E1 --> E2[IV access fluids or blood as indicated]
C2 --> F[Reassess continuously]
D2 --> F
E2 --> F Exam takeaway: Visual recognition of posture, speech limitation, skin perfusion, and mental-status change helps you identify instability before tests return.
Exam takeaway: A quick visual scan can reveal severe distress before vital signs are fully documented.
1.1.1.4 Airway first: when patency or protection is failing
A Explanation
The decision conflict here is observe and gather more data versus secure the airway now. The single finding that resolves it is evidence that the patient cannot maintain or protect the airway: stridor, gurgling, pooling secretions, facial/neck trauma, severe angioedema, rapidly declining mental status, or inability to speak due to obstruction. Oxygen can buy time, but it does not fix a mechanically threatened airway.
WHY THIS IS TESTED: Step 2 CK likes to separate patients who need immediate airway control from those who only need oxygen or noninvasive support. Students often overvalue pulse oximetry and undervalue drooling, hoarseness, or mental-status decline.
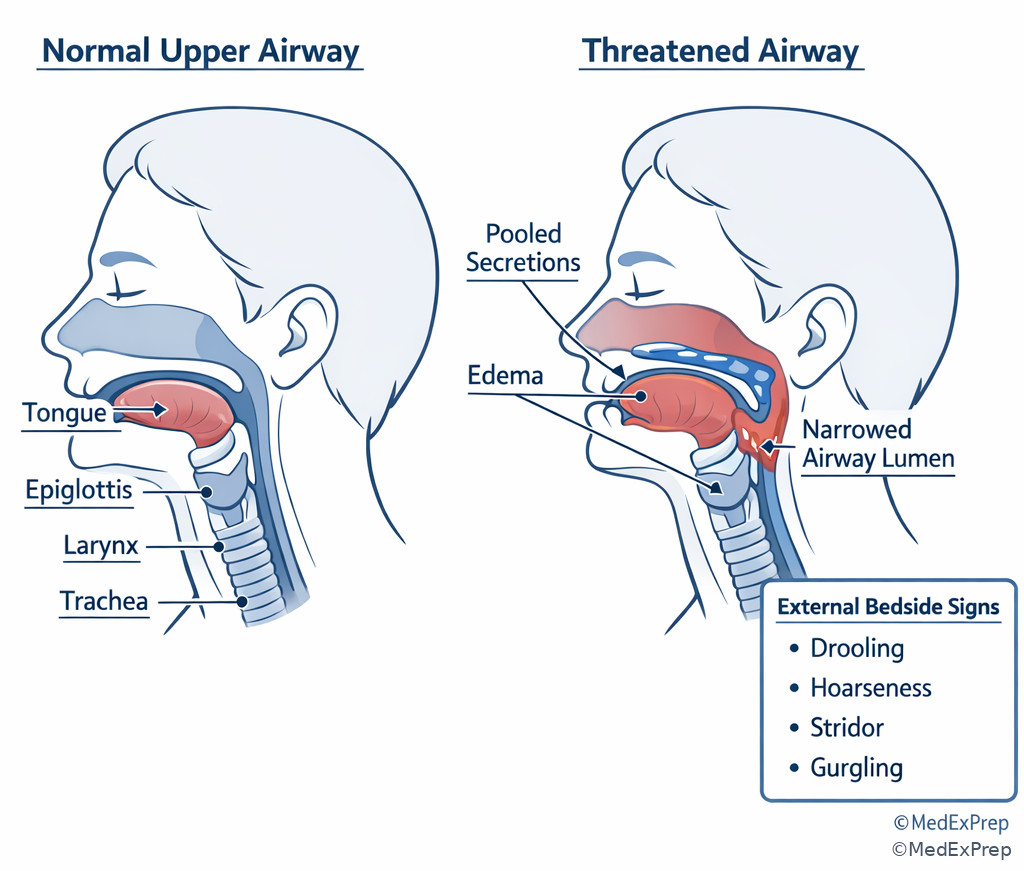
Airway compromise is about patency and protection. A patient with normal oxygen saturation who is obtunded after overdose may still need airway protection. A patient with anaphylaxis and progressive hoarseness may decompensate before saturation falls. A trauma patient with facial fractures, blood in the oropharynx, and gurgling has an airway problem even before severe desaturation appears. The exam pattern is simple: if secretions, swelling, obstruction, or depressed consciousness threaten airway control, call for help early and prepare for definitive airway management.
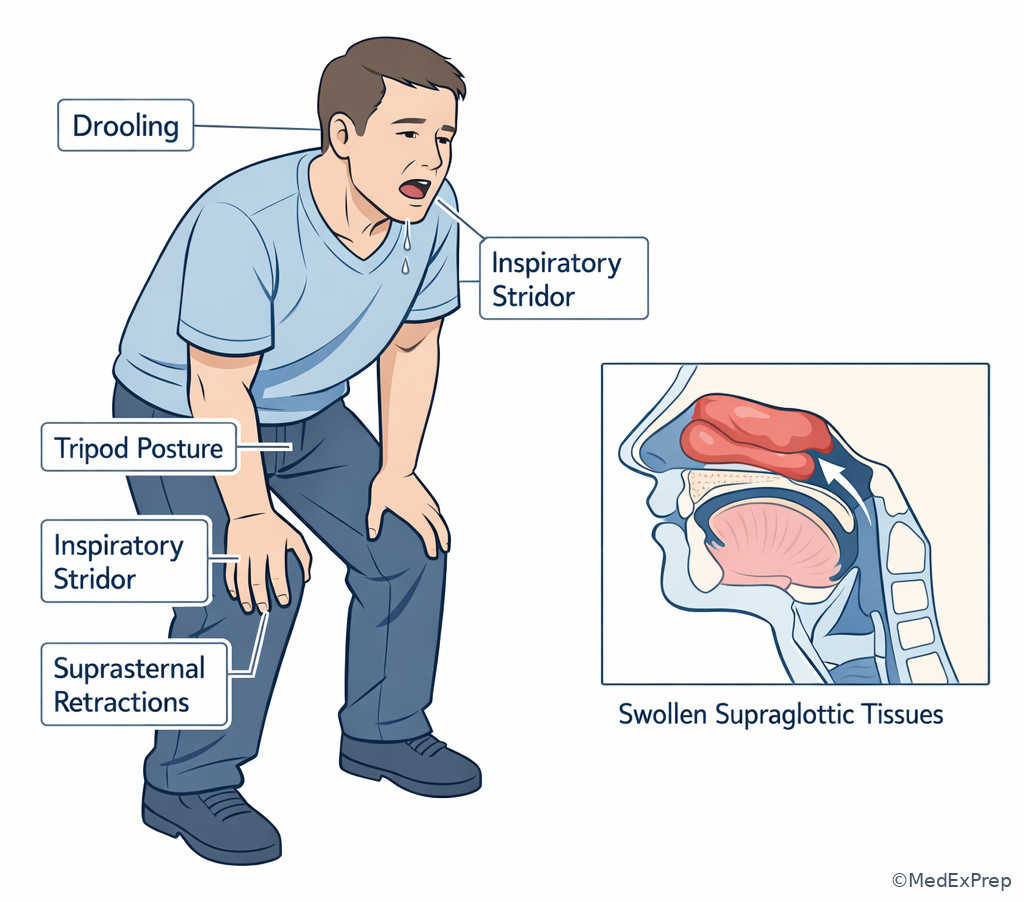
See Fig 4 for a comparison of patent versus threatened airway signs. For a practical progression from bedside signs to intervention, see Fig 5.
B Worked example
A 31-year-old woman with asthma, peanut allergy, and eczema develops throat tightness 10 minutes after eating at a restaurant. She is anxious and says her “voice sounds weird.” BP is 102/64 mm Hg, HR 118/min, RR 24/min, oxygen saturation 98% on room air. She has lip swelling, diffuse urticaria, and mild wheezing. A trainee wants a chest x-ray because of the wheeze.
Reasoning chain: Identify task: best initial therapy. Extract key facts: allergic trigger, mucocutaneous findings, hoarseness, airway edema risk. Apply rule: impending airway compromise from anaphylaxis is treated immediately; normal saturation does not reassure. Eliminate distractors: albuterol may help wheeze but does not treat life-threatening upper airway edema; antihistamines and steroids are adjuncts, not first-line rescue. Verify: intramuscular epinephrine is the immediate step while preparing for airway deterioration if symptoms progress.
C Exam trap
D Checkpoint
Question: A 47-year-old man is brought after an opioid overdose. He is somnolent, vomit is present on his shirt, and he has gurgling respirations. Oxygen saturation is 97% with supplemental oxygen from EMS. Which is the most appropriate immediate priority?
- Head CT
- Airway protection and suctioning
- Serum toxicology panel
- Observation because oxygenation is normal
Answer: B
- A: Tempting because altered mental status can reflect intracranial pathology; wrong because the immediate threat is aspiration and airway compromise.
- B: Right because gurgling and emesis show inability to protect the airway despite acceptable oxygen saturation.
- C: Tempting because overdose is likely; wrong because lab confirmation does not precede airway management.
- D: Tempting because pulse oximetry looks okay; wrong because airway protection is failing.
Exam takeaway: Hoarseness, drooling, secretions, and stridor predict airway failure earlier than pulse oximetry alone.
Exam takeaway: If the patient cannot maintain or protect the airway, immediate airway escalation outranks diagnostic testing.
flowchart TD
A[Airway concern] --> B{Can patient speak clearly and handle secretions?}
B -->|Yes| C[Monitor closely and treat cause]
B -->|No| D[Threatened airway]
D --> E[Suction and position]
D --> F[Prepare bag-mask ventilation]
D --> G[Call airway team]
G --> H[Definitive airway]
C --> I[Reassess for progression] Exam takeaway: Board stems may signal upper airway failure with drooling and stridor rather than low oxygen saturation.
- True or False: A normal pulse oximetry reading excludes a threatened airway. False.
- The bedside finding that most strongly suggests poor airway protection after overdose is gurgling with secretions/emesis.
- Name 3 classic airway red flags: stridor, drooling, decreased consciousness.
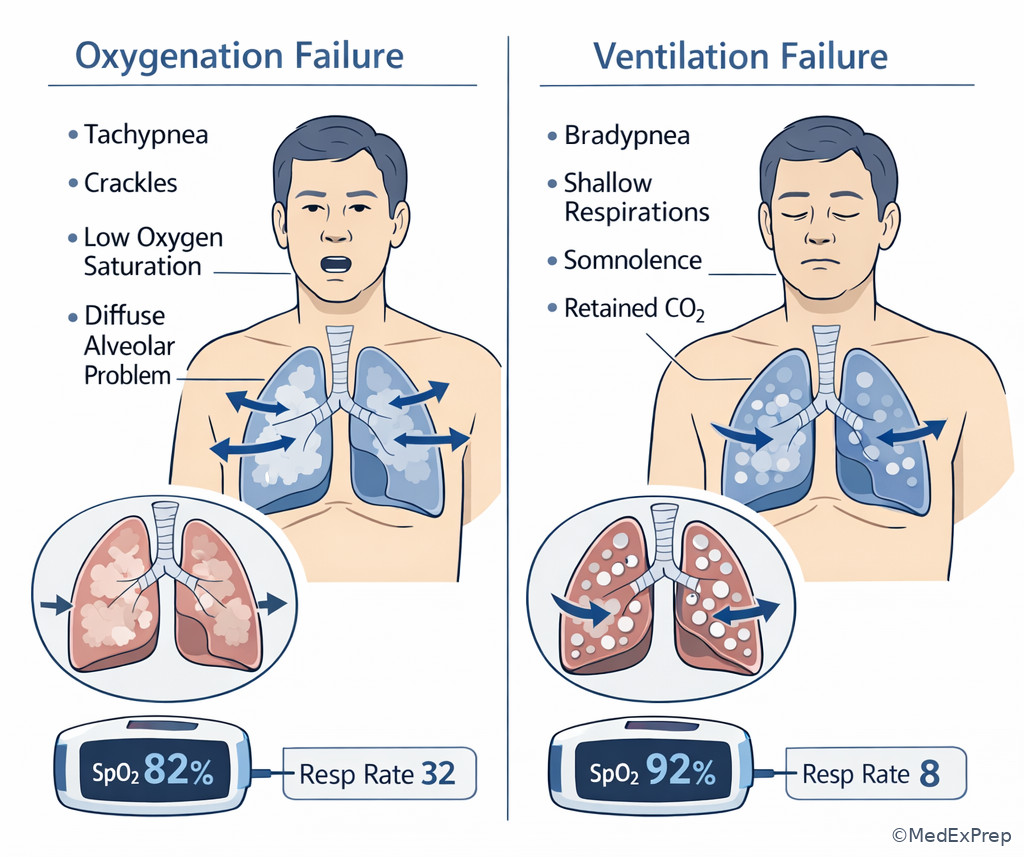
1.1.1.5 Breathing: oxygenation failure versus ventilation failure
A Explanation
The decision conflict is give oxygen and wait versus support ventilation now. The single rule: if breathing effort is failing, respiratory rate is inadequate, the chest is becoming silent, or the patient is tiring or obtunded, think ventilation failure rather than isolated hypoxemia. Oxygen treats low oxygen content; ventilation support treats inadequate air movement and carbon dioxide clearance.
WHY THIS IS TESTED: the exam often presents dyspnea with multiple plausible causes, but the correct answer depends on whether the patient needs oxygen alone, noninvasive positive pressure, bag-mask ventilation, bronchodilators, or urgent intubation.
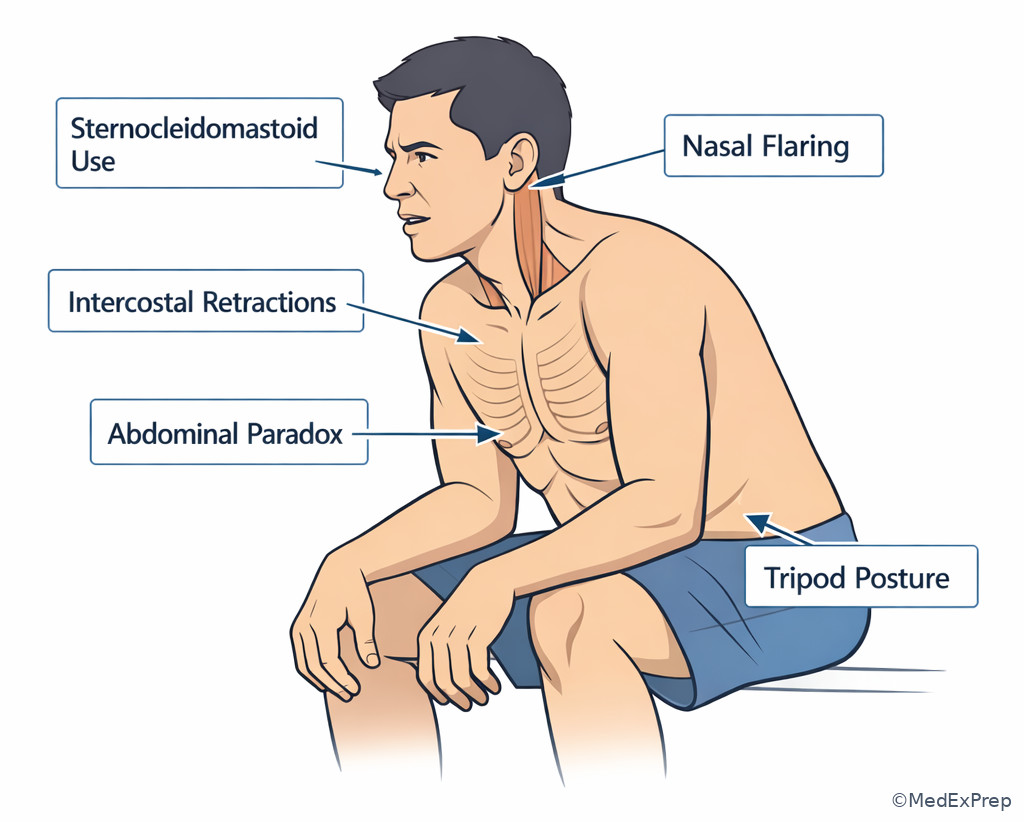
Breathing assessment asks: Is air moving? Is the patient oxygenating? Is the patient tiring? Increased work of breathing, accessory muscles, nasal flaring, retractions, cyanosis, or inability to speak suggest major distress. Bradypnea, shallow respirations, and declining mental status suggest ventilatory failure, especially in overdose, neuromuscular weakness, severe asthma exhaustion, or COPD hypercapnia. In severe asthma, a “silent chest” is more dangerous than loud wheezing because it suggests minimal airflow. In pulmonary edema, crackles with hypoxemia may improve with positive pressure support. In opioid intoxication, pinpoint pupils and hypoventilation direct you to ventilation support and naloxone, not a broad pulmonary workup.
See Fig 6 for a visual comparison of oxygenation failure and ventilation failure.
B Worked example
A 24-year-old woman with severe asthma, allergic rhinitis, and anxiety presents with wheezing after cat exposure. She received two home albuterol treatments. Temperature is 36.9 C, BP 134/82 mm Hg, HR 124/min, RR 10/min, oxygen saturation 92% on room air. She appears drowsy and has barely audible breath sounds bilaterally. A mildly elevated white blood cell count is noted, which tempts concern for infection.
Reasoning chain: Identify task: most appropriate next step. Extract key facts: known asthma, low respiratory rate, drowsiness, almost silent chest. Apply rule: reduced air movement with fatigue signals impending respiratory arrest. Eliminate distractors: chest x-ray and antibiotics are tempting because of leukocytosis, but stress and beta-agonists can raise the WBC count; additional outpatient-style nebulizer planning is too slow. Verify: provide immediate aggressive respiratory support and prepare for definitive airway management if not rapidly improving.
C Exam trap
D Checkpoint
Question: A 72-year-old man with heart failure and COPD is brought in for dyspnea. He is tachypneic, using accessory muscles, and speaking in short phrases. Oxygen saturation is 84% on room air, RR 30/min, BP 168/96 mm Hg. Bilateral crackles are present. Which bedside interpretation is most important right now?
- He needs antibiotics before any respiratory support
- He has isolated anxiety causing tachypnea
- He has clinically significant breathing failure requiring immediate support
- Normal mentation excludes imminent respiratory decompensation
Answer: C
- A: Tempting because crackles can accompany pneumonia; wrong because the immediate issue is hypoxemic respiratory distress.
- B: Tempting because anxiety causes rapid breathing; wrong because objective hypoxemia and crackles point to cardiopulmonary disease.
- C: Right because severe hypoxemia with work of breathing requires immediate respiratory support.
- D: Tempting because he is still awake; wrong because normal mentation does not erase dangerous respiratory effort and hypoxemia.
Exam takeaway: Hypoxemia and hypoventilation may overlap, but drowsiness, bradypnea, and poor chest movement point to the need for ventilatory support.
Exam takeaway: Accessory muscle use and retractions are visual clues to severe respiratory distress even before blood gas results return.
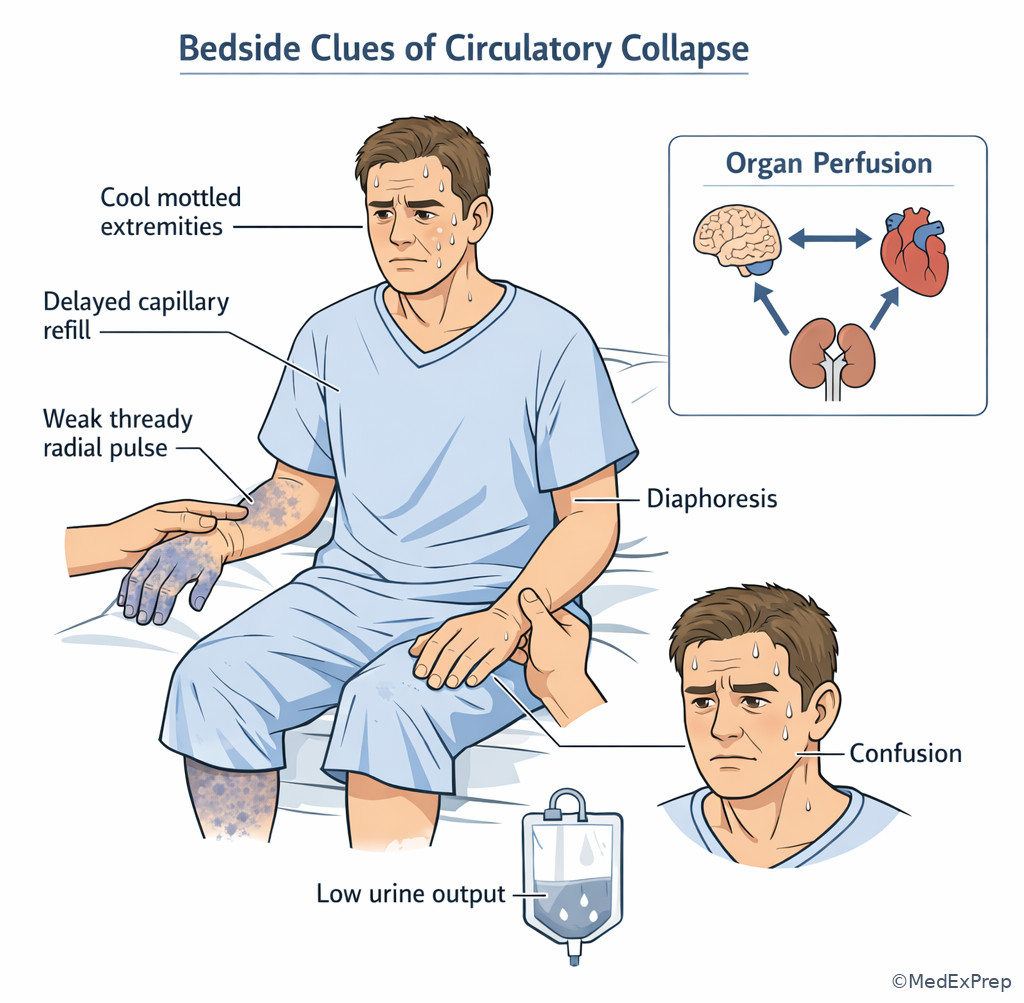
1.1.1.6 Circulation: recognize shock before the blood pressure crashes
A Explanation
The decision conflict is wait for confirmatory data versus treat presumed poor perfusion immediately. The single rule: signs of organ hypoperfusion matter more than a single blood pressure number. A patient can be in early shock before profound hypotension appears.
WHY THIS IS TESTED: Step 2 CK routinely gives subtle shock clues—tachycardia, cool extremities, diaphoresis, confusion, delayed capillary refill, oliguria—while distracting you with a tempting diagnosis-specific workup. The right answer is often access, fluids or blood, monitoring, and source-directed bedside action.
Circulation is about perfusion, not just pressure. Weak pulses, narrow pulse pressure, mottled skin, altered mentation, chest pain with diaphoresis, or reduced urine output all suggest inadequate effective circulation. If hemorrhage is possible, think blood loss and control the source. If sepsis is plausible, upcoming lessons will extend this to cultures, antibiotics, and lactate—but even there, the first bedside recognition is poor perfusion. If obstructive or cardiogenic causes are suspected, resuscitation still starts with recognition of instability and fast escalation. This lesson stays at the broad ABC level: identify poor circulation and initiate immediate support before chasing the exact shock subtype.
See Fig 1 and Fig 2 for where circulation branches off from the general triage process, then use the differential table below to separate common patterns.
B Worked example
A 76-year-old woman with atrial fibrillation on apixaban, osteoarthritis, and chronic anemia presents after several episodes of melena. She reports mild epigastric discomfort. BP is 108/66 mm Hg, HR 122/min, RR 22/min, oxygen saturation 99% on room air. She is cool, pale, and intermittently confused. Hemoglobin returns at 10.1 g/dL, which seems “not that low.”
Reasoning chain: Identify task: most appropriate next step. Extract key facts: ongoing GI bleeding risk, anticoagulant use, tachycardia, confusion, cool skin. Apply rule: shock is a bedside perfusion diagnosis; an early hemoglobin can appear falsely reassuring in acute hemorrhage. Eliminate distractors: endoscopy is likely needed later but not before resuscitation; CT angiography is premature in an unstable-looking patient. Verify: establish large-bore IV access, begin resuscitation, and escalate appropriately.
C Exam trap
D Checkpoint
Question: Which finding most strongly indicates clinically important circulatory compromise in a patient whose systolic blood pressure is still 104 mm Hg?
- Warm hands and normal mentation
- Delayed capillary refill and confusion
- Normal oxygen saturation on room air
- Mild abdominal tenderness without tachycardia
Answer: B
- A: Tempting because blood pressure may still be okay; wrong because these findings argue against poor perfusion.
- B: Right because both findings reflect inadequate organ and peripheral perfusion.
- C: Tempting because monitoring values feel objective; wrong because oxygen saturation does not assess circulation.
- D: Tempting because abdominal pathology can bleed; wrong because the listed clues do not establish circulatory failure.
- The most reliable early bedside clue of shock is not always hypotension; it is often poor perfusion.
- True or False: A normal early hemoglobin excludes acute blood loss. False.
- Name 3 circulation red flags: weak pulses, cool clammy skin, confusion.
| Threat pattern | Choose this first | Reject this early move | Single clue |
|---|---|---|---|
| Gurgling, emesis, low consciousness | Airway protection / suction | Head CT first | Cannot protect airway |
| Severe work of breathing, silent chest | Ventilatory support | Chest x-ray before treatment | Poor air movement and fatigue |
| Tachycardia, cool skin, confusion | Circulatory resuscitation | Definitive imaging first | Organ hypoperfusion |
| Allergic trigger, hoarseness, urticaria | Immediate IM epinephrine | Antihistamines alone | Airway involvement |
| Pinpoint pupils, bradypnea | Ventilation support plus naloxone | Toxicology panel first | Respiratory drive failure |
1.1.1.7 Integration: sequence the next best step under Step 2 CK pressure
A Explanation
The final decision conflict is diagnose the disease versus choose the safest sequence. The single rule: on Step 2 CK, the correct answer usually reflects the best order of care—stabilize, then confirm, then treat definitively, then disposition. The hardest stems add noise: a borderline lab, a plausible alternative diagnosis, or an attractive imaging study. Your job is to identify the governing principle and ignore the noise.
WHY THIS IS TESTED: many missed questions come from selecting an intervention that is generally useful but mistimed for the patient’s current acuity.
A reliable sequence is: identify the task, assess acuity, choose the failing domain, start the first stabilizing action, then reassess and pursue the likely cause. If a patient with trauma has diminished breath sounds and hypotension, do not send for CT first. If a patient with severe GI bleeding is cool, tachycardic, and confused, do not anchor on the hemoglobin. If a patient with suspected sepsis is altered and hypotensive, upcoming sepsis management still begins with ABC stabilization. This sequencing framework turns broad emergency questions into a manageable pattern.
See Fig 5 for the airway decision tree, and use Fig 1 as the overarching template for all unstable-patient stems.
B Worked example
A 55-year-old man with obesity, obstructive sleep apnea, and alcohol use disorder is found unresponsive after vomiting. He has snoring respirations, oxygen saturation 93% on 2 L nasal cannula, RR 8/min, BP 92/58 mm Hg, and pinpoint pupils. The nurse mentions he also complained of chest pain earlier, which makes ACS tempting.
Reasoning chain: Identify task: most appropriate next step. Extract key facts: unresponsiveness, snoring respirations, vomiting, bradypnea, opioid toxidrome clue. Apply rule: airway and ventilation first; supplemental oxygen does not solve hypoventilation or aspiration risk. Eliminate distractors: ECG and troponin matter later if concern persists, but not before supporting breathing. Verify: immediate airway support, naloxone, suction, and close reassessment.
C Exam trap
D Checkpoint
Question: A patient with severe abdominal pain, tachycardia, confusion, and cool extremities is suspected to have perforated viscus. Which principle best determines the next step?
- Order the test with the highest diagnostic yield first
- Stabilize airway, breathing, and circulation before definitive imaging
- Wait for a consultant before placing IV access
- Treat pain first because analgesia improves examination accuracy
Answer: B
- A: Tempting because imaging is often diagnostic; wrong because unstable physiology changes the sequence.
- B: Right because initial stabilization is the governing principle in an unstable patient.
- C: Tempting if surgery is likely; wrong because bedside resuscitation is not deferred.
- D: Tempting because pain control is important; wrong because circulation threats come first.
Exam takeaway: Cool clammy skin, weak pulses, and altered mentation can identify shock before severe hypotension appears.
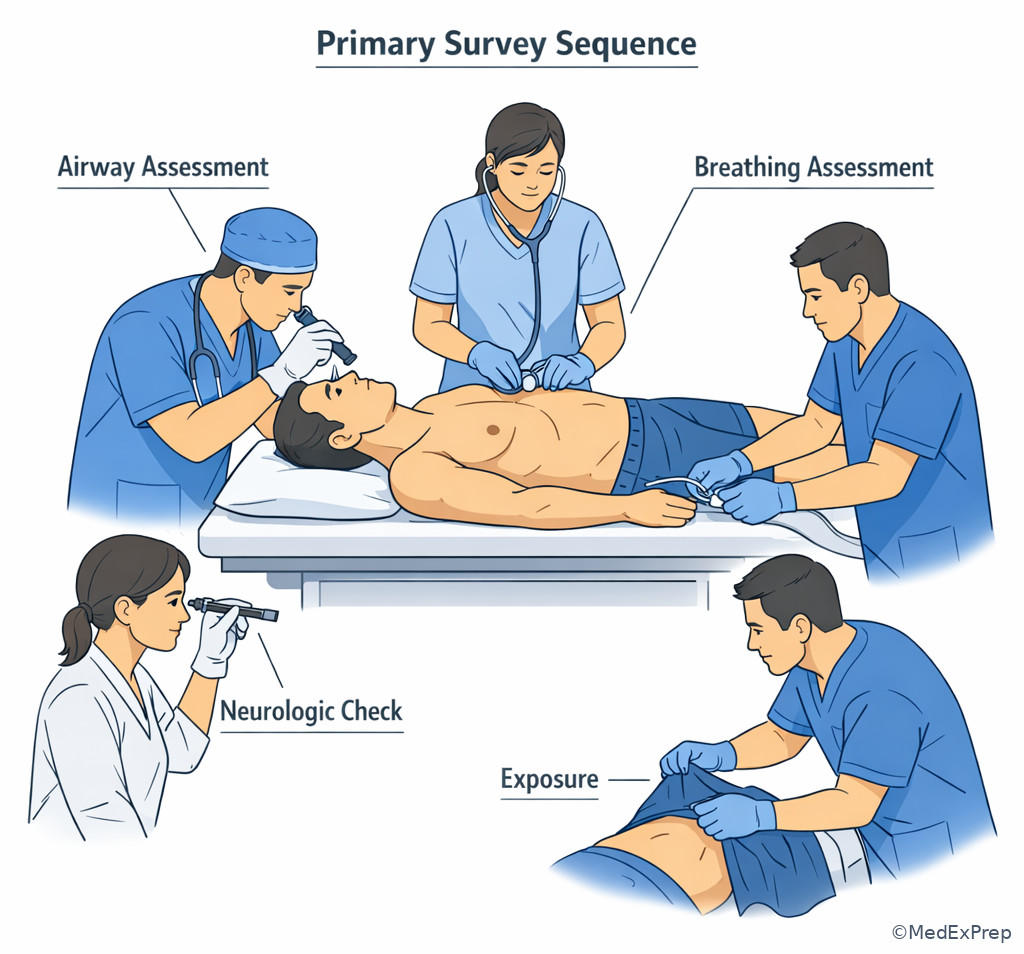
Exam takeaway: The primary survey is a structured bedside sequence for finding and treating immediate threats before advanced testing.
| Finding | Most likely failing domain | Why the tempting alternative is wrong | Best immediate focus |
|---|---|---|---|
| Drooling + muffled voice | Airway | Breathing treatments do not relieve upper airway obstruction | Airway protection |
| Bradypnea + somnolence | Breathing/ventilation | Normal oxygen reading can coexist with inadequate ventilation | Ventilatory support |
| Tachycardia + cool clammy skin + confusion | Circulation | Borderline blood pressure may mask early shock | Resuscitation and monitoring |
| Urticaria + hoarseness after exposure | Airway/anaphylaxis | Antihistamines are too slow as sole therapy | Immediate IM epinephrine |
| Silent chest in asthma | Breathing failure | Less wheezing does not mean improvement | Aggressive respiratory support |
| Melena + tachycardia + confusion | Circulation/hemorrhagic shock | Hemoglobin can be falsely reassuring early | Large-bore IV access and resuscitation |
| Commonly confused pair | Shared features | Discriminator | Implication |
|---|---|---|---|
| Hypoxemia vs hypoventilation | Dyspnea, distress, low oxygen | Bradypnea/somnolence point to hypoventilation | Ventilation support may be required |
| Wheezing asthma vs upper airway edema | Respiratory distress, noisy breathing | Hoarseness/stridor/drooling point to airway edema | Airway planning and cause-specific therapy |
| Anxiety tachypnea vs respiratory failure | Rapid breathing, fear | Objective hypoxemia, accessory muscles, poor air movement | Treat physiology, not presumed anxiety |
| Stable GI bleed vs hemorrhagic shock | Melena, anemia, tachycardia | Confusion/cool skin/weak pulses indicate shock | Resuscitate before endoscopy |
| Normal saturation vs adequate airway | Acceptable pulse ox | Gurgling or emesis means airway protection failure | Secure airway despite “good sat” |
Exam Traps & Differentiators
- Most common wrong answer and why: ordering the “best test” first. Tempting because the diagnosis is guessable; wrong because ABC failure changes the next step.
- Looks similar but isn't: anxiety can cause tachypnea, but anxiety does not cause silent chest, cyanosis, weak pulses, or progressive obtundation.
- If the stem says hoarseness, drooling, or stridor, think threatened airway.
- If the stem says bradypnea, shallow respirations, or somnolence, think ventilatory failure.
- If the stem says cool clammy skin, confusion, weak pulses, or oliguria, think poor perfusion even before severe hypotension.
- If the stem says normal pulse oximetry but gurgling or emesis, think airway protection problem, not reassurance.
- If the stem says severe asthma with less wheezing and drowsiness, think impending respiratory arrest, not clinical improvement.
Related traps from neighboring upcoming topics matter here. In Shock Types and Bedside Clues, the distractor is often choosing the wrong hemodynamic subtype too early. In Sepsis and Septic Shock, the distractor is jumping to antibiotics and cultures without first recognizing that hypotension or altered mentation still requires immediate ABC-focused stabilization.
| Stem phrase | Think | Do next |
|---|---|---|
| “Unable to speak full sentences” | Severe respiratory distress | Immediate respiratory support and reassessment |
| “Gurgling respirations” | Airway protection failure | Suction and airway management |
| “Cool, clammy, confused” | Shock physiology | IV access and resuscitation |
| “Hoarseness after allergen exposure” | Anaphylaxis with airway involvement | IM epinephrine now |
| “Silent chest” | Minimal airflow, impending arrest | Aggressive ventilation-focused management |
| “Normal oxygen saturation but obtunded” | Do not ignore ventilatory or airway failure | Assess breathing effort and airway protection |
Algorithm / Approach
Rapid Review
- Threatened airway → drooling/stridor/gurgling outrank pulse oximetry
- Airway protection failure → normal oxygen saturation does not reassure
- Ventilation failure → bradypnea and somnolence separate it from isolated hypoxemia
- Severe asthma → silent chest is worse than loud wheezing
- Anaphylaxis with hoarseness → IM epinephrine, not antihistamines first
- Shock recognition → confusion and cool clammy skin can precede marked hypotension
- Acute hemorrhage → early hemoglobin may be misleadingly normal
- Board sequencing → stabilize first, diagnose second
- Transport risk → unstable patients do not go to CT before bedside support
- Respiratory distress → inability to speak full sentences signals severity
- Good “numbers” with bad exam → trust bedside physiology over isolated reassuring data
- Most appropriate next step → often asks for order-of-operations, not final diagnosis
- ABCs → choose the failing domain, then the first matching intervention
Self-check quiz
1. A 45-year-old man with obesity and chronic back pain is brought in after taking unknown pills. He is somnolent, has snoring respirations, and vomit at the bedside. Oxygen saturation is 96% on nasal cannula. Which problem requires immediate clarification first?
- Airway protection failure
- Community-acquired pneumonia
- Acute coronary syndrome
- Pulmonary embolism
2. A 26-year-old woman with asthma and seasonal allergies presents with severe dyspnea. She is drowsy, speaks in one-word answers, and has barely audible breath sounds. Which finding most strongly indicates impending respiratory failure rather than uncomplicated bronchospasm?
- Tachycardia
- Mild wheezing
- Drowsiness with a silent chest
- History of atopy
3. A 70-year-old woman with atrial fibrillation on anticoagulation and peptic ulcer disease presents with melena and dizziness. BP is 94/58 mm Hg, HR 126/min, she is cool and intermittently confused, and hemoglobin is 10.4 g/dL. What is the most appropriate next step?
- Urgent CT angiography before any treatment
- Two large-bore IV lines with immediate resuscitation
- Outpatient proton pump inhibitor and close follow-up
- Wait for repeat hemoglobin to confirm major bleeding
4. A 33-year-old woman with peanut allergy develops urticaria, lip swelling, and hoarseness minutes after eating dessert. BP is 108/70 mm Hg, oxygen saturation is 99% on room air, and mild wheezing is present. What is the most appropriate initial therapy?
- Inhaled albuterol alone
- IV glucocorticoids alone
- IM epinephrine
- Observation with pulse oximetry
5. A 62-year-old man with heart failure and COPD presents with acute dyspnea. He is using accessory muscles, has bilateral crackles, speaks in short phrases, and oxygen saturation is 83% on room air. Which principle best guides the next step?
- Antibiotics should precede respiratory support if crackles are present
- Immediate breathing support takes priority over etiologic confirmation
- Normal mentation excludes severe respiratory compromise
- Chest CT is needed before any bedside intervention
6. A 58-year-old man with diabetes, hypertension, and recent vomiting presents with abdominal pain. BP is 102/64 mm Hg, HR 124/min, RR 26/min, oxygen saturation 98% on room air. He is pale, diaphoretic, and confused. Which detail most strongly supports immediate circulatory resuscitation despite the borderline blood pressure?
- Normal oxygen saturation
- Confusion with diaphoresis and tachycardia
- Abdominal pain severity rated 9/10
- Respiratory rate above 20/min
7. A 41-year-old man with alcohol use disorder is found unresponsive. He has pinpoint pupils, RR 7/min, oxygen saturation 95% on face mask, and gurgling respirations. The team is considering head CT, naloxone, chest x-ray, and observation. What is the most appropriate next step?
- Immediate airway support with suction and ventilation assistance
- Head CT because altered mental status may indicate intracranial hemorrhage
- Observation because oxygen saturation is preserved
- Chest x-ray to evaluate aspiration before intervention
8. A 67-year-old woman with COPD, chronic kidney disease, and coronary disease presents with dyspnea and chest tightness. She is anxious, can speak only 2 words at a time, has RR 34/min, HR 130/min, oxygen saturation 95% on room air, and marked accessory muscle use. Which is the most appropriate next step?
- CT pulmonary angiography
- Serial troponin testing before treatment
- Immediate respiratory support and bedside stabilization
- Discharge with close outpatient follow-up because saturation is normal
Answer key
1. Correct answer: A — Airway protection failure.
- A: Tempting because snoring respirations and emesis clearly point to upper airway obstruction and aspiration risk; correct because the single discriminating clue is inability to protect the airway despite acceptable oxygen saturation. Source: American Heart Association resuscitation guidance; Tintinalli emergency airway approach.
- B: Tempting because aspiration or hypoventilation can later lead to pneumonia; incorrect because pneumonia does not explain the immediate snoring airway obstruction requiring urgent action. Discriminating clue: vomit plus snoring respirations.
- C: Tempting because overdose patients can have chest symptoms or cardiac events; incorrect because airway compromise kills faster than undifferentiated cardiac risk. Discriminating clue: somnolence with snoring.
- D: Tempting because hypoxia and tachycardia can suggest PE; incorrect because nothing here outranks the immediate need to clear and protect the airway. Discriminating clue: visible emesis and obstructed breathing sounds.
2. Correct answer: C — Drowsiness with a silent chest.
- A: Tempting because tachycardia commonly appears in severe asthma; incorrect because it is nonspecific and can reflect distress, beta-agonists, or anxiety. Discriminating clue: it does not establish fatigue or poor airflow.
- B: Tempting because wheezing signals bronchospasm; incorrect because mild wheezing alone is less ominous than near absence of breath sounds. Discriminating clue: a silent chest indicates minimal airflow.
- C: Tempting because it sounds dramatic; correct because drowsiness plus silent chest identifies impending respiratory arrest from exhaustion and inadequate ventilation. Source: GINA recommendations; standard emergency medicine texts.
- D: Tempting because atopy supports asthma; incorrect because it does not gauge acuity. Discriminating clue: history does not outweigh current respiratory fatigue signs.
3. Correct answer: B — Two large-bore IV lines with immediate resuscitation.
- A: Tempting because CT angiography can localize bleeding; incorrect because unstable perfusion requires bedside resuscitation before transport. Discriminating clue: cool skin and confusion.
- B: Tempting because it sounds general rather than disease-specific; correct because shock from likely GI bleeding must be treated immediately even if hemoglobin is not profoundly low. Source: ACG guidance for GI bleeding; Harrison's Principles of Internal Medicine.
- C: Tempting because peptic ulcer disease raises interest in acid suppression; incorrect because outpatient treatment is unsafe in hemodynamic compromise. Discriminating clue: hypotension and tachycardia.
- D: Tempting because laboratory confirmation feels objective; incorrect because early hemoglobin can be misleading in acute hemorrhage. Discriminating clue: bedside perfusion is already abnormal.
4. Correct answer: C — IM epinephrine.
- A: Tempting because wheezing suggests bronchospasm; incorrect because albuterol does not reverse systemic anaphylaxis or impending upper airway edema. Discriminating clue: hoarseness after allergen exposure.
- B: Tempting because steroids are commonly given; incorrect because they are adjunctive and slower than the life-saving first-line intervention. Discriminating clue: immediate airway involvement.
- C: Tempting because the picture fits anaphylaxis; correct because mucocutaneous findings plus hoarseness after exposure indicate anaphylaxis requiring immediate IM epinephrine even when oxygen saturation is normal. Source: AAAAI/anaphylaxis guidelines; emergency medicine standards.
- D: Tempting because the blood pressure and oxygen saturation are not yet profoundly abnormal; incorrect because early airway symptoms can precede collapse. Discriminating clue: voice change.
5. Correct answer: B — Immediate breathing support takes priority over etiologic confirmation.
- A: Tempting because crackles may reflect pneumonia; incorrect because treatment sequencing still prioritizes respiratory support for severe hypoxemia and distress. Discriminating clue: oxygen saturation 83% with accessory muscle use.
- B: Tempting because it sounds like a broad principle; correct because immediate support of breathing comes before exact etiologic confirmation in severe dyspnea. Source: ACC/AHA acute heart failure guidance; emergency respiratory care principles.
- C: Tempting because awake patients can seem less sick; incorrect because severe hypoxemia and inability to speak full sentences already establish dangerous respiratory compromise. Discriminating clue: short-phrase speech and major work of breathing.
- D: Tempting because advanced imaging can clarify diagnosis; incorrect because bedside support cannot wait. Discriminating clue: marked instability with low oxygen saturation.
6. Correct answer: B — Confusion with diaphoresis and tachycardia.
- A: Tempting because a normal oxygen saturation can seem reassuring; incorrect because oxygenation does not assess perfusion. Discriminating clue: the patient is still confused and diaphoretic.
- B: Tempting because it clusters multiple concerning signs; correct because these are classic indicators of poor perfusion that justify immediate circulatory resuscitation even before severe hypotension. Source: Harrison's; emergency medicine shock evaluation principles.
- C: Tempting because severe pain suggests serious pathology; incorrect because pain intensity alone does not establish shock. Discriminating clue: perfusion findings, not pain score, determine urgency.
- D: Tempting because tachypnea often accompanies severe illness; incorrect because it is less specific for circulatory collapse than altered mentation with diaphoresis and tachycardia. Discriminating clue: organ hypoperfusion signs are stronger.
7. Correct answer: A — Immediate airway support with suction and ventilation assistance.
- A: Tempting because opioid toxicity is obvious; correct because the immediate threat is combined airway contamination and hypoventilation, so suction and ventilation support come first along with naloxone as appropriate. Discriminating clue: gurgling respirations with RR 7/min. Source: AHA toxicologic emergencies; emergency airway texts.
- B: Tempting because intracranial hemorrhage can cause coma; incorrect because the patient is not yet stabilized for transport and has a reversible airway/breathing threat at bedside. Discriminating clue: pinpoint pupils and hypoventilation.
- C: Tempting because saturation is preserved on supplemental oxygen; incorrect because oxygenation does not fix inadequate ventilation or aspiration risk. Discriminating clue: bradypnea and gurgling.
- D: Tempting because aspiration is plausible; incorrect because imaging does not precede airway management. Discriminating clue: active airway compromise.
8. Correct answer: C — Immediate respiratory support and bedside stabilization.
- A: Tempting because dyspnea, chest tightness, and tachycardia can suggest pulmonary embolism; incorrect because the patient has severe respiratory distress and cannot safely wait for CT before stabilization. Discriminating clue: 2-word speech with marked accessory muscle use.
- B: Tempting because coronary disease raises concern for ACS; incorrect because serial cardiac testing does not outrank obvious respiratory compromise. Discriminating clue: work of breathing is the immediate danger.
- C: Tempting because it sounds nonspecific; correct because severe distress and limited speech signal a breathing emergency even though oxygen saturation is not profoundly low. Source: standard emergency medicine dyspnea assessment; Step-style stabilization principles.
- D: Tempting because the saturation is 95%; incorrect because normal or near-normal saturation does not exclude impending respiratory failure. Discriminating clue: accessory muscle use and inability to speak normally.