Why it matters
- Most PANCE misses are not due to never having heard of the disease; they come from misframing the case before choosing an answer.
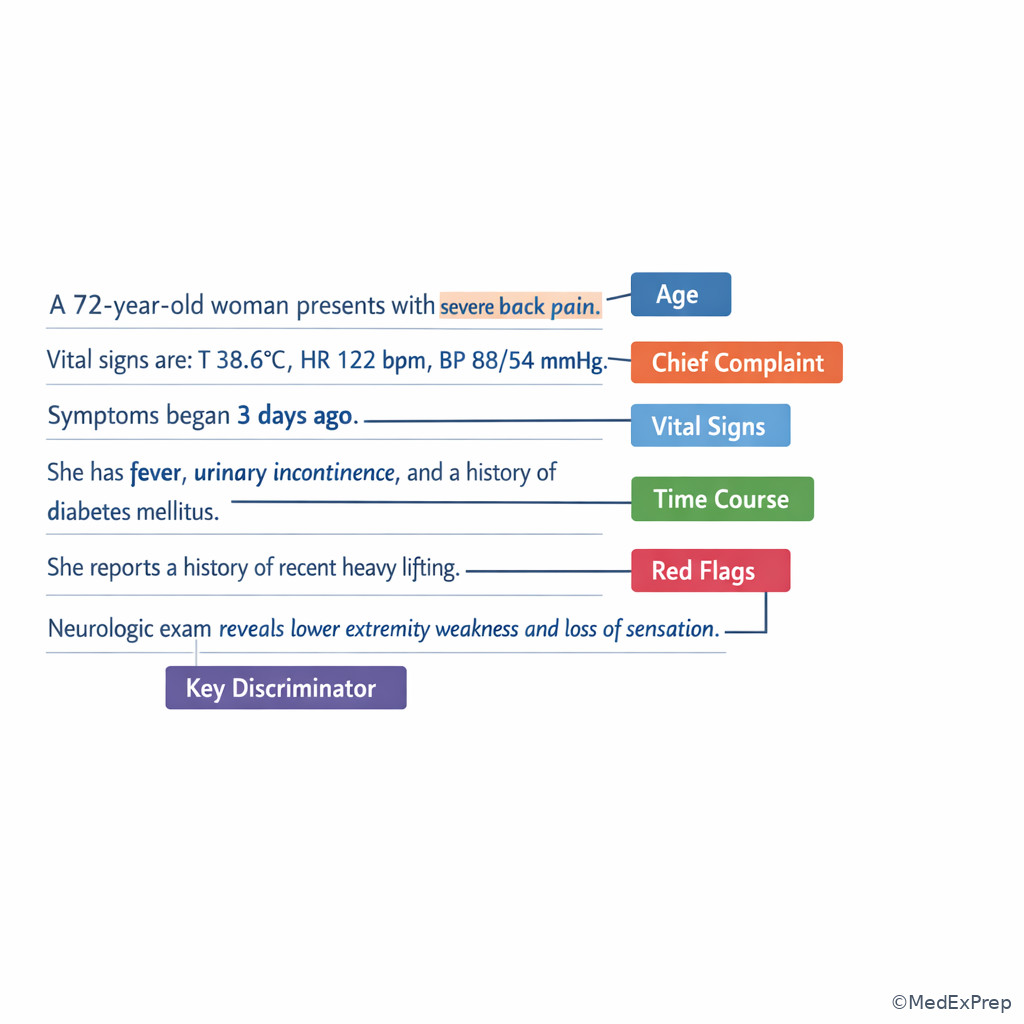
- A good problem representation turns a long vignette into a short decision tool: who is the patient, how sick are they, what syndrome is present, and what single clue rules in or rules out the leading options.
- This framework is the bridge between reading the stem and answering “most likely diagnosis,” “most appropriate test,” or “best next step.”
- Safe exam reasoning starts with stability and red flags; if the representation is wrong, the management choice will also be wrong.
Exam takeaway: Build the answer from stability, syndrome, and discriminating clues rather than from the first familiar diagnosis in the stem.
flowchart LR A[Read stem] --> B[Identify task] B --> C[Assess stability and red flags] C --> D[Create one-line problem representation] D --> E[Match illness script] E --> F[Choose test or treatment] F --> G[Verify against age, timing, contraindications]
See Fig 1 for the overall sequence you should run on nearly every vignette.
Key Terms & Must-Know Facts
1.1.1.1 Key terms
- Problem representation: a one-line summary of the patient using high-yield features.
- Semantic qualifiers: paired descriptors such as acute/chronic, unilateral/bilateral, severe/mild, focal/diffuse.
- Illness script: the mental disease pattern that links risk factors, timing, findings, and next steps.
- Signal: information that changes the differential or management.
- Noise: incidental information that feels specific but does not govern the answer.
- Discriminator: the single clue that separates close answer choices.
- Syndrome framing: categorizing the case as chest pain, dyspnea, shock, anemia, rash, abdominal pain, and so on.
- Pretest probability: how likely a diagnosis is before testing.
- Red flag: a feature suggesting emergency, complication, or need for escalation.
- Best next step: the immediate action that changes outcome or clarifies the diagnosis most efficiently.
- Pivot point: the moment in the stem where one new detail should reorder your differential.
- Distractor: a plausible but wrong option supported by superficial clues.
1.1.1.2 Must-know facts
- Always identify the task before processing the data.
- Vitals and instability outrank elegant diagnosis-building.
- Age, timing, and severity are usually more important than isolated buzzwords.
- The best one-line representation is short enough to say out loud in one breath.
- Good representations use qualifiers, not long symptom lists.
- The strongest board clue is often the detail that makes one tempting answer unsafe.
- Do not test broadly before deciding whether the patient is stable.
- “Most appropriate next step” often means stabilize first, then confirm.
- The correct answer must fit all major clues, not just one memorable clue.
| Element | Include in problem representation | Why it matters on boards |
|---|---|---|
| Demographics | Age, sex if relevant, pregnancy status if relevant | Changes disease prevalence and safety decisions |
| Time course | Acute, subacute, chronic, recurrent | Separates emergencies from chronic processes |
| Severity | Stable vs unstable, mild vs severe | Determines first action and disposition |
| Syndrome | Chest pain, dyspnea, abdominal pain, focal deficit | Keeps differential organized |
| Key findings | Only the top 2-4 discriminators | Prevents drowning in noise |
| Context | Comorbidities, exposures, medications | Creates or removes leading diagnoses |
| Red flags | Shock, hypoxia, neuro deficits, peritonitis | Overrides routine workup |
Exam takeaway: Label the stem by task, red flags, timing, and discriminators before looking at the options.
Core content
1.1.1.3 Foundational structure: what a problem representation must contain
A Explanation
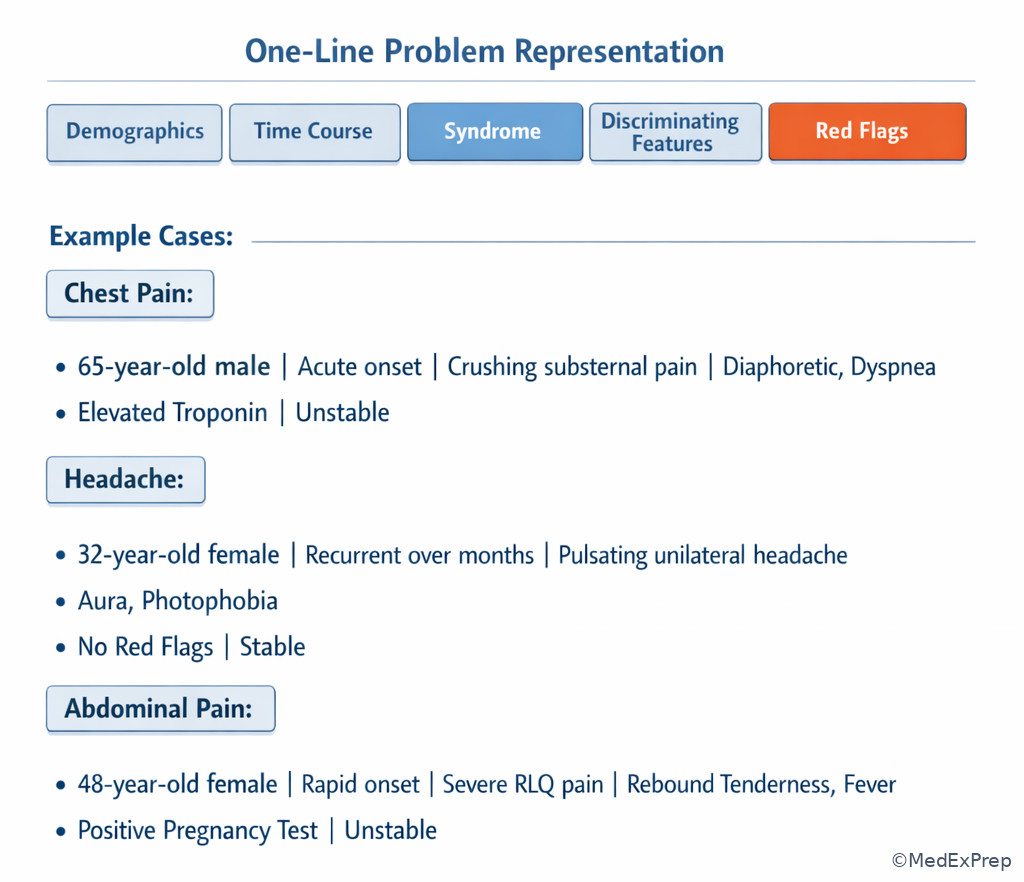
The decision conflict here is simple: should you summarize the case by listing facts or by building a clinically useful frame? On boards, you must choose the frame. The resolving rule is that a problem representation contains only information that changes disease probability or management. A useful structure is: demographics + acuity + syndrome + 2-4 discriminators + stability/red flag status. Example: “An older man with acute crushing exertional chest pain radiating to the left arm with diaphoresis and risk factors, currently hemodynamically stable.” That one sentence is already more useful than ten unranked facts.
WHY THIS IS TESTED: exam writers want to know whether you can identify the governing pattern before getting distracted by side details. Choose the representation that highlights timing and danger; reject summaries that overvalue incidental chronic diseases, irrelevant labs, or social details unless those details directly alter the differential or therapy.
Key rule: A good representation is not a transcript of the stem. It is a filtered summary built to answer the question being asked.
See Fig 1 and compare it to the one-line build process above.
B Worked example
A 68-year-old man with hypertension, type 2 diabetes, and chronic GERD presents with 45 minutes of substernal pressure that began while walking uphill. He reports nausea and diaphoresis. He mentions that he ate spicy food at lunch and had similar “burning” 6 months ago after pizza. Blood pressure is 146/90 mm Hg, pulse 96/min, and oxygen saturation 98% on room air. The task is not “name every possible cause of chest discomfort.” The task is to build the representation that will drive the next step.
Reasoning chain: Identify task → probable acute chest pain evaluation. Extract key facts → older patient, exertional onset, pressure quality, autonomic symptoms, CAD risk factors. Note noise → spicy food history and past GERD. Apply rule → exertional pressure plus diaphoresis outweighs the reflux clue. Eliminate distractor framing → “middle-aged man with heartburn after food” ignores timing and autonomic symptoms. Verify → patient is stable, so evaluation proceeds urgently but not through a collapse algorithm. Best representation: “Older man with acute exertional substernal pressure and autonomic symptoms concerning for acute coronary syndrome.”
C Exam trap
Common wrong answer: Summarizing the case as “chest burning after spicy food” and choosing reflux-driven management.
Why it is tempting: The stem includes a familiar, vivid clue linked to a common outpatient diagnosis.
Single clue that eliminates it: Exertional onset with diaphoresis makes ACS the governing frame until proven otherwise.
D Checkpoint
Question: A 24-year-old woman with asthma and migraines presents with acute pleuritic chest pain and shortness of breath 3 days after a long flight. She also reports mild epigastric burning after coffee. Which is the best problem representation?
- Young woman with reflux symptoms after dietary trigger
- Young woman with acute pleuritic chest pain and dyspnea after immobilization, concerning for pulmonary embolism
- Young woman with asthma flare causing isolated chest tightness
- Young woman with panic symptoms and nonspecific chest discomfort
Answer: B
- A: Tempting because the stem offers epigastric burning, but wrong because that clue does not govern the dangerous syndrome.
- B: Tempting and correct because the combination of acute pleuritic pain, dyspnea, and recent prolonged immobility sharply raises PE probability.
- C: Tempting because asthma can cause dyspnea, but wrong because pleuritic pain after a flight is a stronger discriminator than baseline asthma history.
- D: Tempting because young patients can have anxiety-related symptoms, but wrong because risk factor plus pleuritic pattern requires medical framing first.
Diagnose: Build a one-line summary using demographics, acuity, syndrome, and top discriminators. Order: Only after framing the syndrome should you choose targeted initial testing. Treat: If unstable, begin stabilization before broad workup. Refer/Escalate: Any red-flag presentation should prompt urgent team escalation or ED-level evaluation.
1.1.1.4 Semantic qualifiers: the fastest way to narrow the differential
A Explanation
The decision conflict is whether to think in vague symptom labels or in paired qualifiers that separate diseases. The resolving rule is that the best board differentials are built from semantic qualifiers: acute vs chronic, focal vs diffuse, unilateral vs bilateral, intermittent vs constant, painful vs painless, exertional vs positional, febrile vs afebrile, stable vs unstable. Instead of saying “abdominal pain,” say “acute severe right lower quadrant pain with fever and anorexia.” Instead of “weakness,” say “sudden focal unilateral weakness.” The qualifiers make the disease script visible.
WHY THIS IS TESTED: close distractors often share the same organ system and chief complaint. The exam separates them with one contrasting qualifier. Choose the option that matches the exact pattern; reject options that fit only a generic version of the complaint.
Memory anchor: Think ATLAS for every stem: Age, Time course, Location/syndrome, Alarm features, Semantic qualifiers. If one of these is missing from your summary, your representation is probably weak.
Exam takeaway: When answer choices look similar, the correct option is usually the one that matches the exact qualifier pattern in the stem.
flowchart TD
A[Chief complaint] --> B{Time course}
B -->|Acute| C[Emergency or inflammatory causes rise]
B -->|Chronic| D[Degenerative or functional causes rise]
C --> E{Focal or diffuse}
D --> F{Progressive or intermittent}
E -->|Focal| G[Local structural process]
E -->|Diffuse| H[Systemic process]
F -->|Progressive| I[Malignancy or chronic organ disease]
F -->|Intermittent| J[Functional or episodic disorder] See Fig 2 when you are stuck between two diagnoses in the same system.
B Worked example
A 31-year-old woman with obesity and polycystic ovary syndrome presents with headache. She has chronic migraines, but today’s pain began suddenly, reached maximal intensity within 1 minute, and is associated with vomiting and neck stiffness. She drank red wine last night and says that certain foods usually trigger her headaches. The tempting move is to classify this as another migraine because of age and history. The correct move is to apply qualifiers.
Reasoning chain: Identify task → decide whether this is benign recurrent headache or emergency headache. Extract key facts → sudden thunderclap onset, maximal at onset, neck stiffness, vomiting. Noise → migraine history and trigger foods. Apply rule → thunderclap plus meningeal signs changes the syndrome entirely. Eliminate distractors → migraine typically does not present as maximal at onset with meningismus. Verify → emergency neurovascular process must be considered first. Representation: “Young woman with sudden thunderclap headache and meningeal features concerning for subarachnoid hemorrhage.”
C Exam trap
Common wrong answer: Classifying sudden severe headache as migraine because the patient has prior migraines.
Why it is tempting: Test-takers anchor on past history and a common diagnosis they recognize.
Single clue that eliminates it: “Maximal intensity within 1 minute” is the pivot qualifier pointing to a dangerous secondary headache.
D Checkpoint
Question: A 72-year-old man with atrial fibrillation and hyperlipidemia develops sudden painless monocular vision loss while gardening. Which qualifier pair is most important for narrowing the differential?
- Chronic and bilateral
- Sudden and painless
- Intermittent and exertional
- Progressive and painful
Answer: B
- A: Tempting because chronic bilateral vision changes are common in older adults, but the stem is abrupt and unilateral.
- B: Tempting and correct because sudden painless monocular loss points toward retinal vascular or embolic disease.
- C: Tempting because exertional triggers matter in some syndromes, but vision loss here is defined more strongly by abrupt painless onset.
- D: Tempting because painful vision loss suggests important eye disease, but pain is absent and that absence is diagnostic leverage.
Diagnose: Translate symptoms into qualifier pairs immediately. Order: Choose tests that fit the qualified syndrome, not the broad complaint category. Treat: Dangerous qualifier patterns trigger urgent action even before diagnostic certainty. Refer/Escalate: Thunderclap headache, sudden focal deficits, sudden vision loss, or unstable vitals require immediate escalation.
- The most useful first qualifier pair for many emergency stems is ___ vs ___.
- True or False: A past history of a common benign condition should outweigh a new red-flag time course.
- Name the 3 highest-yield stem elements before labs: age, ___, and ___.
1.1.1.5 Signal vs noise: how to ignore distractors without missing danger
A Explanation
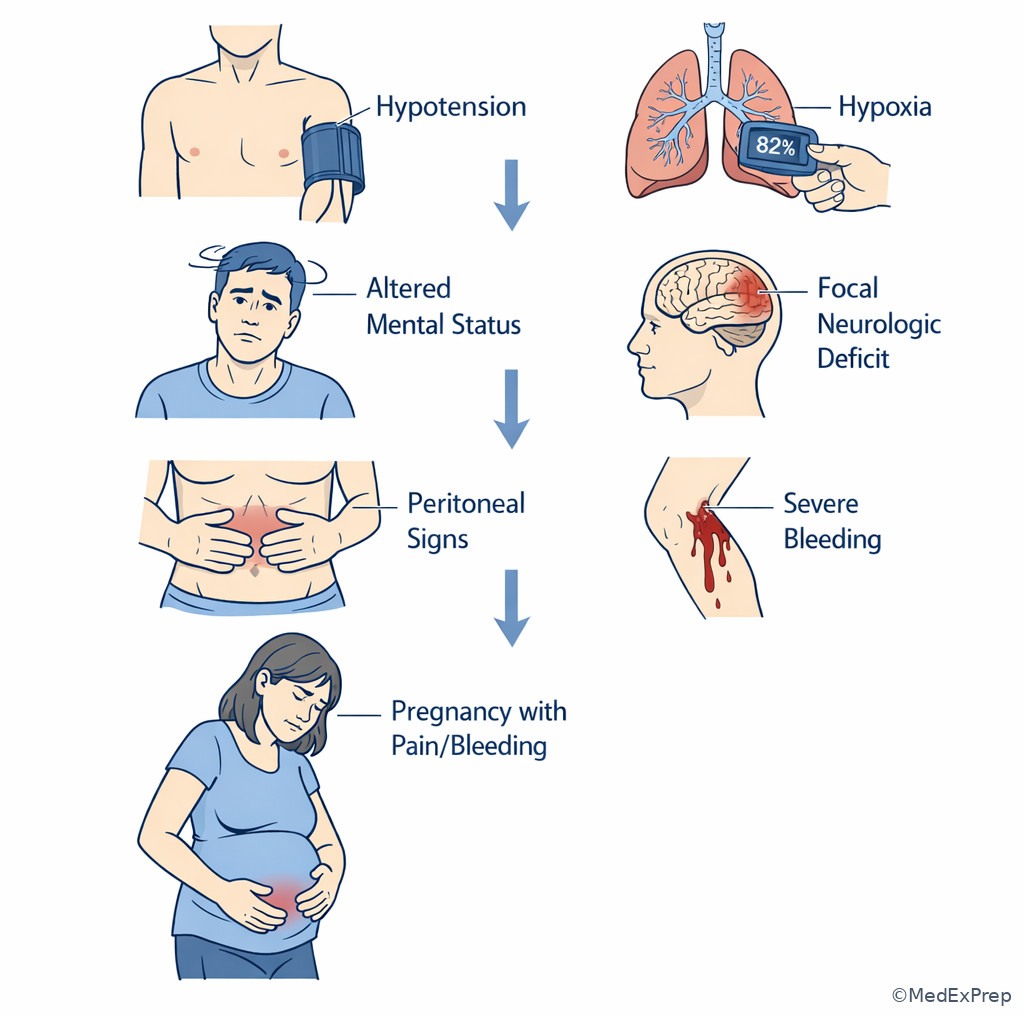
The decision conflict is whether every detail in the stem deserves equal weight. It does not. The resolving rule is that signal changes either disease probability or immediate action; noise adds realism but should not control the answer. Signal often includes vital signs, duration, abruptness, pregnancy status, medication use, immunosuppression, anticoagulation, focal deficits, peritoneal signs, bleeding, and toxic appearance. Noise often includes stable chronic diseases, remote surgeries, social history details without relevance, and familiar-but-non-governing symptoms.
WHY THIS IS TESTED: board stems are intentionally noisy. The exam rewards selective attention, not maximum memory dump. Choose the clue that alters safety or diagnosis. Reject details that merely sound medical but do not change the likely pathway.
Common pitfall: A distractor is not always false. It is often a true statement that is less important than the governing clue in this patient.
Exam takeaway: The correct answer usually follows the few clues that change urgency or probability, not the most colorful background detail.
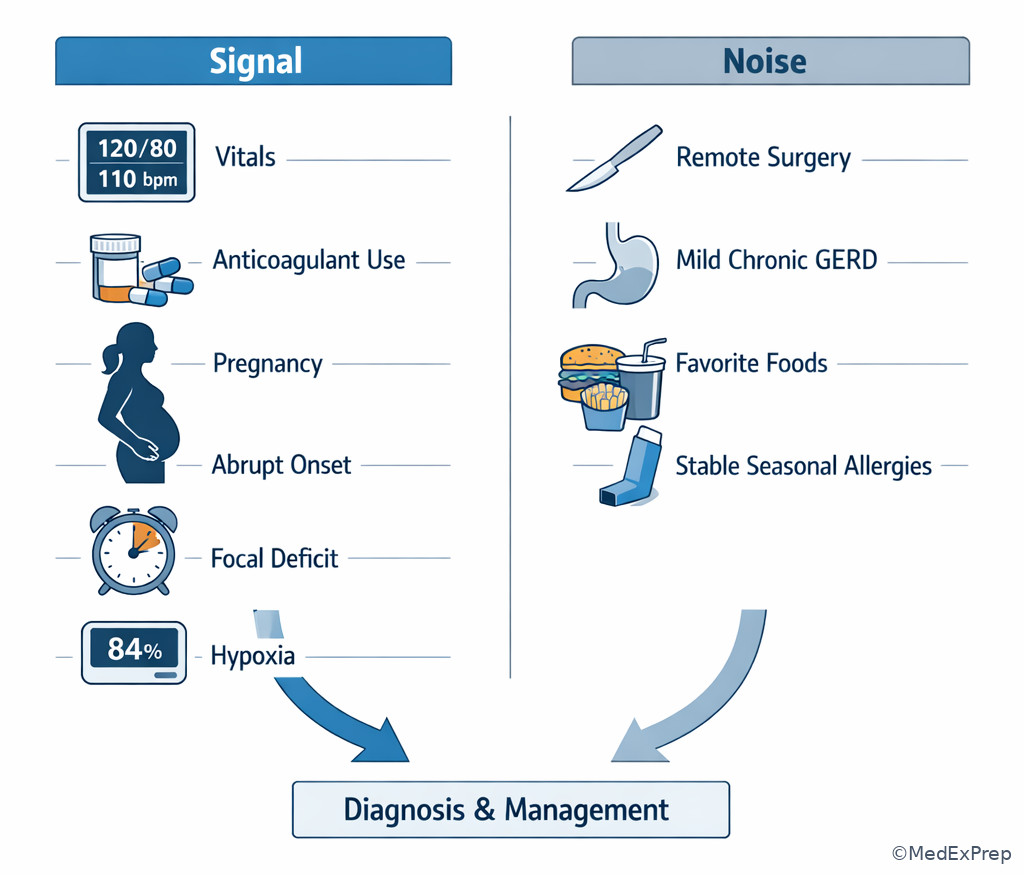
See Fig 3 for the visual distinction between data that should drive the answer and data that should be demoted.
B Worked example
A 59-year-old woman with osteoarthritis, hypothyroidism, and a remote cholecystectomy presents with acute shortness of breath. She takes estrogen therapy and returned from an international flight yesterday. She mentions mild chronic cough during spring allergy season and says her daughter recently had bronchitis. Heart rate is 118/min, respiratory rate 24/min, and oxygen saturation 89% on room air. The test-taker who overweights the cough or sick contact may chase infection. The strong representation comes from signal.
Reasoning chain: Identify task → acute dyspnea differential with management implications. Extract signal → tachycardia, hypoxemia, recent flight, estrogen use, acute onset. Demote noise → seasonal cough, family bronchitis, remote surgery. Apply rule → VTE risk factors plus hypoxia prioritize PE framing. Eliminate distractors → bronchitis does not explain hypoxemia and thrombotic risk as well. Verify → this patient may require urgent imaging pathway and anticoagulation planning depending on evaluation. Representation: “Middle-aged woman with acute hypoxemic dyspnea and VTE risk factors concerning for pulmonary embolism.”
C Exam trap
Common wrong answer: Overcalling pneumonia or bronchitis because of cough and sick contact.
Why it is tempting: Infectious diagnoses are common and feel familiar; the cough creates false coherence.
Single clue that eliminates it: Recent immobility plus estrogen exposure plus unexplained hypoxemia are stronger governing clues for PE.
D Checkpoint
Question: Which stem detail is most likely to be signal rather than noise in a patient with acute abdominal pain?
- He prefers spicy foods
- She had seasonal allergies as a teenager
- He has guarding and rebound tenderness
- She once had a normal colonoscopy 5 years ago
Answer: C
- A: Tempting because dietary details sometimes matter, but this one rarely determines emergent abdominal decisions.
- B: Tempting only because it is medical history, but it does not change acute abdominal risk framing.
- C: Tempting and correct because peritoneal signs immediately change urgency, workup, and surgical concern.
- D: Tempting because prior testing feels specific, but a remote normal study does not govern today’s acute abdomen.
Diagnose: Separate signal from background realism. Order: Let signal choose your first diagnostic branch. Treat: Do not delay urgent supportive care while investigating low-value noise. Refer/Escalate: If signal indicates hypoxia, shock, acute neurologic deficit, or peritonitis, escalate promptly.
1.1.1.6 Illness scripts: matching the representation to the right disease family
A Explanation
The decision conflict is whether to jump directly from a symptom to an answer or to compare the patient with stored disease patterns. The resolving rule is to use illness scripts: risk factors, time course, classic features, confirmatory tests, and expected next steps. Problem representation is the input; illness script matching is the engine. If the representation is “older smoker with chronic progressive cough, weight loss, and hemoptysis,” malignancy scripts rise. If it is “young patient with episodic wheeze triggered by exercise and allergens,” asthma scripts rise.
WHY THIS IS TESTED: the PANCE commonly offers four options from the same system that all share overlap. The best answer is the option whose entire illness script fits, not the one that matches a single symptom. Choose the diagnosis or action aligned with the full script; reject those that would require missing key expected findings.
High-Yield Connection: This concept overlaps with future systems-based topics across cardiology, pulmonology, GI, neurology, and infectious disease. On exam day, illness scripts are what let the same reasoning framework travel across organ systems.
Exam takeaway: The best answer is the option whose risk factors, timing, and findings all fit the same disease script.
flowchart TD A[Problem representation] --> B[Generate top scripts] B --> C[Risk factors match?] C --> D[Time course match?] D --> E[Signature findings match?] E --> F[Best-fit diagnosis] F --> G[Best next test or treatment]
See Fig 4 for the script-matching sequence that turns a one-line summary into an answer.
B Worked example
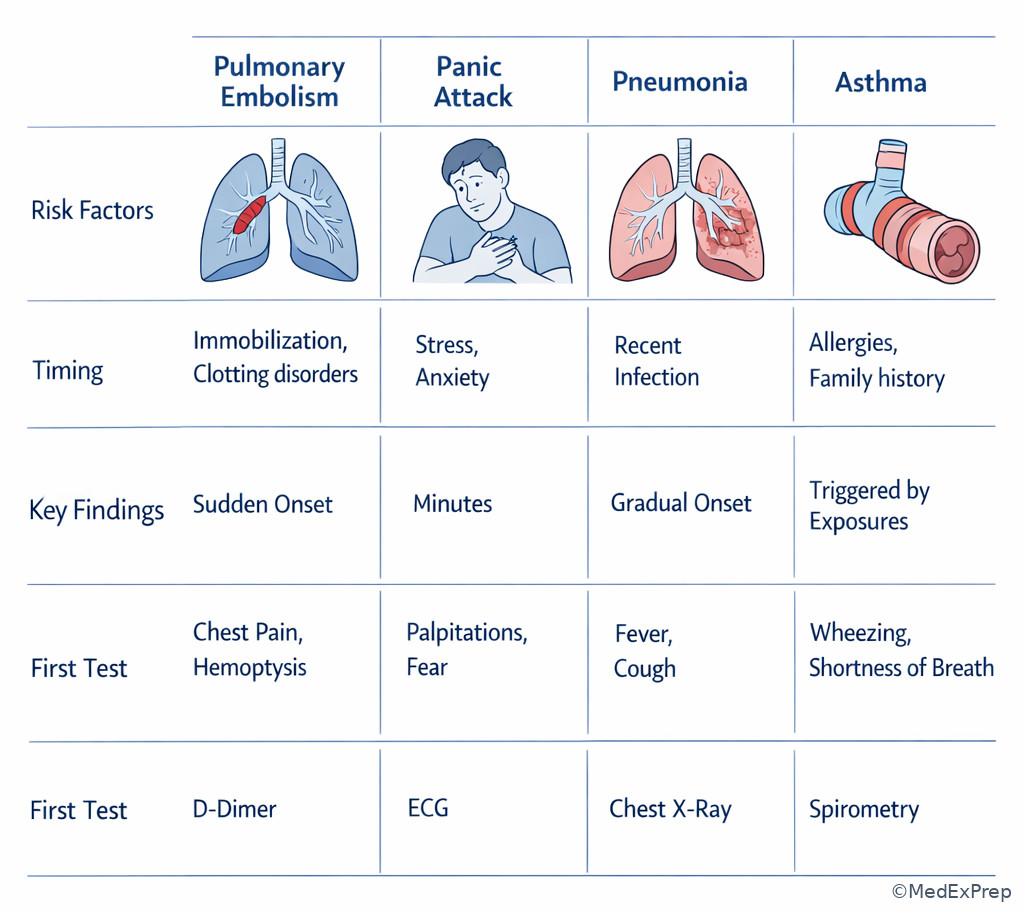
A 27-year-old woman with lupus and a recent delivery 3 weeks ago presents with pleuritic chest pain, dyspnea, and mild hemoptysis. She also reports a history of anxiety and says she “sometimes hyperventilates when stressed.” Temperature is 37.1°C, pulse 122/min, respiratory rate 26/min, and oxygen saturation 91% on room air. Her exam shows no wheezing. The differential could include panic attack, pneumonia, asthma, and PE, all of which may share dyspnea.
Reasoning chain: Identify task → choose the most likely diagnosis and likely next step. Extract key facts → postpartum state, autoimmune disease, pleuritic pain, tachycardia, hypoxemia, hemoptysis. Apply illness scripts → PE script fits risk context plus cardiorespiratory pattern. Eliminate distractors → panic can mimic dyspnea but should not explain hypoxemia; asthma would more likely show wheeze; pneumonia often brings fever or focal infectious findings. Verify → the script supports urgent PE evaluation. The case is won by script fit, not by symptom overlap.
C Exam trap
Common wrong answer: Panic attack.
Why it is tempting: Anxiety can cause tachypnea, chest discomfort, and dyspnea in young adults.
Single clue that eliminates it: Objective hypoxemia with postpartum thrombotic risk makes a cardiopulmonary script much stronger than a psychiatric one.
D Checkpoint
Question: A 63-year-old smoker with 15-pound weight loss, persistent cough, and streaks of blood in sputum presents for evaluation. Which approach best uses illness scripts?
- Choose acute bronchitis because cough is the main complaint
- Choose GERD because cough can occur with reflux
- Prioritize lung malignancy because age, smoking history, weight loss, and hemoptysis fit the script
- Prioritize asthma because cough can be chronic
Answer: C
- A: Tempting because bronchitis is common, but the chronic constitutional features are a mismatch.
- B: Tempting because reflux can cause chronic cough, but it does not account well for hemoptysis and weight loss.
- C: Tempting and correct because the entire illness script aligns with malignancy risk and presentation.
- D: Tempting because chronic cough can suggest asthma, but smoking, weight loss, and hemoptysis are stronger discriminators elsewhere.
- The single best phrase to describe disease-pattern matching is the ___ script.
- True or False: The correct option may share fewer total symptoms than a distractor but still be right if the key discriminator fits better.
- Name the 3 script elements most likely to break a tie between close diagnoses: risk factors, time course, and ___.
Diagnose: Compare the patient against 2-3 leading scripts within the same syndrome. Order: Select the initial test that best confirms the top script or rules out the dangerous competitor. Treat: Begin first-line supportive or syndrome-based care when appropriate. Refer/Escalate: If the leading script implies emergent disease, escalate while confirming.
1.1.1.7 From representation to best next step: diagnosis is not always the immediate task
A Explanation
The decision conflict is whether the stem is asking for the diagnosis, the test, or the first action. The resolving rule is that your representation must feed the specific task. A correct diagnosis with the wrong next step still loses points. For example, “likely ectopic pregnancy” should immediately cue pregnancy test confirmation if status is unknown, hemodynamic assessment, urgent ultrasound pathway if stable, and emergent OB/GYN escalation if unstable. Likewise, “probable sepsis” should cue stabilization and cultures/antibiotics, not a leisurely broad outpatient differential.
WHY THIS IS TESTED: exam writers frequently give enough clues to suspect the diagnosis but then ask for the next action that improves safety. Choose the action that logically follows from the representation and urgency. Reject elegant but delayed diagnostics when instability or a time-sensitive treatment is the true priority.
Memory anchor: After the one-liner, ask “DDV” — Diagnose what syndrome this is, Decide if stable, Verify the next step asked by the stem.
Exam takeaway: The problem representation should drive either stabilization, targeted testing, or first-line treatment depending on the question asked.
flowchart LR
A[Problem representation] --> B{What is asked?}
B -->|Most likely diagnosis| C[Choose best-fit illness script]
B -->|Best test| D[Choose test that changes management]
B -->|Best next step| E{Stable?}
E -->|No| F[Stabilize and escalate]
E -->|Yes| G[Guideline-based initial evaluation or treatment] See Fig 5 for the transition from representation to action. This directly sets up the upcoming topic Best Next Step Logic.
B Worked example
A 25-year-old woman with no major medical history presents with lower abdominal pain and light vaginal bleeding. She is 7 weeks late for menses and has had one episode of near-syncope. She also mentions dysuria for 2 days. Blood pressure is 84/52 mm Hg, pulse 128/min. The stem asks for the most appropriate next step. The representation is “reproductive-age woman with presumed early pregnancy, abdominal pain, bleeding, and hemodynamic instability.” The diagnosis may be ectopic pregnancy, but the asked task is action.
Reasoning chain: Identify task → next step, not just diagnosis. Extract key facts → unstable vitals, pregnancy-related symptoms, abdominal pain, bleeding. Noise → dysuria may tempt UTI framing. Apply rule → unstable suspected ectopic requires immediate resuscitation and urgent OB/GYN/surgical escalation, not outpatient urine testing or delayed imaging. Eliminate distractors → transvaginal ultrasound is appropriate in stable patients, but not before addressing instability. Verify → patient safety determines the answer.
C Exam trap
Common wrong answer: Ordering a confirmatory ultrasound first.
Why it is tempting: Ultrasound is indeed a key diagnostic test in suspected ectopic pregnancy.
Single clue that eliminates it: Hypotension and tachycardia make stabilization and emergent escalation the immediate priority.
D Checkpoint
Question: A board stem strongly suggests meningitis, but the patient is hypotensive, febrile, and altered. What should the problem representation prompt first when the question asks for best next step?
- Detailed outpatient differential diagnosis
- Immediate stabilization and urgent empiric management pathway
- Delayed treatment until full culture confirmation returns
- Reassurance because infectious symptoms are common
Answer: B
- A: Tempting because careful differential reasoning matters, but instability outranks diagnostic completeness.
- B: Tempting and correct because altered mental status and hypotension signal a time-sensitive emergency.
- C: Tempting because cultures help confirm the diagnosis, but waiting would be unsafe.
- D: Tempting only if the severity is ignored; the stem’s red flags make reassurance inappropriate.
Diagnose: Use the one-liner to define syndrome and severity. Order: Choose targeted initial tests only after checking whether the patient is stable. Treat: Begin time-sensitive first-line care when delay is harmful. Refer/Escalate: Unstable patients, suspected surgical emergencies, and time-critical neurologic or cardiopulmonary cases require immediate escalation.
Exam Traps & Differentiators
Most common wrong answer and why: The most common mistake is selecting the option tied to the most memorable clue rather than the option supported by the whole representation. For example, “burning after spicy food” can feel more concrete than “exertional chest pressure,” but the latter governs the syndrome.
| Looks similar but isn't | Tempting overlap | Single discriminator | Use this frame instead |
|---|---|---|---|
| Panic attack vs pulmonary embolism | Dyspnea, tachycardia, chest discomfort | Hypoxemia or VTE risk factor | Acute cardiopulmonary threat until excluded |
| Migraine vs subarachnoid hemorrhage | Severe headache, nausea, vomiting | Thunderclap onset/maximal at onset | Emergency headache pathway |
| GERD vs ACS | Chest burning or discomfort | Exertional pattern or diaphoresis | Acute coronary syndrome frame |
| Bronchitis vs PE | Cough, dyspnea, chest discomfort | Unexplained hypoxemia with thrombotic risk | PE evaluation frame |
| UTI vs ectopic pregnancy | Pelvic pain, urinary symptoms | Amenorrhea plus bleeding or instability | Pregnancy emergency frame |
| Tension headache vs meningitis/SAH | Headache and discomfort | Fever, neck stiffness, altered mental status, or thunderclap timing | Emergency neuro/infectious frame |
Exam takeaway: When two answers share symptoms, one stem detail usually separates the safe choice from the tempting trap.
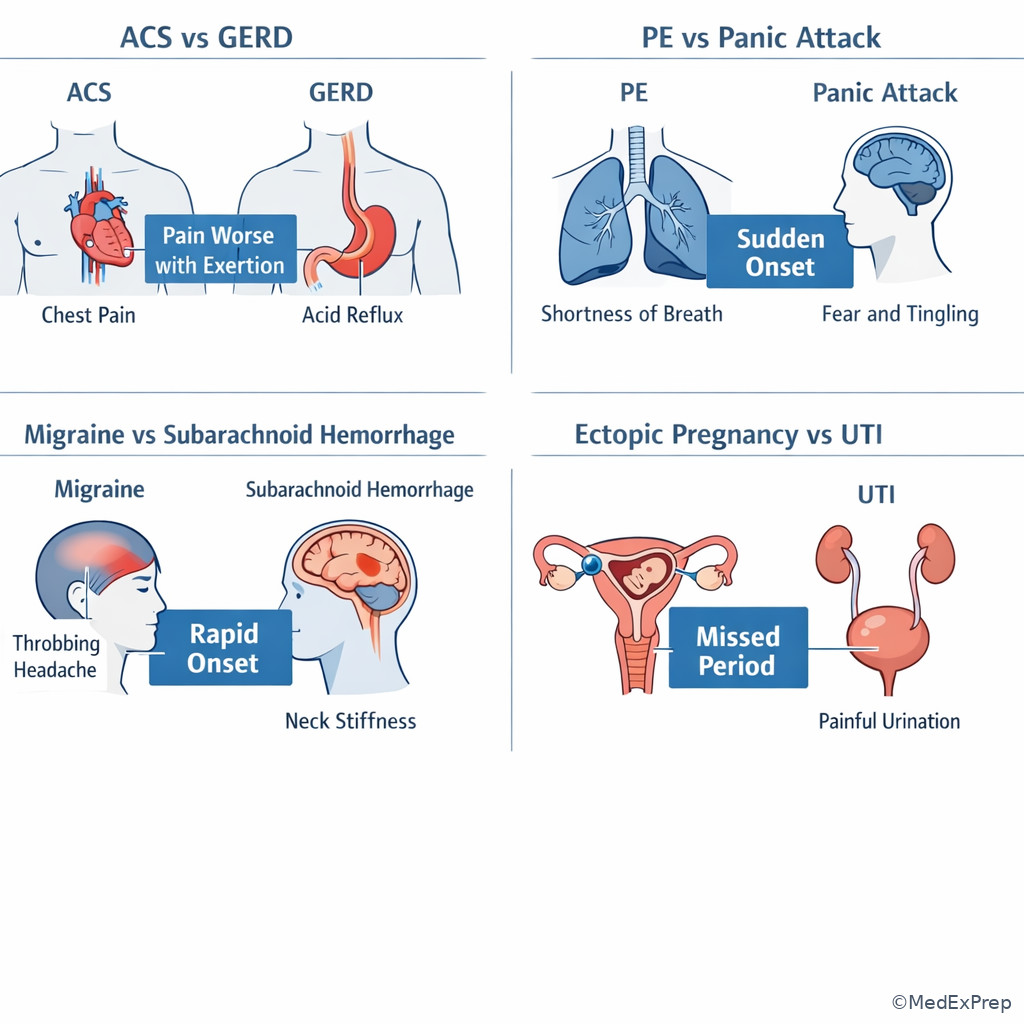
See Fig 6 for classic close-call differential pairs you will repeatedly see across this course.
- If the stem says sudden, severe, maximal at onset → think dangerous secondary process before benign recurrent syndrome.
- If the stem says hypotension, hypoxia, altered mental status, or peritoneal signs → think stabilization and escalation before elegant workup.
- If the stem says postpartum, immobilization, estrogen use, active cancer, or unilateral leg swelling → think VTE framing when dyspnea or pleuritic pain appears.
- If the stem says exertional symptoms with autonomic features → think ischemic or dangerous cardiopulmonary disease over benign outpatient explanations.
- If the stem says amenorrhea plus pelvic pain or vaginal bleeding → think pregnancy-related emergency until proven otherwise.
- If the stem says focal deficit or sudden monocular vision loss → think vascular/neuro-ophthalmic emergency, not “just a migraine” or “just anxiety.”
Common traps & distractors: Related traps will recur in upcoming topics. In Board Vignette Clues, you will practice ranking clue importance; in Best Next Step Logic, you will practice acting correctly after identifying the governing frame. A frequent confusable pair is “correct diagnosis, wrong immediate action.”
Tables
| Reference table: semantic qualifiers | Qualifier pair | Why it matters | Classic example |
|---|---|---|---|
| Time course | Acute vs chronic | Changes urgency and disease family | Acute chest pain vs chronic reflux |
| Pattern | Intermittent vs constant | Helps distinguish episodic from ongoing pathology | Biliary colic vs peritonitis |
| Distribution | Focal vs diffuse | Local lesion vs systemic process | Focal deficit vs generalized weakness |
| Laterality | Unilateral vs bilateral | Narrows vascular, ophthalmic, and renal causes | Monocular vision loss vs bilateral blurring |
| Character | Painful vs painless | Often separates inflammatory from ischemic or embolic disease | Painful red eye vs painless vision loss |
| Severity | Stable vs unstable | Determines whether to stabilize first | Stable PE workup vs shock pathway |
| Comparison table | Weak representation | Strong representation |
|---|---|---|
| Chest pain | Man with chest discomfort and heartburn history | Older man with acute exertional substernal pressure and diaphoresis, stable but concerning for ACS |
| Headache | Woman with headache and vomiting | Young woman with thunderclap headache, maximal at onset, vomiting, and neck stiffness |
| Dyspnea | Woman with cough and shortness of breath | Middle-aged woman with acute hypoxemic dyspnea, tachycardia, recent flight, and estrogen exposure |
| Abdominal pain | Patient with belly pain and nausea | Reproductive-age woman with amenorrhea, pelvic pain, vaginal bleeding, and hemodynamic instability |
| Vision complaint | Older man with eye problem | Older man with sudden painless monocular vision loss and embolic risk factors |
| Differential/classification table | Complaint category | Dangerous frame | Common benign trap | Discriminator |
|---|---|---|---|---|
| Chest pain | ACS/PE/aortic catastrophe | GERD/musculoskeletal pain | Exertional onset, diaphoresis, risk factors, hypoxia | |
| Headache | SAH/meningitis/temporal arteritis | Migraine/tension headache | Thunderclap timing, fever, neck stiffness, vision loss | |
| Abdominal pain | Appendicitis, perforation, ectopic, ischemia | Dyspepsia, constipation | Peritoneal signs, bleeding, instability, severe focal pain | |
| Dyspnea | PE, pneumothorax, heart failure, sepsis | Anxiety, viral bronchitis | Hypoxemia, unilateral findings, thrombotic risk, edema, fever with toxicity | |
| Neurologic complaint | Stroke, spinal cord compression, CNS infection | Benign vertigo, anxiety, chronic neuropathy | Sudden focal deficit, bowel/bladder change, fever, altered mental status |
Exam takeaway: A one-line summary should contain demographics, acuity, syndrome, discriminators, and stability status.
Exam takeaway: Unstable vitals and danger signs should immediately reshape the problem representation and next step.
Exam takeaway: Compare disease patterns side by side to identify the single feature that breaks the tie.
Algorithm / Approach
Memory anchor: Use IPSMAV — Identify task, Patient stability, Summarize, Match scripts, Act, Verify.
Rapid Review
- Problem representation → one-line filtered summary, not a stem rewrite
- Semantic qualifiers → paired descriptors that collapse the differential fast
- Signal → clue that changes urgency, probability, or treatment
- Noise → realistic detail without decision value in this case
- Illness script → risk factors plus timing plus signature findings
- Best next step → depends on the task verb, not just the diagnosis
- Hypotension with suspected ectopic → resuscitate and escalate before routine imaging
- Thunderclap headache → dangerous secondary cause until proven otherwise
- Exertional chest pressure with diaphoresis → ACS frame beats reflux history
- Dyspnea with VTE risk and hypoxemia → PE frame beats anxiety label
- Sudden painless monocular vision loss → embolic/vascular frame beats chronic eye disease
- Peritoneal signs → surgical abdomen frame, not functional GI explanation
- Past history can mislead → new time course and severity usually matter more
- Close-call options → find the single missing expected feature
Self-check quiz
1. A 66-year-old man with hypertension and hyperlipidemia presents with 30 minutes of exertional substernal pressure and diaphoresis. He also reports chronic reflux after large meals. Which problem representation is most appropriate?
- Older man with heartburn after meals and chronic GERD
- Older man with acute exertional chest pressure and autonomic symptoms concerning for ACS
- Older man with nonspecific chest discomfort and probable anxiety
- Older man with chronic musculoskeletal chest pain
2. A 29-year-old woman with prior migraines presents with sudden severe headache that reached maximal intensity immediately and is associated with vomiting and neck stiffness. Which semantic qualifier pair most strongly changes the differential?
- Chronic and recurrent
- Unilateral and throbbing
- Sudden and maximal at onset
- Stress-related and intermittent
3. A 58-year-old woman with obesity and osteoarthritis presents with acute dyspnea. She returned from a transatlantic flight yesterday and takes estrogen therapy. She mentions that her grandson had a cold. Pulse is 116/min and oxygen saturation is 90% on room air. Which stem detail should receive the greatest weight in the problem representation?
- Grandson with a recent cold
- Acute dyspnea with hypoxemia, recent flight, and estrogen use
- History of osteoarthritis
- Obesity alone without time course
4. A 24-year-old woman presents with lower abdominal pain and vaginal spotting. Her last menstrual period was 8 weeks ago. Blood pressure is 82/48 mm Hg and pulse is 132/min. The stem asks for the most appropriate next step. Which approach is best?
- Treat empirically for cystitis because dysuria can accompany pelvic pain
- Obtain outpatient pelvic ultrasound before any other action
- Frame as unstable possible ectopic pregnancy and initiate urgent stabilization with escalation
- Reassure because early pregnancy bleeding is often benign
5. A 72-year-old man with atrial fibrillation develops sudden painless loss of vision in one eye. Which is the most likely high-yield problem representation?
- Older man with chronic bilateral visual decline from cataracts
- Older man with sudden painless monocular vision loss and embolic risk factors
- Older man with painful red eye from acute glaucoma
- Older man with recurrent migraine aura
6. A 34-year-old woman 2 weeks postpartum presents with pleuritic chest pain, dyspnea, and anxiety. She has a history of panic attacks and says this feels similar. Pulse is 124/min and oxygen saturation is 91% on room air. Which answer best explains why pulmonary embolism should outrank panic attack in the problem representation?
- Both conditions can cause tachycardia, but postpartum status and hypoxemia strongly favor PE
- Because panic attacks never cause dyspnea
- Because postpartum patients cannot have psychiatric symptoms
- Because pleuritic chest pain is diagnostic of PE in all cases
7. A 61-year-old smoker presents with cough for 3 months, 10-pound weight loss, and blood-streaked sputum. He also reports occasional nocturnal reflux. Which is the best use of illness scripts?
- Choose GERD because cough can be reflux-related
- Choose acute bronchitis because cough is common in outpatient medicine
- Prioritize lung malignancy because the full risk-and-symptom script fits best
- Choose asthma because chronic cough may occur without wheeze
8. A 43-year-old man with diabetes presents with abdominal pain, fever, and vomiting. He notes that spicy food worsened his symptoms after dinner. On exam he has guarding and rebound tenderness. Which principle should dominate the problem representation and next step?
- Dietary triggers are the strongest clue in abdominal pain stems
- Peritoneal signs are signal that override benign GI explanations
- Remote outpatient history should outweigh physical examination
- Vomiting without diarrhea usually indicates a functional disorder
Answer key
1.1.1.8 1. Question 1 Answer: B
Correct answer mechanism-to-treatment logic: Exertional substernal pressure with diaphoresis in an older patient with vascular risk factors fits an ischemic chest pain script. The problem representation should foreground the dangerous cardiology frame, which then guides urgent ECG/troponin-based evaluation and ACS management rather than reflux treatment. This is the classic example of dangerous signal overruling a familiar benign clue. Sources: AHA/ACC chest pain guidance; Harrison’s Principles of Internal Medicine.
- A: Tempting because GERD is common and the patient mentions reflux. Incorrect because the discriminating stem clue is exertional pressure with diaphoresis, not meal-related burning. Single clue: exertional onset with autonomic symptoms.
- B: Tempting and correct because it captures age, acuity, syndrome, and dangerous discriminators in one line. Single clue: acute exertional chest pressure plus diaphoresis.
- C: Tempting because chest discomfort can be nonspecific, but incorrect because nothing in the stem supports anxiety better than ACS. Single clue: objective risk context and classic symptom pattern.
- D: Tempting because musculoskeletal chest pain is common, but incorrect because chronic reproducible pain is not described. Single clue: autonomic symptoms are atypical for simple chest wall pain.
1.1.1.9 2. Question 2 Answer: C
Correct answer mechanism-to-treatment logic: Thunderclap timing—sudden and maximal at onset—is the key semantic qualifier that transforms “headache” into a possible hemorrhagic emergency script. This changes the initial diagnostic pathway and urgency immediately. Sources: Harrison’s Principles of Internal Medicine; standard emergency neurology teaching.
- A: Tempting because migraine is often chronic and recurrent, but incorrect because the stem explicitly breaks that pattern. Single clue: new sudden maximal onset.
- B: Tempting because unilateral throbbing suggests migraine, but incorrect because the timing is more important than the pain character here. Single clue: thunderclap onset outweighs typical migraine descriptors.
- C: Tempting and correct because sudden onset reaching peak intensity immediately is the emergency discriminator. Single clue: maximal at onset.
- D: Tempting because stress can trigger benign headaches, but incorrect because the stem includes meningeal features and dangerous timing. Single clue: neck stiffness with abrupt onset.
1.1.1.10 3. Question 3 Answer: B
Correct answer mechanism-to-treatment logic: Acute dyspnea plus hypoxemia with recent prolonged travel and estrogen exposure should dominate the representation because these clues directly increase PE probability and alter urgent testing choices. Signal beats infectious background noise. Sources: CHEST/standard VTE guidance; Harrison’s Principles of Internal Medicine.
- A: Tempting because sick contacts often appear in respiratory stems, but incorrect because this does not explain thrombotic risk and hypoxemia as well. Single clue: recent flight plus estrogen use.
- B: Tempting and correct because it combines the highest-value signal data into a PE-oriented frame. Single clue: acute hypoxemia with VTE risks.
- C: Tempting because comorbidities matter, but osteoarthritis has low immediate decision value here. Single clue: it does not change acute dyspnea urgency.
- D: Tempting because obesity is a risk factor, but alone it is weaker than the full thrombotic pattern and time course. Single clue: acute onset plus hypoxemia is more decisive.
1.1.1.11 4. Question 4 Answer: C
Correct answer mechanism-to-treatment logic: In a reproductive-age patient with amenorrhea, pain, spotting, and shock, the representation should trigger unstable ectopic pregnancy until proven otherwise. The question asks for best next step, so immediate stabilization and emergent escalation outrank routine imaging or outpatient treatment. Sources: standard obstetric emergency practice; Harrison’s Principles of Internal Medicine.
- A: Tempting because urinary symptoms can coexist, but incorrect because cystitis does not explain shock in this context. Single clue: hypotension with amenorrhea and bleeding.
- B: Tempting because ultrasound is diagnostically important, but incorrect because unstable patients require resuscitation first. Single clue: BP 82/48 mm Hg.
- C: Tempting and correct because it matches both the representation and the task asked by the stem. Single clue: hemodynamic instability.
- D: Tempting because some early pregnancy bleeding is benign, but incorrect because the vital signs make reassurance unsafe. Single clue: tachycardia with hypotension.
1.1.1.12 5. Question 5 Answer: B
Correct answer mechanism-to-treatment logic: Sudden painless monocular vision loss in a patient with atrial fibrillation fits an embolic retinal vascular script. The representation must reflect abruptness, laterality, pain status, and embolic risk. Sources: Harrison’s Principles of Internal Medicine; standard ophthalmic emergency teaching.
- A: Tempting because cataracts are common in older adults, but incorrect because cataracts cause gradual, not sudden, decline and are usually bilateral over time. Single clue: sudden onset.
- B: Tempting and correct because it captures the highest-yield discriminators. Single clue: sudden painless monocular loss with AF.
- C: Tempting because glaucoma is urgent and vision-threatening, but incorrect because acute angle-closure glaucoma is typically painful with a red eye. Single clue: painless presentation.
- D: Tempting because migraine aura can cause transient visual symptoms, but incorrect because embolic risk and the symptom pattern fit better elsewhere. Single clue: atrial fibrillation plus monocular deficit.
1.1.1.13 6. Question 6 Answer: A
Correct answer mechanism-to-treatment logic: Panic attack and PE can both cause dyspnea and tachycardia, but postpartum hypercoagulability and objective hypoxemia sharply increase PE probability. The correct reasoning uses a close-call differential and picks the discriminator. Sources: VTE guideline principles; Harrison’s Principles of Internal Medicine.
- A: Tempting and correct because it explains the overlap while identifying the key discriminator. Single clue: postpartum status plus oxygen saturation 91%.
- B: Tempting because it seems to separate psychiatric from medical disease, but incorrect because panic attacks can indeed cause dyspnea. Single clue: absolute language “never” is false.
- C: Tempting because postpartum physiology matters, but incorrect because psychiatric symptoms can still occur postpartum. Single clue: the issue is probability, not impossibility.
- D: Tempting because pleuritic pain is classically associated with PE, but incorrect because it is not independently diagnostic. Single clue: “in all cases” overstates the evidence.
1.1.1.14 7. Question 7 Answer: C
Correct answer mechanism-to-treatment logic: Chronic cough, smoking history, weight loss, and hemoptysis together create a malignancy script. Illness scripts require full-pattern matching, not single-symptom anchoring. Sources: Harrison’s Principles of Internal Medicine; standard pulmonary oncology teaching.
- A: Tempting because reflux can cause chronic cough, but incorrect because it does not explain weight loss and hemoptysis nearly as well. Single clue: constitutional symptoms with blood-streaked sputum.
- B: Tempting because bronchitis is common, but incorrect because a 3-month course with weight loss is not the expected script. Single clue: chronicity plus weight loss.
- C: Tempting and correct because the entire risk-and-symptom package fits malignancy best. Single clue: smoker with hemoptysis and weight loss.
- D: Tempting because asthma may present with cough, but incorrect because the absence of the expected script features and presence of malignancy clues argue against it. Single clue: hemoptysis with weight loss.
1.1.1.15 8. Question 8 Answer: B
Correct answer mechanism-to-treatment logic: Guarding and rebound are peritoneal signs, which are high-value signal in abdominal pain. They immediately increase concern for a surgical abdomen and change urgency, workup, and consultation needs. Sources: Harrison’s Principles of Internal Medicine; standard acute abdomen teaching.
- A: Tempting because spicy food is a classic GI distractor, but incorrect because it does not outrank peritoneal signs. Single clue: guarding and rebound.
- B: Tempting and correct because it names the principle of signal dominance in a dangerous abdomen. Single clue: peritoneal findings on exam.
- C: Tempting because history matters, but incorrect because the physical examination here is more decision-critical. Single clue: acute peritoneal exam changes management.
- D: Tempting because vomiting patterns can suggest GI categories, but incorrect because it ignores the most dangerous exam feature. Single clue: rebound tenderness signals more than a functional disorder.