Why it matters
- The NCLEX does not reward isolated trivia; it rewards safe clinical judgment within entry-level RN scope.
- Many wrong answers are attractive because they are reasonable healthcare actions but are not the best nursing priority for the stem.
- If you know the test plan structure, you can quickly identify whether the item is asking you to assess, intervene, teach, delegate, monitor, document, or escalate.
- Understanding structure early prevents two major failures: overthinking like a provider and under-prioritizing safety threats.
Key Terms & Must-Know Facts
1.1.1.1 Key terms
- Test plan: official framework describing what the NCLEX-RN measures.
- Client needs: major content categories used to organize exam coverage.
- Integrated processes: nursing process, caring, communication/documentation, teaching/learning, culture/spirituality.
- CJMM: Clinical Judgment Measurement Model used to structure reasoning.
- Recognize cues: identify relevant findings from the stem.
- Analyze cues: connect findings to likely risks/problems.
- Prioritize hypotheses: decide which problem is most urgent.
- Generate solutions: identify safe options within RN scope.
- Take action: choose the highest-priority nursing action.
- Evaluate outcomes: determine whether the action worked or requires escalation.
- RN scope: assessment, intervention, teaching, monitoring, documentation, delegation, escalation.
- Provider-only action: prescribing, diagnosing, or independently selecting medical treatment.
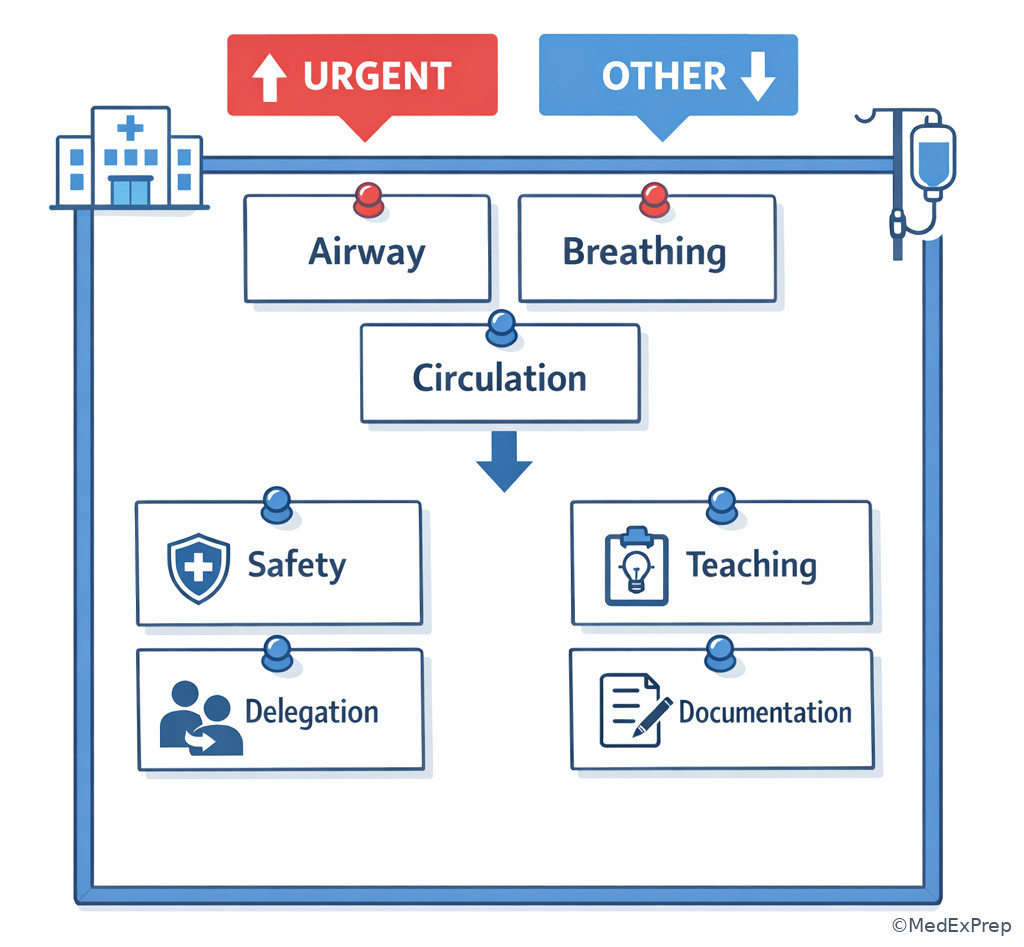
- Priority framework: ABCs, unstable before stable, acute before chronic, actual before potential, safety before convenience.
1.1.1.2 Must-know facts
- The NCLEX tests safe entry-level RN practice, not independent provider decision-making.
- The exam is broad; do not invent unofficial numeric weights when not provided.
- Every question can be approached as a task: assess, act, teach, monitor, delegate, document, or report.
- When a stem includes deterioration, safety risk usually outranks education and routine comfort measures.
- Delegation never transfers RN accountability for assessment, judgment, or evaluation.
- A tempting option may be correct in another situation but wrong for this priority.
- NCLEX items often include noise: chronic disease history, mildly abnormal labs, or familiar diagnoses that are not the deciding clue.
- The best answer usually matches both priority framework and scope of practice.
Exam takeaway: Sort every stem into test-plan category, clinical judgment step, and RN action type before choosing an answer.
flowchart TD
A[Read stem] --> B[Identify task]
B --> C{What is being tested?}
C --> D[Client need domain]
C --> E[Integrated process]
C --> F[CJMM step]
D --> G[Choose RN-safe action]
E --> G
F --> G
G --> H[Verify with priority framework] Exam takeaway: Visual grouping of domains helps you stop studying by random disease lists and start studying by tested decision patterns.
Core content
1.1.1.3 Foundational map: what the NCLEX test plan is actually organizing
A Explanation
The first decision conflict is simple but crucial: should you study and answer questions by body system alone, or by the exam's tested nursing roles? Choose the test-plan structure. Reject a pure disease-list approach when the answer options are all nursing actions, not diagnoses. The single rule that resolves this conflict: if the item asks what the RN should do next, it is testing a client need plus integrated process, even when the disease label seems prominent.
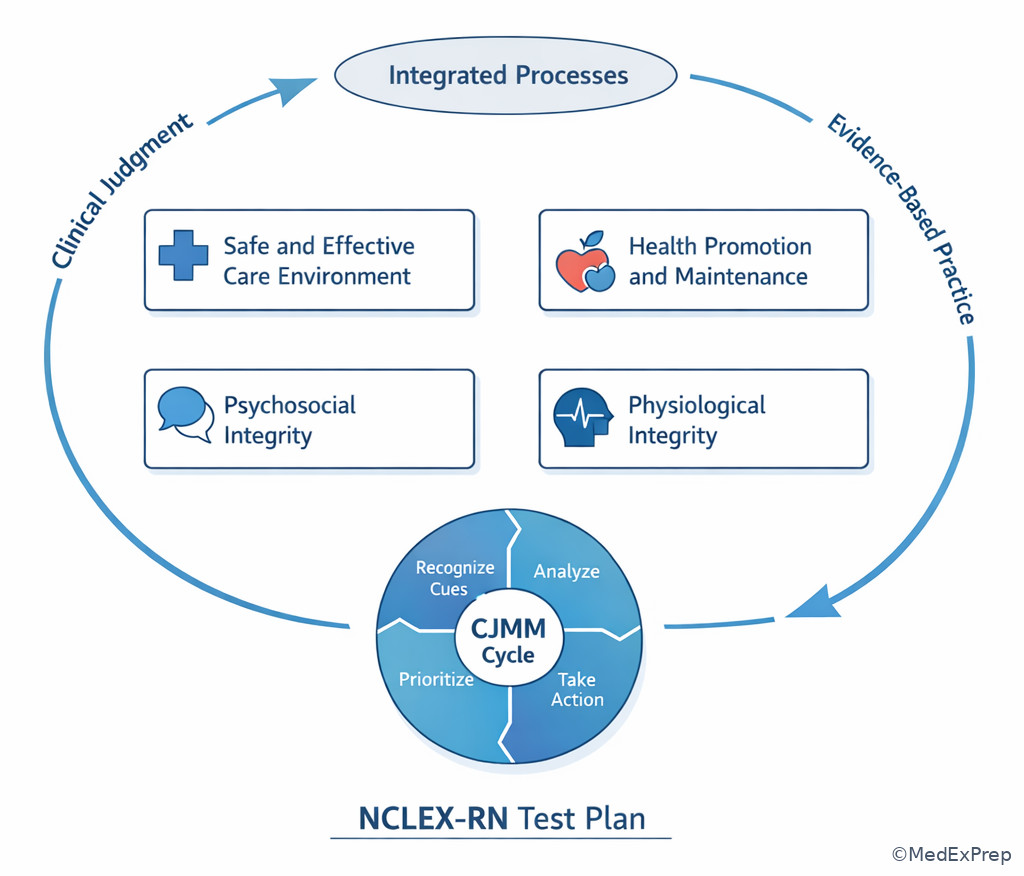
WHY THIS IS TESTED: Students often know the disease but miss the question type. The NCLEX wants to know whether you can provide safe, effective, client-centered care within RN scope across settings. See Fig 1.
The major client need groupings are broad on purpose. They are not meant to trap you into memorizing bureaucratic labels; they are meant to make your preparation comprehensive. Safe and Effective Care Environment captures management, delegation, safety, and infection control. Health Promotion and Maintenance covers development, prevention, and expected teaching. Psychosocial Integrity tests therapeutic communication, coping, and behavioral safety. Physiological Integrity spans basic care, medications, reduction of risk potential, and adaptation to illness.
Integrated processes cut across all of them. A postpartum teaching item, a sepsis priority item, and a mental health therapeutic-communication item all still require nursing process, communication, and teaching. That is why many questions feel mixed. They are supposed to.
B Worked example
A 72-year-old client on a medical-surgical unit has type 2 diabetes, chronic kidney disease, and osteoarthritis. The client reports new shortness of breath while ambulating to the bathroom. Oxygen saturation is 88% on room air, respiratory rate 28/min, blood glucose 214 mg/dL, and the client asks whether a home walker will be covered by insurance after discharge. Which framework should guide the RN's answer selection first?
Reasoning chain: Identify task - this is a priority nursing action item, not a discharge-planning item. Extract key facts - new dyspnea, low oxygen saturation, tachypnea. Apply rule - classify under physiological integrity and safety using ABCs. Eliminate distractors - diabetes teaching and discharge equipment questions are real nursing issues but not the current priority. Verify - the correct action category is immediate respiratory assessment/intervention and escalation as needed.
C Exam trap
D Checkpoint
Question: A nurse reviews a practice question about a postpartum client who needs discharge teaching on newborn bathing, reports sadness since yesterday, and now has heavy vaginal bleeding with dizziness. Which lens should the nurse apply first to choose the most appropriate next action?
- A. Health promotion teaching - Tempting because discharge teaching is appropriate postpartum; wrong because acute hemorrhage cues outrank routine teaching.
- B. Psychosocial support - Tempting because sadness may signal mood concerns; wrong because circulation threat is more urgent than emotional screening in this moment.
- C. Physiological integrity with priority framework - Tempting because it focuses on bleeding and dizziness; right because unstable circulation must be addressed first.
- D. Management of care through delegation - Tempting because multiple needs exist; wrong because the first issue is not who to assign but what urgent condition to address.
1.1.1.4 Integrated processes and CJMM: how the exam turns content into decisions
A Explanation
The second decision conflict is whether to answer from memory alone or from a reasoning sequence. Choose the CJMM plus integrated processes. Reject answer choices that skip cue recognition, ignore analysis, or leap to intervention without matching the action to the data. The single resolving rule: the best NCLEX answer follows the most defensible sequence from cue to action to evaluation within RN scope.
WHY THIS IS TESTED: Safe practice depends on noticing what matters, deciding what it means, and acting appropriately. The exam therefore tests process, not just recall. See Fig 2.
The six CJMM steps create a clean mental algorithm: recognize cues, analyze cues, prioritize hypotheses, generate solutions, take action, evaluate outcomes. On exam day, this prevents both impulsive answering and provider-style overreach. For example, if a client has confusion, fever, and hypotension, you do not need to medically diagnose septic shock to answer safely. You must recognize concerning cues, prioritize a perfusion/infection hypothesis, initiate nursing actions per protocol, and escalate urgently.
Integrated processes tell you how nursing work appears across all domains. Communication and documentation may be tested in a respiratory question. Teaching and learning may be tested in a medication-safety question. Caring and culture may alter what response is best in a mental health or maternal-newborn item. This is why the exam feels layered: one stem can test both physiology and communication quality.
Exam takeaway: The correct option usually matches the strongest cue-to-priority-to-action sequence rather than the most impressive intervention.
flowchart LR A[Recognize cues] --> B[Analyze cues] B --> C[Prioritize hypotheses] C --> D[Generate solutions] D --> E[Take action] E --> F[Evaluate outcomes] C --> G[ABCs Stability Safety Scope] G --> E
B Worked example
A 4-year-old client in the emergency department has asthma, eczema, and a peanut allergy. After receiving a prescribed antibiotic, the child develops wheezing, lip swelling, and restlessness. The parent says, "This happened once when he had a cold," and the chart notes a low-grade fever earlier in the day. Reasoning chain: Identify task - best next nursing action. Extract key facts - wheezing, swelling, restlessness after medication. Apply rule - recognize an acute airway/allergic cue cluster. Eliminate distractors - fever and prior cold history are noise; they make infection-related reasoning tempting. Verify - the answer should prioritize airway support, urgent medication administration per orders/protocol, and escalation.
C Exam trap
D Checkpoint
Question: A client with heart failure, anxiety, and chronic back pain reports sudden chest tightness and appears pale. Which CJMM step most directly helps the nurse decide whether to treat this as anxiety or a possible perfusion problem?
- A. Recognize cues - Tempting because the nurse must notice chest tightness and pallor; incomplete because noticing alone does not compare competing explanations.
- B. Analyze cues - Tempting because it asks what the symptoms mean; right because the nurse must interpret whether the cue cluster supports perfusion concern over anxiety.
- C. Generate solutions - Tempting because the nurse wants a next action; wrong because action selection comes after interpreting the cues.
- D. Evaluate outcomes - Tempting because response monitoring matters; wrong because the nurse has not acted yet.
- The 6 CJMM steps are: recognize cues, analyze cues, prioritize hypotheses, generate solutions, take action, evaluate outcomes.
- True or False: A correct NCLEX option may be a reasonable nursing action but still be wrong because it is not the highest priority. True.
- The most common reason students miss priority items is failing to separate cue recognition from intervention selection.
1.1.1.5 RN scope inside the test plan: what the exam expects you to do versus not do
A Explanation
The third decision conflict is whether the RN should independently solve the whole medical problem or act within nursing scope and escalate appropriately. Choose RN-scope action. Reject options that require diagnosis, prescribing, or choosing a provider-only treatment plan. The single rule that resolves many questions: if an answer asks you to do something outside entry-level RN scope, it is wrong even if the medical idea sounds logical.
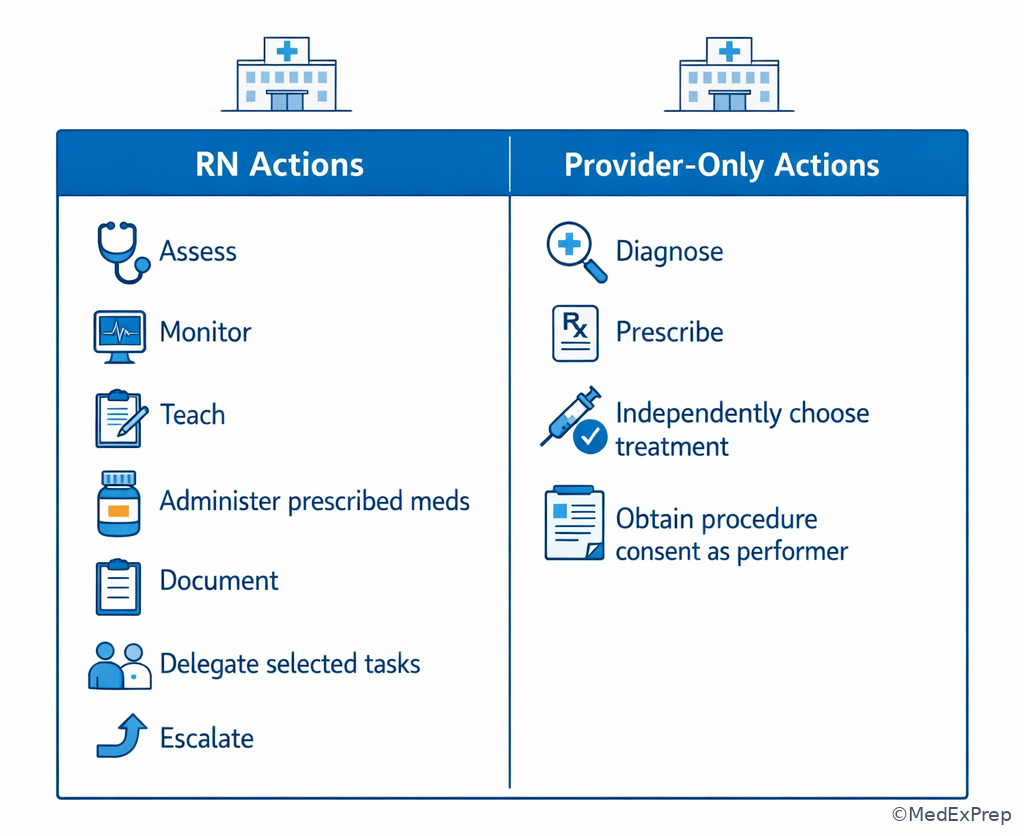
WHY THIS IS TESTED: NCLEX is a licensure exam for safe nursing practice. It must distinguish between a candidate who knows when to act and when to clarify, hold, notify, or consult. See Fig 3.
Within scope, the RN assesses, identifies cues, implements prescribed or protocol-supported interventions, monitors, teaches, documents, delegates selected tasks, and evaluates outcomes. Outside scope, the RN does not independently diagnose disease, prescribe medications, sign provider consent, or choose medical treatment plans. This distinction appears even in routine settings. A question about a medication order may really be about recognizing an unsafe order and seeking clarification, not about pharmacology facts alone.
This topic connects directly to the upcoming lesson on Entry-Level RN Scope. For now, anchor one high-yield rule: if the client is unstable, the RN keeps assessment, judgment, teaching, and evaluation. Delegation of simple tasks does not remove RN accountability.
Exam takeaway: When an option crosses into diagnosing, prescribing, or independently choosing treatment, eliminate it and choose the safest nursing action.
flowchart TD
A[Answer option] --> B{Within RN scope?}
B -->|Yes| C[Assess intervene monitor teach document delegate evaluate]
B -->|No| D[Reject option]
D --> E[Hold unsafe action if needed]
E --> F[Notify provider or consult per policy] Exam takeaway: A visual split between RN actions and provider-only actions helps eliminate scope-violating distractors quickly.
B Worked example
A 58-year-old client with COPD, hypertension, and recent pneumonia has a new provider order for a sedating medication. The client is somnolent, respirations are 10/min, oxygen saturation is 89% on prescribed oxygen, and the spouse states, "He always gets sleepy after medications." Potassium is 3.4 mEq/L. Reasoning chain: Identify task - the RN's next safe action. Extract key facts - oversedation and respiratory compromise after a new order. Apply rule - the RN should assess, hold an unsafe medication if indicated by policy/order parameters, support airway/breathing, and notify the provider. Eliminate distractors - independently changing the prescription or diagnosing respiratory failure crosses scope. Verify - the best option remains a nursing safety response plus escalation.
C Exam trap
D Checkpoint
Question: Which action most clearly falls outside entry-level RN scope on an NCLEX item?
- A. Reassessing pain 30 minutes after an IV analgesic - Tempting because follow-up is standard nursing care; wrong choice because this is within RN scope.
- B. Teaching a client how to use an incentive spirometer - Tempting because education is a nursing responsibility; wrong choice because this is within RN scope.
- C. Independently selecting an alternative antibiotic when the client reports a rash - Tempting because allergy safety matters; right because medication selection is provider authority.
- D. Holding a medication and notifying the provider about a clearly unsafe finding - Tempting because it involves medication judgment; wrong choice because recognizing unsafe administration conditions and escalating is within RN scope.
1.1.1.6 Priority language: how test-plan structure shapes what “best next action” means
A Explanation
The fourth decision conflict is between a correct nursing action and the highest-priority nursing action. Choose the option that best matches the urgency framework embedded in the test plan. Reject lower-priority but still appropriate care. The single rule: a good action loses if another option addresses airway, breathing, circulation, instability, acute change, or immediate safety risk first.
WHY THIS IS TESTED: Entry-level RNs are expected not just to know what can be done, but what must be done first. See Fig 4.
NCLEX wording often reveals the intended framework: priority, first, most appropriate next action, requires immediate follow-up, and best client to see first. These terms usually signal that multiple options are reasonable. The exam then separates candidates by whether they can rank them safely. A client who needs teaching may still wait if another client has stridor. A routine medication may be delayed if verification is needed for a possible allergy. A provider notification may be necessary, but after the RN performs a stabilizing intervention within scope if the client is actively deteriorating.
This lesson introduces the structure; the upcoming topic on Priority Frameworks will deepen the actual ranking rules. For now, know that test-plan structure and priority language work together: a question can be in any content domain and still fundamentally be a prioritization item.
Exam takeaway: When several options are correct in general, choose the one that addresses immediate instability, airway-breathing-circulation, or safety first.
flowchart TD
A[All options seem reasonable] --> B{Any ABC threat?}
B -->|Yes| C[Choose airway breathing circulation action]
B -->|No| D{Any unstable acute change?}
D -->|Yes| E[See unstable client first]
D -->|No| F{Any immediate safety risk?}
F -->|Yes| G[Remove danger / implement precautions]
F -->|No| H[Then teach, comfort, or routine tasks] B Worked example
An RN on a postpartum unit receives four updates: a client requesting breastfeeding teaching, a client with anxiety about newborn bathing, a client with a saturated perineal pad and lightheadedness, and a client asking for PRN ibuprofen for cramping. The hemorrhage client also has a history of iron-deficiency anemia and reports mild nausea after lunch. Reasoning chain: Identify task - best client to address first. Extract key facts - heavy bleeding and lightheadedness indicate possible instability. Apply rule - circulation threat outranks teaching, reassurance, and routine analgesia. Eliminate distractors - the breastfeeding client and anxious parent still need care, but later. Verify - the best answer addresses hemorrhage first and triggers immediate assessment/intervention.
C Exam trap
D Checkpoint
Question: Which statement best explains why many NCLEX priority questions feel difficult?
- A. They usually require memorizing rare diseases - Tempting because unfamiliar conditions increase stress; wrong because the main challenge is often ranking safe nursing actions.
- B. They often contain several actions that are all appropriate at different times - Tempting because this matches real exam experience; right because priority wording forces you to choose the best action now.
- C. They depend mostly on calculating medication doses - Tempting because math can be stressful; wrong because many difficult items contain no calculations.
- D. They are designed around provider treatment plans - Tempting because medical knowledge appears in stems; wrong because the NCLEX targets nursing judgment within RN scope.
- If a stem says first or priority, ask which option addresses ABCs, instability, or safety.
- True or False: An option can be correct nursing care and still be the wrong NCLEX answer. True.
- Name 3 common urgency signals: airway/breathing problem, hemodynamic instability, immediate safety threat.
1.1.1.7 Building a study plan from the test plan without using false precision
A Explanation
The final decision conflict is whether to study by chasing guessed percentages or by building balanced coverage around official structure and recurring themes. Choose balanced, blueprint-informed study. Reject false precision such as invented chapter weights or overcommitting to favorite systems while neglecting safety, delegation, and communication. The single rule: when official weighting is broad or unspecified, prepare across all major domains and use repeated NCLEX themes to guide review density.
WHY THIS IS TESTED: Candidates often fail not because they know too little medicine, but because they underprepare in high-frequency nursing judgment areas like delegation, infection prevention, medication safety, and early recognition of deterioration. See Fig 5.
A strong study plan uses the test plan as an organizer, then layers recurring nursing themes onto it: respiratory compromise, hemodynamic instability, sepsis/infection risk, medication adverse effects, electrolyte/lab abnormalities, falls/aspiration/pressure injury prevention, therapeutic communication, and delegation boundaries. This approach mirrors how the NCLEX blends content. You may get a pediatric stem that is really about respiratory priority, or a community-health item that is really about teaching and safety.
Do not mistake broad coverage for equal importance in every week of studying. Instead, use retrieval cycles: review the framework, practice scenario questions, identify error patterns, and revisit weak domains. Follow agency policy and state nurse practice rules when local processes vary.
Exam takeaway: Organize study by domains, recurring nursing themes, and error patterns rather than by random disease lists.
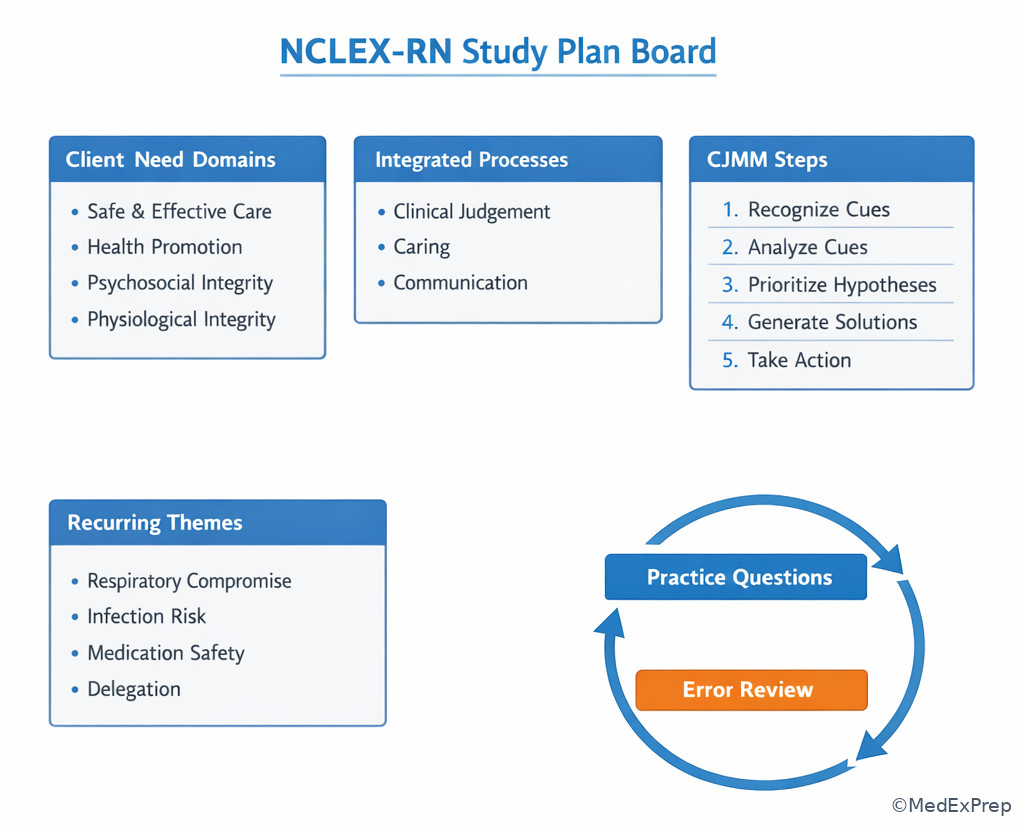
Exam takeaway: Mixed practice better reflects the exam because client need, process, and priority often overlap in one stem.
B Worked example
A student scores well on endocrine and cardiac content quizzes but misses multiple NCLEX-style items on falls, isolation, prioritization, and delegation. The student decides to spend the next week reviewing only arrhythmias because that feels more medical. Reasoning chain: Identify task - choose the best study adjustment. Extract key facts - misses cluster in nursing judgment domains, not disease facts. Apply rule - blueprint-informed study corrects the tested weakness. Eliminate distractors - more disease detail may feel productive but does not target the actual pattern. Verify - the safer plan is mixed practice plus focused review of priority, scope, safety, and communication frameworks.
C Exam trap
D Checkpoint
Question: Which study strategy best matches the NCLEX test plan structure?
- A. Study only adult medical-surgical diseases because most questions are clinical - Tempting because many stems involve illness; wrong because the exam also heavily tests safety, delegation, communication, and teaching across settings.
- B. Use official broad domains, integrated processes, and recurring nursing themes to organize mixed practice - Tempting because it is systematic; right because it matches how the exam integrates content and judgment.
- C. Memorize unofficial percentages from social media and ignore weak areas with lower rumored frequency - Tempting because it promises efficiency; wrong because unsupported weighting creates dangerous blind spots.
- D. Review only content from the most recent clinical rotation - Tempting because it feels current; wrong because the NCLEX is broad across populations and settings.
Exam Traps & Differentiators
- Most common wrong answer and why: choosing a medically impressive action that crosses RN scope. It is tempting because it sounds decisive. Eliminate it when the action requires diagnosing, prescribing, or independently choosing treatment.
- Looks similar but isn't: assessment versus delay. "Assess first" is correct only when there is not already enough data to identify an immediate threat requiring urgent action within protocol.
- Right action, wrong priority: teaching, comfort, documentation, or notification may all be appropriate, but not before airway, bleeding, or acute neurological change.
- Client-centered wording trap: responding to the client's stated preference first feels therapeutic, but objective instability outranks conversational concerns.
- Delegation trap: assigning a task that requires nursing judgment to UAP or LPN/LVN. The option looks efficient but fails the scope/accountability test.
| Stem says... | Think... | Reject... |
|---|---|---|
| Priority / first / immediate follow-up | ABCs, instability, actual harm | Routine teaching or comfort first |
| Best next nursing action | RN-scope intervention | Provider-only decision |
| Which task to delegate | Stable, predictable, no judgment | Initial assessment, unstable client, teaching evaluation |
| Requires clarification | Unsafe order, mismatch with client condition | Blind compliance with the order |
| Most important to monitor | Outcome tied to biggest risk | Less urgent but familiar data point |
| Confusable pair | Why it feels similar | Discriminator |
|---|---|---|
| Assess first vs act first | Both are nursing-process valid | Act first when clear immediate threat is already evident |
| Notify provider vs intervene first | Both may be needed | Use immediate RN stabilization within scope before calling when client is actively compromised |
| Teach vs prioritize | Teaching is always important | Teaching waits when airway, perfusion, or safety is unstable |
| Delegate vs do yourself | Efficiency matters in practice | RN keeps judgment, unstable assessment, and evaluation |
| Medical knowledge vs nursing action | Disease terms dominate stems | Question asks what the RN should assess, do, teach, or report |
If the stem says "new shortness of breath," think physiological priority before teaching.
If the stem says "which action requires clarification," think scope, safety, and mismatch with client status.
If the stem says "best client to see first," think unstable before stable.
If the stem says "which task is appropriate to delegate," think predictable task without nursing judgment.
If the stem says "most likely needs immediate follow-up," think objective deterioration over subjective but noncritical concerns.
Tables
| Reference summary | High-yield use on questions |
|---|---|
| Client needs | Tell you the broad content area being tested |
| Integrated processes | Explain why communication, teaching, and nursing process appear in every domain |
| CJMM steps | Provide a repeatable reasoning sequence from cue to action |
| RN scope | Eliminates provider-only distractors |
| Priority frameworks | Separate a reasonable action from the best action now |
| Recurring NCLEX themes | Guide study toward frequently tested safety patterns |
| Framework | Question it answers | Example use |
|---|---|---|
| Client need domain | What broad area is this? | Safety vs physiology vs psychosocial |
| Integrated process | What nursing function is embedded? | Teaching, documentation, communication |
| CJMM | What step am I in? | Recognize cues before generating solutions |
| RN scope | Can the nurse do this independently? | Teach spirometer use: yes; choose antibiotic: no |
| Priority rule | Which option comes first? | Dyspnea before discharge teaching |
| Differential classification | What it looks like | What it is really testing |
|---|---|---|
| Medication question | Drug name and order details | Safety check, monitoring, or clarification |
| Postpartum question | Teaching, bonding, bleeding | Priority and maternal safety |
| Pediatric respiratory question | Parent report plus symptoms | Cue recognition and airway priority |
| Mental health question | Therapeutic response options | Communication process and safety |
| Delegation question | Several realistic unit tasks | Scope, stability, and accountability |
| Community question | Home teaching and resources | Health promotion plus safety and follow-up |
Exam takeaway: A visual cue board reinforces that many items are solved by sorting findings into urgency categories.
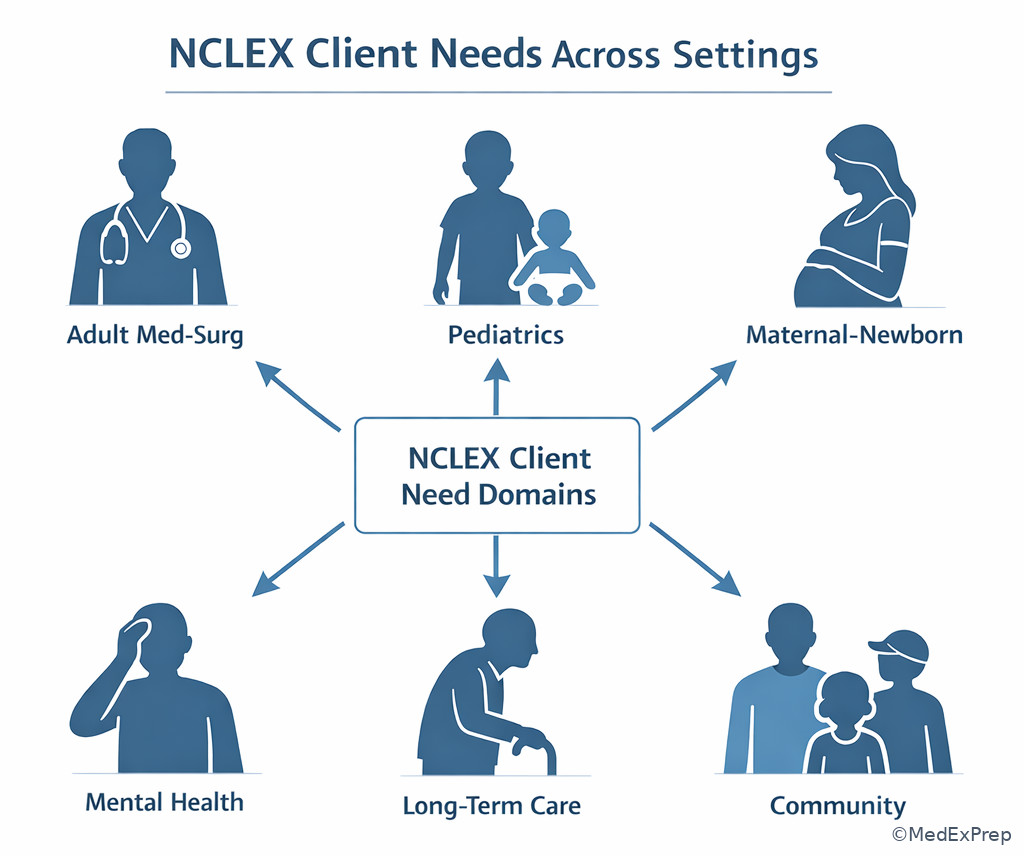
Exam takeaway: The same test-plan structure applies in adult, pediatric, maternal-newborn, mental health, and community questions.
Algorithm / Approach
Use this mini decision framework on every new question. It is especially useful early in the course while you are still learning how the exam is built. See Fig 1, Fig 3, and Fig 4.
Exam takeaway: A repeatable stem-to-answer algorithm reduces errors caused by scope confusion, weak prioritization, and distractor attraction.
Rapid Review
- Test plan -> organizes nursing decisions, not just diseases.
- Client need domain -> tells you the broad care problem category.
- Integrated process -> explains why teaching and documentation appear everywhere.
- CJMM -> converts cues into a defensible action sequence.
- Recognize cues -> isolate the abnormal finding that changes priority.
- Analyze cues -> compare what the findings mean before acting.
- Prioritize hypotheses -> rank airway, perfusion, and safety threats first.
- RN scope -> assess, intervene, monitor, teach, document, delegate selected tasks, escalate.
- Provider-only action -> diagnose, prescribe, or independently choose treatment.
- Priority item -> several options may be true, but only one is safest now.
- Delegation item -> stability and predictability decide what leaves the RN.
- Communication item -> still may be a safety or priority question underneath.
- Study plan -> organize by domains plus recurring nursing themes, not social-media percentages.
- Noise in stems -> chronic conditions and mild labs often distract from the acute cue.
Self-check quiz
1. A nursing student reviews a practice item about a client with new wheezing after a medication, chronic eczema, and parental concern about school attendance tomorrow. Which action best matches NCLEX test-plan thinking?
- A. Address the school concern first because it is the client's stated priority
- B. Focus on the new wheezing and choose the safest immediate nursing action
- C. Select the option that names the most likely medical diagnosis
- D. Choose the answer with the most complex medication change
2. A client with chronic heart failure, anxiety, and insomnia reports sudden shortness of breath while asking for sleep-hygiene teaching. Which option is most appropriate for the RN to eliminate first as outside scope?
- A. Reassess lung sounds and oxygen saturation
- B. Teach slow pursed-lip breathing while further assessing
- C. Independently prescribe a higher diuretic dose for the evening
- D. Notify the provider after obtaining focused assessment findings
3. A 68-year-old client in long-term care has dementia, diabetes, and chronic constipation. The UAP reports the client is more sleepy than usual. Vital signs are temperature 38.4°C, heart rate 112/min, blood pressure 92/58 mm Hg, respiratory rate 24/min. The client also has dry skin and had a poor appetite at breakfast. Which is the most appropriate next nursing action?
- A. Ask the UAP to repeat the vital signs in 30 minutes
- B. Perform immediate focused assessment and escalate concern for possible deterioration
- C. Document decreased appetite and continue routine rounds
- D. Provide constipation teaching after administering scheduled stool softener
4. A postpartum client, 6 hours after delivery, has mild perineal discomfort, asks about newborn bathing, and suddenly reports dizziness. The pad is saturated in 20 minutes. The client has asthma and seasonal allergies, and a hemoglobin from yesterday is mildly low. Which framework should guide the RN's answer selection first?
- A. Health promotion and teaching
- B. Psychosocial support
- C. Circulation priority within physiological integrity
- D. Delegation efficiency
5. A school-age child with asthma, ADHD, and a recent ear infection receives a prescribed medication and then develops lip swelling and inspiratory wheeze. The parent says the child "gets dramatic when scared," and the chart notes a slightly elevated temperature earlier. Which CJMM step most directly separates the correct answer from distractors?
- A. Analyze cues
- B. Evaluate outcomes
- C. Document teaching
- D. Delegate routine care
6. An RN receives four possible actions for a client with new confusion after opioid administration: decrease the opioid dose independently, hold the medication and assess respirations, ask the UAP to determine sedation level, or tell the family the confusion is expected. The client also has COPD and sleep apnea. Which is the most appropriate next action?
- A. Decrease the opioid dose independently
- B. Hold the medication and assess respirations
- C. Ask the UAP to determine sedation level
- D. Reassure the family and continue monitoring only
7. An RN candidate reviews scores and sees strong performance in endocrine and cardiac content but repeated misses in delegation, order clarification, fall precautions, and infection isolation. The candidate plans the next study block. Which approach is most appropriate?
- A. Spend all study time on endocrine content because it feels highest yield
- B. Use a blueprint-based mixed review focused on weak nursing judgment domains
- C. Ignore low-scoring areas until memorization of diseases is complete
- D. Use unofficial online percentages to skip topics that seem less common
8. During a simulated NCLEX item review, a client with pneumonia, chronic kidney disease, and anxiety has oxygen saturation 86% on room air, asks when discharge papers will be ready, and has a potassium level of 3.3 mEq/L from yesterday. Four answer choices are offered: start discharge teaching, apply oxygen per protocol and assess, independently order a chest x-ray, or delegate the initial respiratory assessment to the UAP. Which choice best fits the NCLEX test-plan structure?
- A. Start discharge teaching
- B. Apply oxygen per protocol and assess
- C. Independently order a chest x-ray
- D. Delegate the initial respiratory assessment to the UAP
Answer key
1. Correct answer: B. Focus on the new wheezing and choose the safest immediate nursing action.
- A: Tempting because client concerns matter and NCLEX values client-centered care. Incorrect because ABCs outrank next-day planning; the single stem clue is new wheezing after a medication. Priority-rationale: address breathing first. Source: NCSBN Clinical Judgment framework; Lewis.
- B: Tempting because it centers the acute cue, and correct because it matches test-plan thinking: physiological integrity plus CJMM plus RN-safe priority action. The discriminating clue is wheezing. Source: NCSBN; Saunders.
- C: Tempting because identifying the underlying problem feels intellectually satisfying. Incorrect because NCLEX asks for the RN's action, not independent medical diagnosis. The clue is what should the RN do. Source: ANA Standards; NCSBN.
- D: Tempting because high-intensity treatment sounds urgent. Incorrect because complexity does not beat scope and priority; the RN does not choose medication changes independently. The clue is nursing action, not treatment selection. Source: ANA Standards; Saunders.
2. Correct answer: C. Independently prescribe a higher diuretic dose for the evening.
- A: Tempting because assessment often comes first. Incorrect as the answer to this question because reassessing oxygenation is within RN scope, so it should not be eliminated. The clue is outside scope. Source: ANA Standards; Lewis.
- B: Tempting because teaching and breathing support are common nursing measures. Incorrect as the answer because this remains within RN scope. The clue is pursed-lip breathing, a nursing intervention. Source: Saunders.
- C: Tempting because the client has heart failure and worsening symptoms. Correct because independently prescribing or adjusting a diuretic dose is provider authority. The single discriminating clue is prescribe. Source: ANA Standards of Practice; NCSBN scope guardrails.
- D: Tempting because provider notification is often needed. Incorrect as the answer because notifying after focused assessment findings is appropriate RN action. The clue is after obtaining assessment findings. Source: NCSBN; Lewis.
3. Correct answer: B. Perform immediate focused assessment and escalate concern for possible deterioration.
- A: Tempting because repeating data can confirm an abnormal finding. Incorrect because the client already shows a concerning cue cluster: fever, tachycardia, hypotension, and tachypnea. The discriminating clue is BP 92/58 mm Hg with fever and tachycardia. Priority-rationale: unstable before routine recheck. Source: Lewis; NCSBN.
- B: Tempting because it addresses instability directly, and correct because the RN must assess deterioration and escalate promptly. The clue is the multi-system abnormal vital-sign pattern. Priority-rationale: ABCs/circulation and safety. Source: Lewis; Saunders.
- C: Tempting because documentation matters and poor appetite may be relevant. Incorrect because documentation does not come before assessment of possible sepsis or hypoperfusion. The clue is acute change in level of alertness. Source: NCSBN; ANA.
- D: Tempting because constipation care is valid in long-term care. Incorrect because chronic bowel management is lower priority than acute instability. The clue is more sleepy than usual plus abnormal vitals. Source: Saunders.
4. Correct answer: C. Circulation priority within physiological integrity.
- A: Tempting because postpartum teaching is expected before discharge. Incorrect because heavy bleeding with dizziness indicates an acute circulation problem. The clue is saturated pad in 20 minutes. Source: Lewis obstetric nursing principles; Saunders.
- B: Tempting because postpartum emotion and support are important. Incorrect because psychosocial care does not outrank hemorrhage cues. The clue is dizziness plus rapid pad saturation. Source: NCSBN; Saunders.
- C: Tempting because it directs attention to the urgent physiologic issue, and correct because circulation threat determines the best next action. The discriminating clue is acute excessive bleeding. Source: Lewis; NCSBN.
- D: Tempting because several needs exist and delegation may seem efficient. Incorrect because deciding who should help is not the first question when the client may be unstable. The clue is possible hemorrhage. Source: ANA; NCSBN.
5. Correct answer: A. Analyze cues.
- A: Tempting because it asks what the findings mean, and correct because the nurse must interpret lip swelling plus inspiratory wheeze after medication as an acute allergic/airway problem rather than anxiety or fever. The clue is symptoms immediately after medication. Source: NCSBN CJMM; Saunders.
- B: Tempting because outcome evaluation is always part of care. Incorrect because the nurse has not yet chosen the action; interpretation comes first. The clue is decision still pending. Source: NCSBN.
- C: Tempting because documentation is expected. Incorrect because it is not the CJMM step that separates the right answer in an acute event. The clue is airway cues. Source: ANA; Lewis.
- D: Tempting because routine tasks may be delegated. Incorrect because delegation is irrelevant until the nurse identifies the acute problem and acts. The clue is active respiratory compromise. Source: NCSBN; ANA.
6. Correct answer: B. Hold the medication and assess respirations.
- A: Tempting because reducing the opioid seems to address the cause. Incorrect because dose adjustment is prescribing. The discriminating clue is independently. Priority-rationale: scope violation. Source: ANA Standards; NCSBN.
- B: Tempting because it is immediate and within scope, and correct because the RN should stop the unsafe administration, assess airway/breathing, and then escalate. The clue is new confusion after opioid administration in COPD and sleep apnea. Priority-rationale: breathing first. Source: Lewis; Saunders.
- C: Tempting because UAP assistance may save time. Incorrect because sedation level in a newly unstable client requires RN assessment and judgment. The clue is new confusion with respiratory risk factors. Source: ANA delegation principles; NCSBN.
- D: Tempting because mild confusion can occur with opioids. Incorrect because reassurance alone ignores a potential respiratory-depression event. The clue is COPD and sleep apnea. Source: Lewis; Saunders.
7. Correct answer: B. Use a blueprint-based mixed review focused on weak nursing judgment domains.
- A: Tempting because familiar content boosts confidence. Incorrect because it does not target the actual error pattern. The clue is repeated misses in delegation, clarification, precautions, isolation. Source: Saunders; NCSBN.
- B: Tempting because it is systematic, and correct because the NCLEX tests integrated nursing judgment across domains, not just disease recall. The discriminating clue is weakness in nursing judgment areas. Source: NCSBN test plan principles; Saunders.
- C: Tempting because some students believe diseases must be mastered first. Incorrect because deferring major decision-framework weaknesses prolongs the real problem. The clue is high content performance already exists. Source: HESI review principles; NCSBN.
- D: Tempting because percentages promise efficiency. Incorrect because unofficial weighting can create blind spots and is not authoritative. The clue is unofficial online percentages. Source: NCSBN guidance; Saunders.
8. Correct answer: B. Apply oxygen per protocol and assess.
- A: Tempting because discharge readiness matters and the client is asking about it. Incorrect because oxygen saturation of 86% indicates an immediate breathing priority. The clue is 86% on room air. Priority-rationale: breathing before teaching. Source: Lewis; NCSBN.
- B: Tempting because it addresses the acute cue directly, and correct because it is a within-scope nursing action that matches the test plan's focus on safe, immediate care and cue response. The discriminating clue is hypoxemia. Source: Lewis; Saunders.
- C: Tempting because imaging might help explain pneumonia status. Incorrect because ordering diagnostics independently is outside RN scope. The clue is independently order. Source: ANA Standards; NCSBN.
- D: Tempting because delegation can improve workflow. Incorrect because the initial respiratory assessment of an unstable client must remain with the RN. The clue is initial assessment plus low oxygen saturation. Source: ANA delegation principles; NCSBN.