Why it matters
- The NCLEX-PN does not reward memorizing random facts; it rewards recognizing what kind of client need the stem is testing and choosing the safest action within PN/LVN scope.
- Many wrong answers are tempting because they are reasonable nursing actions, but they belong to the wrong category or wrong priority level.
- Knowing the framework helps you sort questions faster: urgent physiologic instability, infection risk, communication, teaching reinforcement, delegation, and documentation each have different best-next-step rules.
- This framework becomes the base for the next topics on clinical judgment steps and priority frameworks, so early mastery reduces errors across the entire course.
Key Terms & Must-Know Facts
1.1.1.1 Key terms
- Client needs framework: the NCLEX-PN content map used to organize safe nursing care decisions.
- Management of Care: coordination, reporting, assignment, advocacy, and safe participation in care systems.
- Safety and Infection Control: prevention of injury, errors, and transmission of infection.
- Health Promotion and Maintenance: growth, development, prevention, screening, and teaching reinforcement.
- Psychosocial Integrity: emotional support, coping, therapeutic communication, and behavioral safety.
- Basic Care and Comfort: mobility, hygiene, elimination, nutrition, and comfort measures.
- Pharmacological and Parenteral Therapies: medication administration, monitoring, and IV-related safety within scope.
- Reduction of Risk Potential: monitoring for complications, trends, labs, and early warning signs.
- Physiological Adaptation: response to acute physiologic change or instability.
- Cue recognition: noticing relevant assessment data.
- Prioritization: choosing which need is most urgent.
- Action selection: taking the safest in-scope step.
- Evaluation: checking response after action.
- Scope of practice: what a PN/LVN can perform under law, policy, and supervision requirements.
1.1.1.2 Must-know facts
- One NCLEX question can touch more than one category, but one category usually best explains the safest answer.
- ABCs and acute instability usually outrank teaching, comfort, and routine documentation.
- For PN/LVN exam items, unsafe escalation delays are common distractors.
- Psychosocial questions still use safety-first reasoning.
- Medication questions test administration safety, monitoring, side effects, and reporting more often than drug memorization alone.
- Reduction of Risk Potential often appears as trend recognition rather than crisis treatment.
- Health Promotion and Maintenance focuses on expected teaching and prevention, not unstable client rescue.
- Management of Care for PN/LVN questions emphasizes assignment, reporting, confidentiality, and chain of command within scope.
Exam takeaway: Sort the stem into a client-needs bucket before choosing the safest action.
flowchart TD
A[Read the stem] --> B{What is the main task?}
B --> C[Safe care system issue
Management of Care]
B --> D[Injury or infection prevention
Safety and Infection Control]
B --> E[Prevention or teaching reinforcement
Health Promotion and Maintenance]
B --> F[Emotional coping or communication
Psychosocial Integrity]
B --> G[Physical care need
Physiological Integrity]
G --> G1[Basic Care and Comfort]
G --> G2[Pharmacological and Parenteral Therapies]
G --> G3[Reduction of Risk Potential]
G --> G4[Physiological Adaptation] Exam takeaway: Use ABCs and instability to decide which category wins when a stem fits more than one.
flowchart LR
A[Multiple possible categories] --> B{Any airway, breathing, circulation, acute neuro, severe bleeding, or sepsis cue?}
B -->|Yes| C[Physiological Adaptation / urgent escalation]
B -->|No| D{Immediate safety or infection threat?}
D -->|Yes| E[Safety and Infection Control]
D -->|No| F{Routine teaching, support, comfort, or monitoring?}
F --> G[Use the best matching lower-acuity category] Exam takeaway: Visual grouping helps you quickly recognize whether a question is about safety systems, psychosocial care, prevention, or physiologic problems.

Exam takeaway: Many exam stems ask for the safest in-scope bedside action before higher-level decisions by the RN or provider.
Core content
1.1.1.3 Foundational map: what the client-needs framework is really asking
A Explanation
The first decision conflict is simple but high yield: Is this question mainly asking what kind of need the client has, or is it tempting you to jump straight to an intervention? On exam day, students often misfire because they see a familiar action and choose it before classifying the problem. The rule that resolves this: name the main need before naming the action. If the stem is about safe systems, assignment, confidentiality, or reporting, think Management of Care. If the stem is about injury prevention or precautions, think Safety and Infection Control. If it is about prevention, developmental expectations, or reinforcing routine teaching, think Health Promotion and Maintenance. If emotions, coping, crisis communication, or behavior dominate, think Psychosocial Integrity. If the body system problem is central, think Physiological Integrity and then decide which physiologic subcategory fits best.
WHY THIS IS TESTED: The NCLEX-PN commonly gives an answer that is not unsafe, but belongs to the wrong problem category and therefore is not the best answer.
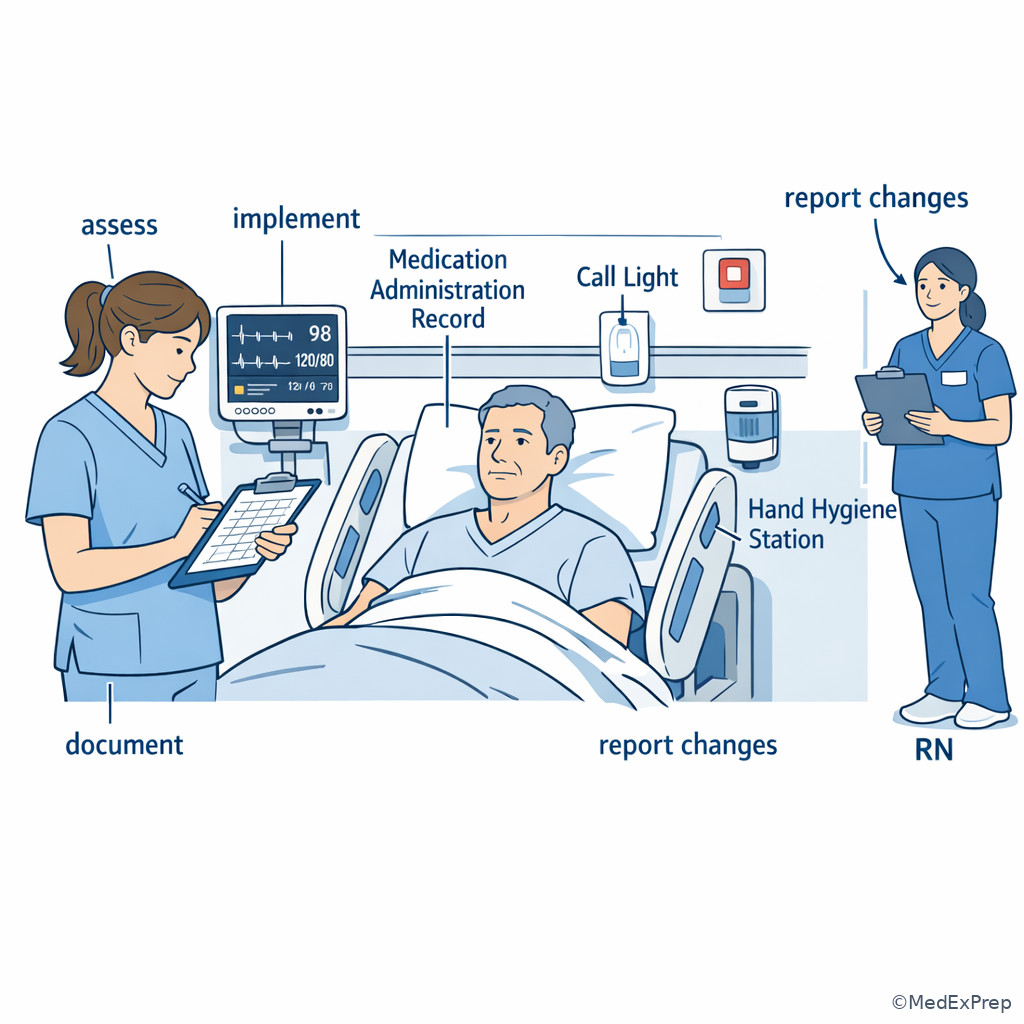
Use See Fig 1 when you feel two answers both sound reasonable. The figure compresses the exam logic: sort the task first, then decide priority. This matters for PN/LVN scope because your safest action is often to assess a focused cue, implement an established intervention, document accurately, and report unexpected findings—not to independently redesign the plan of care.
B Worked example
A 72-year-old client in a rehabilitation unit has hypertension, osteoarthritis, and mild hearing loss. The client says, “I’m worried I’ll fall when I get up tonight.” The chart also notes a family question about low-sodium diet teaching, and the latest potassium is 3.4 mEq/L. Which issue best frames the nurse’s immediate task? Identify task: the question asks what kind of need is primary. Extract key facts: fear of falling, nighttime mobility risk, rehab setting, mild lab abnormality that is not the main threat, and diet teaching as a secondary issue. Apply rule: immediate fall prevention belongs to Safety and Infection Control, not Health Promotion and Maintenance and not Reduction of Risk Potential. Eliminate distractors: the low potassium is mildly abnormal but not the reason for the stem; diet teaching matters but is not the current priority. Verify: the best framework label is safety risk prevention.
C Exam trap
D Checkpoint
Question: A practical nurse reviews four chart notes. Which note is best categorized under Management of Care rather than another client-needs area?
- Reinforcing home foot-care teaching to a client with diabetes before discharge
- Reporting a change in urine output and edema to the RN for a client with heart failure
- Applying seizure precautions for a client admitted after a syncopal episode
- Using open-ended statements with a grieving spouse in hospice
Answer: B
- A: Tempting because discharge tasks involve coordination, but the core purpose is preventive teaching reinforcement, so this fits Health Promotion and Maintenance.
- B: Tempting because edema is physiologic, but the action tested is recognizing change and reporting through the care system, which fits Management of Care.
- C: Tempting because precautions feel like “management,” but seizure precautions are a safety intervention, so Safety and Infection Control is the better match.
- D: Tempting because hospice care involves many team issues, but the action is therapeutic communication, so it fits Psychosocial Integrity.
1.1.1.4 The major categories and their high-yield boundaries
A Explanation
The next decision conflict is boundary confusion: Which category looks similar but is not the best fit? This is where most framework questions become testable. Health Promotion and Maintenance can look like Basic Care and Comfort because both involve routine care, but prevention and teaching reinforcement belong to health promotion, while feeding assistance, hygiene, positioning, and elimination support belong to basic care. Reduction of Risk Potential can look like Physiological Adaptation because both involve body problems, but risk reduction usually means monitoring for complications or trend recognition before crisis develops; physiologic adaptation usually means the client is already unstable or acutely worsening. Management of Care can overlap with Safety and Infection Control, but if the answer centers on assignment, chain of command, consent/confidentiality, or reporting, it belongs to management; if it centers on preventing falls, sharps injury, or infection spread, it belongs to safety.
WHY THIS IS TESTED: the exam wants to know whether you can distinguish routine support, monitoring, urgent rescue, and system-level nursing actions without mixing them up.
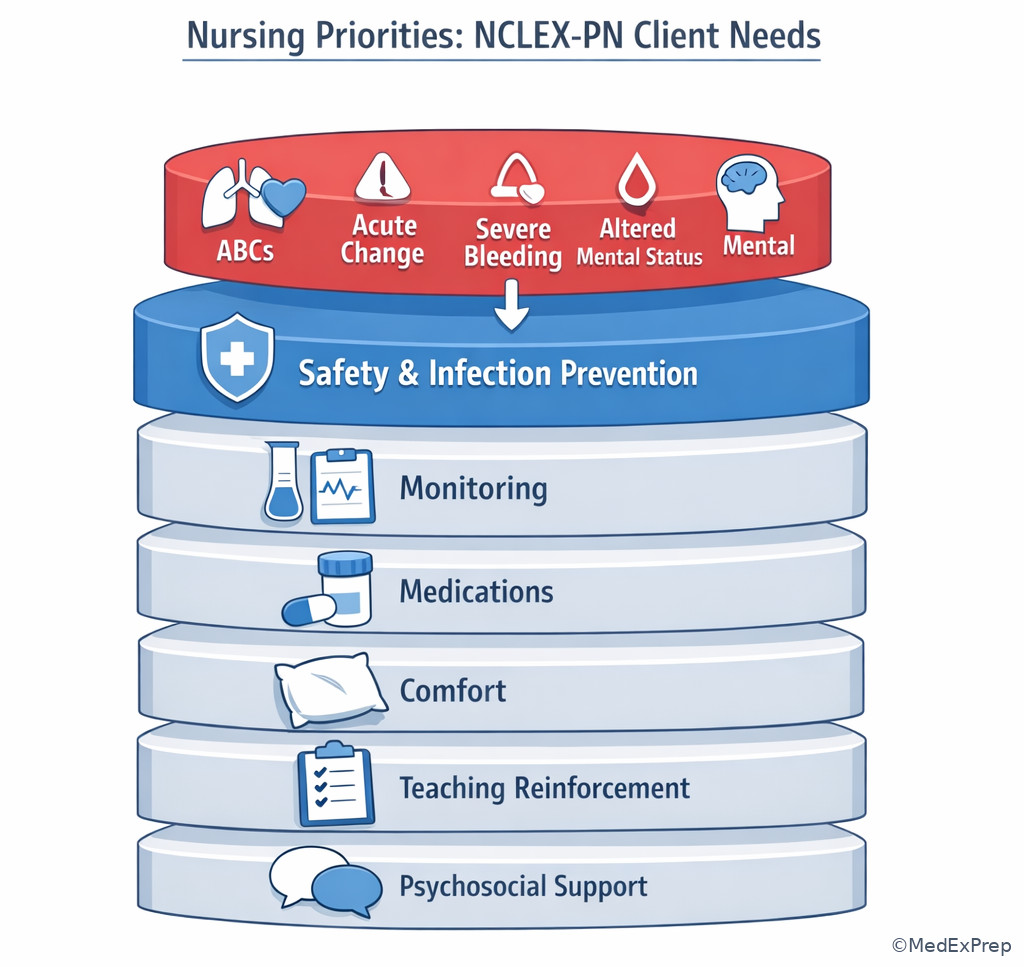
See Fig 2 for the priority overlay that breaks ties. When two categories fit, the more urgent ABC/safety issue usually wins. This becomes especially important in mixed stems containing both psychosocial distress and physiologic cues. Anxiety matters, but severe dyspnea still comes first.
B Worked example
A 19-year-old postpartum client with iron-deficiency anemia and generalized anxiety says she feels “overwhelmed” about newborn care. She is also saturating one peri-pad every 15 minutes and has a pulse of 122/min. A family member asks for breastfeeding teaching handouts. Identify task: choose the dominant category. Extract key facts: postpartum setting, emotional distress, educational need, and a major bleeding cue with tachycardia. Apply rule: acute heavy bleeding with tachycardia is Physiological Adaptation, not Psychosocial Integrity and not Health Promotion and Maintenance. Eliminate distractors: anxiety is real but not the highest priority; teaching is lower priority; anemia history is noise because the current bleed is the urgent cue. Verify: address acute physiologic instability and notify the RN/provider per policy while taking immediate safety actions.
C Exam trap
D Checkpoint
Question: Which action is best grouped under Reduction of Risk Potential?
- Checking a postoperative client’s urine output trend and reporting a decline over 4 hours
- Raising side rails and keeping the bed low for a client receiving opioids
- Assisting with oral care and repositioning a client on bed rest
- Reinforcing vaccine schedule teaching with a parent at a clinic visit
Answer: A
- A: Tempting because it may later become physiologic instability, but the tested action is monitoring trends and reporting risk before crisis, which is Reduction of Risk Potential.
- B: Tempting because opioids involve medications, but the action itself is preventing injury, so it fits Safety and Infection Control.
- C: Tempting because immobility can cause complications, but the direct task is comfort and routine physical care, so this is Basic Care and Comfort.
- D: Tempting because vaccines are medical, but the focus is prevention and teaching reinforcement, so this fits Health Promotion and Maintenance.
- The category most tied to confidentiality, chain of command, and reporting is Management of Care.
- True or False: A question about trend monitoring before a crisis usually fits Physiological Adaptation. False.
- Name the 3 commonly confused pairs: Health Promotion vs Basic Care, Reduction of Risk vs Physiological Adaptation, Management vs Safety.
1.1.1.5 Physiological Integrity: breaking the largest category into testable pieces
A Explanation
Physiological Integrity is the largest source of confusion because it contains four different kinds of exam tasks. The decision conflict is: What type of body-care question is this actually testing? If the answer is feeding, hygiene, mobility, skin care, sleep, elimination support, or nonpharmacologic comfort, choose Basic Care and Comfort. If the answer is medication administration, IV monitoring, adverse effects, dosage safety, or route-specific concerns, choose Pharmacological and Parenteral Therapies. If the answer is watching for complications, interpreting labs or trends, or recognizing early warning signs, choose Reduction of Risk Potential. If the answer is responding to acute physiologic deterioration such as respiratory distress, shock, severe bleeding, or sudden neurologic decline, choose Physiological Adaptation.
WHY THIS IS TESTED: NCLEX-PN stems often give the same client condition but ask four different questions, each belonging to a different physiologic subcategory.
See Fig 1 again for the sub-branches under Physiological Integrity. This is not trivia; it changes the best answer. For a client with COPD, assisting with meals is Basic Care and Comfort, checking oxygen tubing safety may be Safety and Infection Control, monitoring pulse oximetry trend is Reduction of Risk Potential, and responding to sudden severe dyspnea is Physiological Adaptation.
B Worked example
A 67-year-old client with type 2 diabetes, chronic kidney disease, and peripheral neuropathy is admitted with pneumonia. During the shift, the client needs assistance to the toilet, receives an IV antibiotic, has a rising creatinine level, and later becomes suddenly confused with oxygen saturation 84% on room air. Identify task: decide which physiologic subcategory fits each cue. Extract key facts: toileting help, IV medication, worsening lab trend, then acute hypoxemia/confusion. Apply rule: toileting assistance = Basic Care and Comfort; IV antibiotic \(administration/monitoring = Pharmacological and Parenteral Therapies\); rising creatinine = Reduction of Risk Potential; sudden confusion with low oxygen saturation = Physiological Adaptation. Eliminate distractors: do not label everything “physiologic adaptation” just because the client is sick. Verify: the category depends on the task asked in the stem, not only the diagnosis.
C Exam trap
D Checkpoint
Question: A client receiving furosemide reports dizziness on standing. Which question most clearly belongs to Pharmacological and Parenteral Therapies?
- What intervention best reduces fall risk during ambulation?
- Which finding should be reported as a potential adverse medication effect?
- Which meal choice best supports sodium restriction teaching?
- Which trend suggests worsening fluid overload over 24 hours?
Answer: B
- A: Tempting because dizziness occurs after a drug, but the question asks about injury prevention, so Safety and Infection Control is the better fit.
- B: Tempting because it may also require reporting, but the tested focus is adverse-effect recognition from a medication, which belongs to Pharmacological and Parenteral Therapies.
- C: Tempting because the medication is diuretic-related, but the core task is dietary teaching reinforcement, so Health Promotion and Maintenance fits better.
- D: Tempting because diuretics change fluid status, but trend monitoring over time is Reduction of Risk Potential.
1.1.1.6 Management, safety, and psychosocial integrity in PN/LVN scope
A Explanation
This section tests a different conflict: When does the safest answer involve communication, reporting, or system behavior instead of hands-on care? For PN/LVN questions, this is especially high yield because scope matters. Management of Care includes participation in assignment processes, following the chain of command, protecting confidentiality, obtaining and documenting accurate data, and reporting changes. Safety and Infection Control includes standard and transmission-based precautions, fall prevention, medication error prevention, and environmental safety. Psychosocial Integrity includes therapeutic communication, support for coping, nonjudgmental responses, behavioral de-escalation, and maintaining emotional safety. The resolving rule: choose the answer that matches both the client need and the PN/LVN role. If the stem drifts into independent diagnosis, care-plan design, or unsupervised triage, reject it.
WHY THIS IS TESTED: NCLEX-PN often offers one answer that sounds clinically smart but exceeds PN/LVN authority, and another that is safer, more conservative, and therefore correct.
See Fig 2 for tie-breaking with priority. For example, a client expressing hopelessness belongs to Psychosocial Integrity, but if the same client also has access to a sharp object and escalating agitation, safety becomes immediate. Likewise, documenting an abnormal finding is correct but not sufficient if the finding also requires prompt reporting.
B Worked example
A 54-year-old client with alcohol use disorder, cirrhosis, and depression is hospitalized for GI bleeding now stabilized. During the evening shift, the client says, “I don’t want to wake up tomorrow,” while pulling at the IV dressing. The spouse asks whether the client’s lab results can be discussed in the hallway. Identify task: choose the primary safe response category. Extract key facts: self-harm statement, behavioral agitation, confidentiality request in a public area, and a distracting stable past bleed. Apply rule: immediate safety and psychosocial response are central; maintain a safe environment, stay with the client as indicated by policy, use therapeutic communication, and notify the RN/provider according to facility procedure. Eliminate distractors: hallway disclosure violates confidentiality; routine charting alone is insufficient; the prior GI bleed is not the current issue. Verify: this is a psychosocial and safety scenario handled with conservative escalation.
C Exam trap
D Checkpoint
Question: Which option best reflects a PN/LVN-safe response under the client-needs framework?
- Independently revise the client’s suicide precautions based on personal assessment
- Discuss the client’s condition with the spouse in a public elevator because the spouse is family
- Use therapeutic communication, maintain safety, and promptly notify the RN of the client’s statement
- Reassure the client that everything will be fine and return after medication pass
Answer: C
- A: Tempting because it appears proactive, but independently changing the care plan exceeds PN/LVN authority in many settings and is unsafe for licensure-style questions.
- B: Tempting because families are involved in care, but public disclosure violates confidentiality and fails management-of-care standards.
- C: Tempting because it seems less dramatic than calling a code, but it is the correct in-scope sequence: therapeutic communication, safety action, and prompt RN notification.
- D: Tempting because reassurance sounds supportive, but false reassurance is nontherapeutic and delays needed safety escalation.
- The safest answer for a possible self-harm cue starts with safety and therapeutic presence, not reassurance alone.
- True or False: Documentation is enough when the client makes a suicide-related statement. False.
- Name 3 Management of Care themes: reporting, confidentiality, chain of command.
1.1.1.7 How to use the framework to answer mixed-category exam questions
A Explanation
The hardest foundational conflict is the mixed stem: What do you do when one scenario contains teaching, medications, lab trends, emotional distress, and safety risk all at once? The single rule that resolves it is: the best answer addresses the highest-priority active threat while staying within scope. That means you do not ignore the other needs; you simply do not handle them first. This is where the framework stops being a list and becomes a decision tool. Start with the main task, then overlay priority. Use See Fig 2. If there is no urgent threat, move toward prevention, reinforcement, comfort, and monitoring. If there is urgent instability, safety or Physiological Adaptation wins. If the stem asks about assignment or reporting process rather than direct care, Management of Care may be the better match even when a medical diagnosis is present.
WHY THIS IS TESTED: the NCLEX-PN rarely presents a perfectly “clean” category. Real clients have overlapping needs, and the exam measures whether you can choose the best next step rather than the best eventual plan.
This is also where students overstep scope. A provider-level answer can sound impressive, but NCLEX-PN rewards the bedside practical nurse action: focused assessment, immediate safety intervention, reinforce existing teaching, administer ordered treatment within policy, document, and report. The wrong answer is often correct for an RN, provider, or for a later stage of care.
B Worked example
A 76-year-old long-term care resident with dementia, heart failure, and dysphagia becomes more short of breath during lunch. The resident is coughing with thin liquids, has bilateral ankle edema, and the daughter asks whether the influenza vaccine is due. The medication cart is also waiting for routine noon medications. Identify task: choose the safest next action. Extract key facts: dyspnea during swallowing, aspiration risk, existing heart failure, preventive question from family, and routine meds creating time pressure. Apply rule: immediate airway/breathing concern and safety risk dominate; stop oral intake, keep the client safe, assess focused respiratory status, and notify the RN/provider per facility protocol. Eliminate distractors: vaccine teaching is lower priority; routine medications can wait until the breathing issue is addressed; edema history is relevant background but not the immediate event. Verify: the framework points to Safety and Infection Control plus Physiological Adaptation, with breathing risk taking priority.
C Exam trap
D Checkpoint
Question: A client with newly diagnosed diabetes asks about foot care while the nurse notices the client is diaphoretic and shaking before lunch. Which framework-guided action is most appropriate first?
- Reinforce daily foot inspection teaching using a handout
- Check the client’s blood glucose and follow the established hypoglycemia protocol
- Document the symptoms and recheck in 30 minutes
- Ask the provider to change the insulin prescription
Answer: B
- A: Tempting because teaching is needed, but Health Promotion and Maintenance does not outrank an immediate possible hypoglycemic event.
- B: Tempting because it delays teaching, but it is correct because the active physiologic and safety threat must be addressed first using established protocol.
- C: Tempting because re-evaluation matters, but documentation without intervention delays care for a potentially unstable client.
- D: Tempting because the insulin may need adjustment later, but changing therapy is provider-level and outside the PN/LVN role.
Exam Traps & Differentiators
Exam takeaway: The best answer often loses only because it belongs to the wrong category or wrong priority level.
flowchart TD
A[Teaching in stem] --> B{Immediate threat present?}
B -->|Yes| C[Avoid teaching first]
B -->|No| D[Choose Health Promotion if prevention or reinforcement is the task] E[Lab trend in stem] --> F{Acute instability now?}
F -->|Yes| G[Choose Physiological Adaptation]
F -->|No| H[Choose Reduction of Risk Potential] I[Reporting/documenting in stem] --> J{Main task is coordination, confidentiality, chain of command?}
J -->|Yes| K[Choose Management of Care]
J -->|No| L[May belong to another category with reporting as the action] Exam takeaway: When multiple needs appear together, follow ABCs and safety before comfort, teaching, or routine tasks.
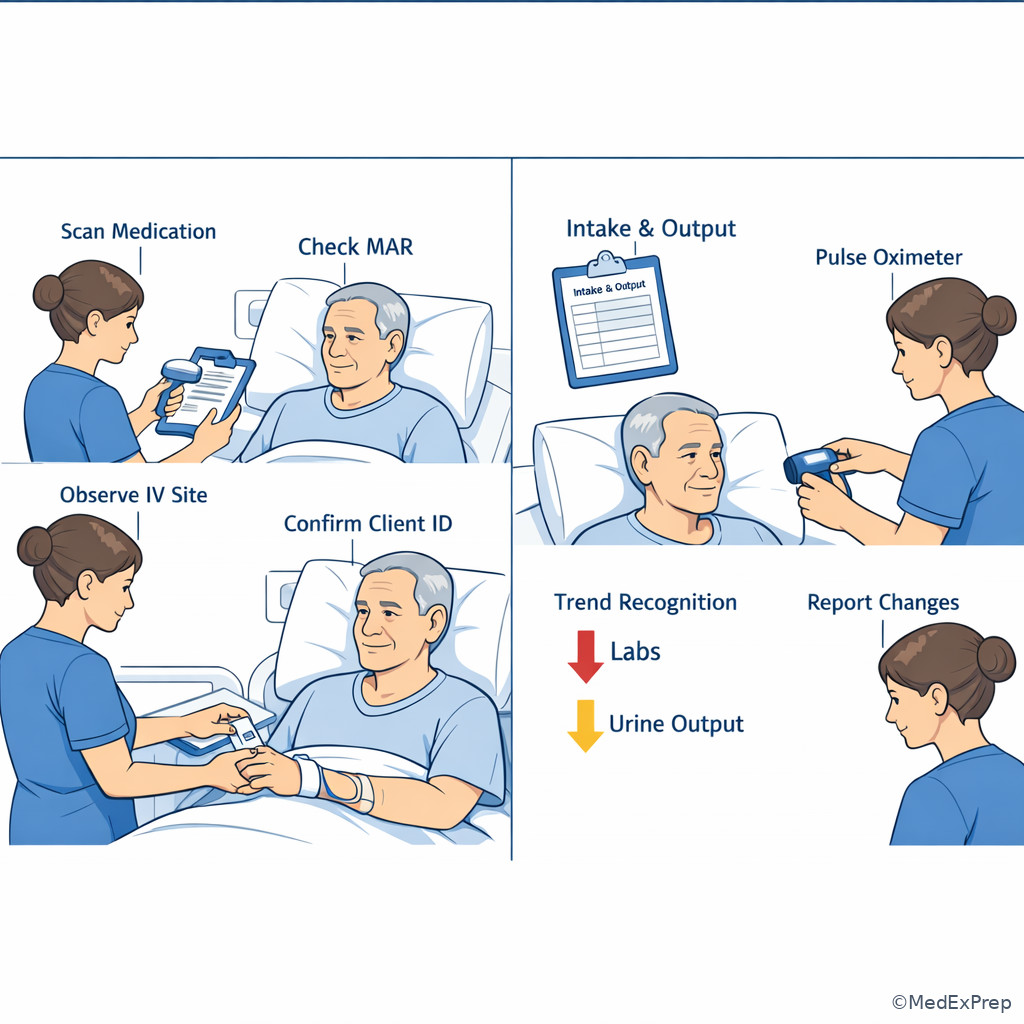
Most common wrong answer and why: The most common wrong answer is a true statement or reasonable nursing action that is either lower priority, outside PN/LVN scope, or aimed at the wrong client-needs category. See Fig 3 for the choose-vs-avoid pattern and See Fig 4 for the urgency overlay.
| Stem clue | Think this category | Not this one | Discriminator |
|---|---|---|---|
| Reinforce vaccines, screening, developmental guidance | Health Promotion and Maintenance | Basic Care and Comfort | Prevention/teaching versus hands-on routine care |
| Intake/output trend, lab trend, complication watch | Reduction of Risk Potential | Physiological Adaptation | Monitoring before crisis versus active instability |
| Confidentiality, reporting, assignment, chain of command | Management of Care | Safety and Infection Control | System/process action versus injury/infection prevention |
| Medication adverse effect, administration check, IV site issue | Pharmacological and Parenteral Therapies | Basic Care and Comfort | Drug/parenteral safety versus routine physical support |
| Crying, grief, anxiety, coping, therapeutic response | Psychosocial Integrity | Health Promotion and Maintenance | Emotional support versus preventive teaching |
| Dyspnea, sudden confusion, chest pain, hemorrhage | Physiological Adaptation | Reduction of Risk Potential | Acute deterioration now |
Looks similar but isn't:
| Confusable pair | Looks similar because | Actually different because | Exam cue to break the tie |
|---|---|---|---|
| Health Promotion vs Basic Care | Both may involve daily care and teaching | One is prevention/anticipated reinforcement; the other is direct comfort and ADL support | Ask whether the answer teaches or physically assists |
| Reduction of Risk vs Physiological Adaptation | Both involve body-system monitoring | One watches for worsening; the other responds to active deterioration | Look for words like sudden, severe, acute, unstable |
| Management of Care vs Safety | Both feel “protective” | One is coordination/reporting/legal process; the other is hazard prevention | If chain of command/confidentiality is central, choose management |
| Psychosocial vs Physiologic priority | Distress often coexists with symptoms | Airway, bleeding, and instability outrank emotional support first | ABCs override when present |
- If the stem says “reinforce teaching,” think Health Promotion and Maintenance unless an urgent safety or physiologic threat is present.
- If the stem says “trend,” “monitor,” or “report a change over time,” think Reduction of Risk Potential.
- If the stem says “sudden,” “severe,” “new confusion,” “respiratory distress,” or “heavy bleeding,” think Physiological Adaptation first.
- If the stem says “who should be told,” “what should be reported,” “confidentiality,” or “assignment,” think Management of Care.
- If the stem says “therapeutic response,” “coping,” “grief,” or “nonjudgmental communication,” think Psychosocial Integrity.
- If the stem says “fall risk,” “precautions,” “PPE,” or “error prevention,” think Safety and Infection Control.
Cross-topic trap alert: In the upcoming Priority Frameworks lesson, you will see similar answer sets where all four actions are appropriate but only one is first. The framework in this lesson tells you what kind of need is being tested; priority frameworks tell you which of several correct needs comes first.
Tables
| Category | What the exam usually asks | Typical PN/LVN action | Common wrong move |
|---|---|---|---|
| Management of Care | Report, assign, protect privacy, follow chain of command | Communicate findings promptly, document accurately, follow policy | Trying to independently redesign the plan |
| Safety and Infection Control | Prevent falls, errors, exposure, transmission | Use precautions, environmental safeguards, verification checks | Teaching later while ignoring an active hazard |
| Health Promotion and Maintenance | Reinforce routine teaching, screening, prevention, development | Support established teaching and expected care routines | Choosing it when the client is unstable now |
| Psychosocial Integrity | Therapeutic communication, coping, crisis support | Use nonjudgmental responses and maintain emotional safety | False reassurance or arguing with the client |
| Basic Care and Comfort | Mobility, hygiene, elimination, nutrition, comfort | Assist with ADLs and basic physical care | Confusing routine assistance with prevention teaching |
| Pharmacological and Parenteral Therapies | Medication checks, adverse effects, infusion issues | Administer safely, monitor, hold/report per order/policy | Ignoring side effects because the drug is scheduled |
| Reduction of Risk Potential | Monitor complications, labs, trends | Recognize and report early deterioration clues | Waiting until a trend becomes a crisis |
| Physiological Adaptation | Acute instability, urgent physiologic change | Take immediate in-scope action and escalate | Delaying for teaching, routine meds, or documentation alone |
| Question wording | Best framework lens | Best first thought |
|---|---|---|
| Most appropriate response | Psychosocial Integrity or Management | Is this therapeutic and within scope? |
| Best next step | Any category | What is the highest-priority active need? |
| Most important to report | Management or Reduction of Risk/Adaptation | Is there urgent change or a critical trend? |
| Requires immediate clarification | Safety/Pharmacology/Management | Is the order unsafe, incomplete, or outside policy? |
| Best evidence of understanding | Health Promotion or Pharmacology | What teaching point reflects safe reinforcement? |
| Priority client | Adaptation or Safety | Who has acute ABC/safety risk now? |
| Scenario | Classification | Why |
|---|---|---|
| Client asks how to prevent pressure injuries at home | Health Promotion and Maintenance | Prevention teaching reinforcement |
| Client needs turning and heel protection during bed rest | Basic Care and Comfort | Direct routine physical support |
| Client on heparin has oozing at IV site and easy bruising | Pharmacological and Parenteral Therapies | Medication adverse-effect monitoring |
| Post-op blood pressure drops slowly over several hours with rising pulse | Reduction of Risk Potential | Trend suggesting complication before collapse |
| Client develops sudden stridor after medication administration | Physiological Adaptation | Acute airway emergency |
| Family requests report details in the waiting room | Management of Care | Confidentiality and communication process issue |
| Client on contact precautions needs dedicated equipment | Safety and Infection Control | Transmission prevention |
| Client says “No one cares if I live” after bereavement | Psychosocial Integrity | Therapeutic communication and safety assessment/escalation |
Exam takeaway: Start with urgency, then classify the need, then choose the safest in-scope action.
flowchart TD
A[Read the question ask] --> B{Immediate ABC or severe safety threat?}
B -->|Yes| C[Physiological Adaptation or Safety and Infection Control]
B -->|No| D{Main task is reporting, confidentiality, assignment, or chain of command?}
D -->|Yes| E[Management of Care]
D -->|No| F{Main task is prevention or teaching reinforcement?}
F -->|Yes| G[Health Promotion and Maintenance]
F -->|No| H{Main task is coping or therapeutic response?}
H -->|Yes| I[Psychosocial Integrity]
H -->|No| J[Physiological Integrity subcategory]
J --> J1[Basic Care and Comfort]
J --> J2[Pharmacological and Parenteral Therapies]
J --> J3[Reduction of Risk Potential] Exam takeaway: Distinguish medication safety tasks from trend-monitoring tasks even when they involve the same client.
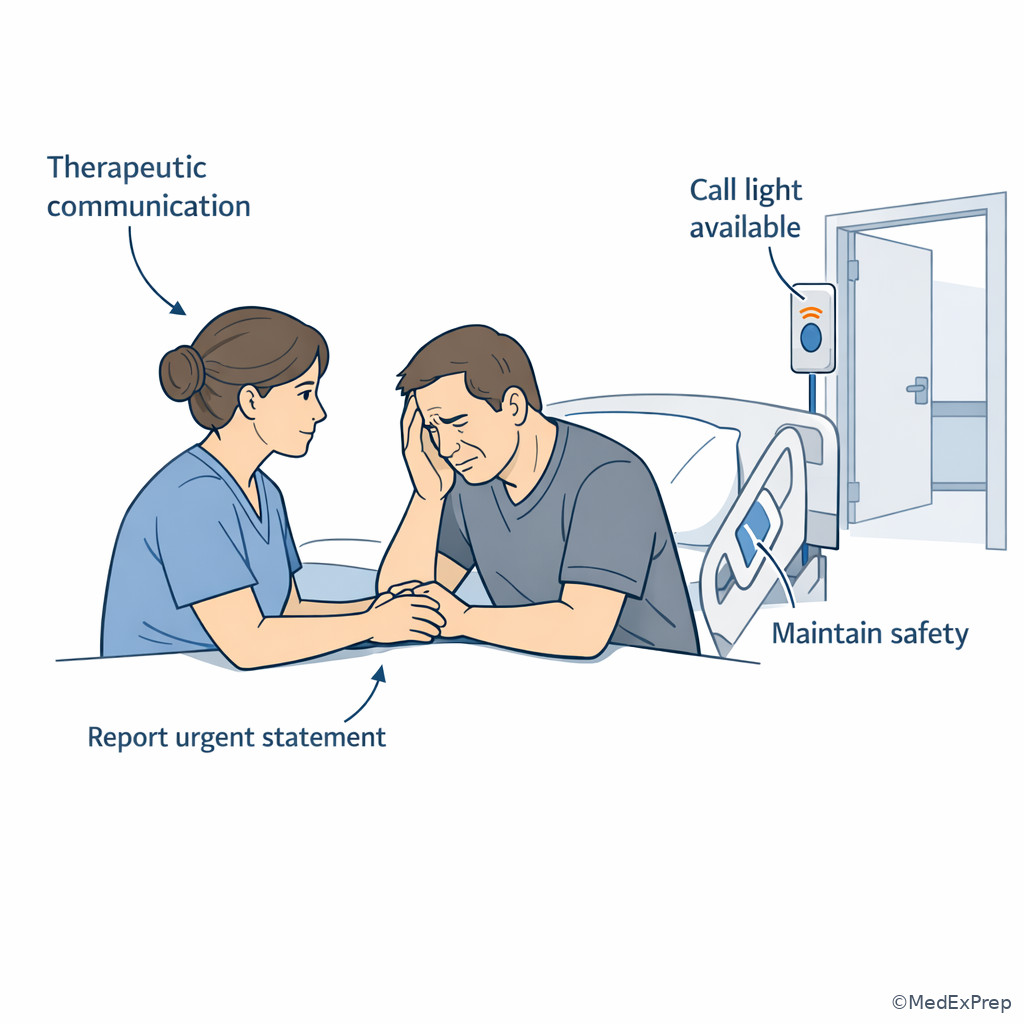
Exam takeaway: Psychosocial support is essential, but immediate safety still leads when self-harm or escalation cues are present.
Algorithm / Approach
Use See Fig 5 as your default mental algorithm. In the next two topics, you will add more formal steps for cue recognition and prioritization, but this framework already lets you eliminate many distractors quickly.
Rapid Review
- Management of Care → reporting/confidentiality/chain-of-command cue beats diagnosis in the stem.
- Safety and Infection Control → hazards and precautions outrank routine teaching.
- Health Promotion and Maintenance → prevention and reinforcement, not acute rescue.
- Psychosocial Integrity → therapeutic communication, unless ABC/safety threat overrides.
- Basic Care and Comfort → direct ADL and comfort support, not prevention counseling.
- Pharmacological and Parenteral Therapies → medication effect or administration issue is the key discriminator.
- Reduction of Risk Potential → trend recognition before collapse.
- Physiological Adaptation → sudden deterioration now.
- Mixed stem → highest-priority active threat decides the category.
- Teaching in the stem → do not choose it first if instability is present.
- Documentation option → necessary, but rarely enough by itself for urgent findings.
- Scope filter → reject provider-level or RN-only comprehensive planning answers.
- Priority client questions → unstable beats stable, actual problem beats potential problem.
- Client-needs framework → first sorts the problem; later frameworks rank competing actions.
Self-check quiz
1. A 66-year-old client in a clinic with hypertension and obesity asks when to return for a routine vaccine. The client is stable, chatting comfortably, and waiting for printed instructions. Which framework category best fits the nurse’s task?
- Health Promotion and Maintenance
- Basic Care and Comfort
- Reduction of Risk Potential
- Management of Care
2. A 79-year-old long-term care resident with cataracts and osteoarthritis says, “I’m afraid I’ll trip going to the bathroom tonight.” The resident also has a routine bowel regimen due later and a family teaching packet at bedside. Which framework category is the best match for the immediate nursing task?
- Safety and Infection Control
- Health Promotion and Maintenance
- Psychosocial Integrity
- Pharmacological and Parenteral Therapies
3. A 58-year-old client with heart failure and chronic kidney disease has gained 2 kg in 2 days. During the shift, urine output has decreased from the prior day, and the client remains alert with oxygen saturation 95% on room air. Which action best matches the client-needs framework for the most important current task?
- Place the client in high-Fowler position and call a rapid response team
- Continue to monitor intake/output trends and report the change to the RN
- Reinforce low-sodium diet teaching before dinner
- Assist with a warm blanket and repositioning for comfort
4. A 24-year-old postpartum client with a history of anxiety says she feels scared about newborn care. At the same time, the nurse notes the client is pale, the fundus is boggy, and a perineal pad is saturated in 10 minutes. Which is the most appropriate next action?
- Stay with the client, address the acute bleeding using established measures, and notify the RN immediately
- Provide detailed breastfeeding teaching to reduce the client’s anxiety
- Document the findings and recheck the client after finishing other assigned tasks
- Ask the provider for a new medication order before assessing further
5. A 70-year-old client with diabetes, peripheral vascular disease, and mild neuropathy receives scheduled insulin before lunch. Ten minutes later, the client becomes diaphoretic, shaky, and irritable. The client also asks for foot-care teaching materials. Which action is most appropriate?
- Reinforce foot-care teaching while lunch is delivered
- Check the blood glucose and follow the established hypoglycemia protocol
- Document the symptoms because the insulin was given as ordered
- Request that the provider change the insulin prescription immediately
6. A practical nurse is caring for a 61-year-old client with COPD, hypertension, and depression who says, “I’m tired of this.” The client is speaking in full sentences, oxygen saturation is 93% on prescribed oxygen, and no self-harm plan is expressed. Which nursing action is the safest and most appropriate within PN/LVN scope?
- Initiate a new suicide precaution protocol independently based on personal judgment
- Use therapeutic communication to explore the statement, maintain safety, and report concerning findings to the RN
- Tell the client that positive thinking will help and continue medication administration
- Ask the spouse to stay and monitor the client while the nurse leaves the unit
7. A 73-year-old postoperative client with coronary artery disease and chronic anemia is alert and reports incisional pain 5/10. Over the last 4 hours, blood pressure has trended down from 132/78 to 104/62 mm Hg, pulse has risen from 82 to 104/min, and urine output has declined. Which option best reflects the PN/LVN’s priority framework-based action?
- Administer the prescribed analgesic first because uncontrolled pain raises pulse rate
- Recognize a complication trend, perform focused reassessment, and promptly report to the RN
- Encourage oral fluids and recheck vital signs at the end of the shift
- Independently diagnose early hemorrhagic shock and prepare a transfusion consent form
8. A 6-year-old client with asthma, eczema, and recent viral illness is on a pediatric unit with an established bronchodilator order. The child is anxious, using accessory muscles, and has audible wheezing; oxygen saturation is 88% on room air. The parent asks whether the child can receive school vaccine records before discharge. Which is the best next action for the practical nurse?
- Print the vaccine record first because discharge paperwork prevents delays later
- Assist the child to a position that eases breathing, apply ordered oxygen/interventions per policy, and notify the RN of the respiratory change
- Explain that anxiety often worsens asthma and coach the parent to calm the child before any intervention
- Call the provider to request a different bronchodilator before assessing the child further
Answer key
1. Correct answer: A
- A: Tempting because vaccine follow-up can feel routine, and it is correct because the stem centers on prevention and teaching reinforcement for a stable client. The discriminating clue is the routine vaccine question with no acute problem. Source: NCSBN test plan framework; Saunders NCLEX review.
- B: Tempting because clinic teaching often includes practical daily care, but Basic Care and Comfort focuses on direct physical support like hygiene, mobility, nutrition, and elimination. The clue eliminating it is that the nurse is not assisting with ADLs. Source: Saunders; Lewis Medical-Surgical Nursing.
- C: Tempting because follow-up can reduce future risk, but Reduction of Risk Potential is about monitoring for complications or trends, not routine prevention. The key clue is client stability and absence of a complication trend. Source: NCSBN; Saunders.
- D: Tempting because follow-up appointments involve healthcare systems, but the main task is not coordination, assignment, or reporting. The clue eliminating it is the direct prevention teaching ask. Source: NCSBN; ANA standards on role and communication.
2. Correct answer: A
- A: Tempting because it seems too obvious, and it is correct because the immediate task is preventing a nighttime fall. The discriminating clue is fear of tripping during bathroom ambulation tonight. Source: NCSBN safety focus; Saunders.
- B: Tempting because the teaching packet is present, but prevention teaching is lower priority than an active fall risk. The clue eliminating it is the word “immediate.” Source: NCSBN; Lewis.
- C: Tempting because fear is an emotion, but the question is not asking for therapeutic communication as the primary task; it asks about the immediate need. The clue eliminating it is the concrete injury risk. Source: Saunders; ANA standards.
- D: Tempting because a bowel regimen is due later, but no medication issue is central right now. The clue eliminating it is that the medication is routine and later. Source: Saunders.
3. Correct answer: B
- A: Tempting because high-Fowler positioning is correct for dyspnea and rapid response reflects urgency, but the client is oxygenating adequately and is not described as acutely unstable. The discriminating clue is stable oxygen saturation and alert mental status. Source: NCSBN prioritization principles; Lewis.
- B: Tempting because it feels less dramatic, and it is correct because the stem describes a complication trend—weight gain, declining urine output—without current collapse. The discriminating clue is a gradual pattern over time. Source: NCSBN; Saunders.
- C: Tempting because diet teaching is appropriate for heart failure, but routine education is lower priority than recognizing worsening fluid status. The clue eliminating it is the objective trend change. Source: Saunders.
- D: Tempting because comfort measures are always reasonable, but they do not address the most important current clinical cue. The clue eliminating it is the rising risk of fluid overload. Source: ANA standards; Lewis.
4. Correct answer: A
- A: Tempting because it interrupts communication-based support, and it is correct because acute postpartum bleeding threatens circulation and requires immediate established interventions plus RN notification. The discriminating clue is saturated pad in 10 minutes with boggy fundus and pallor. Source: NCSBN ABC/safety focus; Lewis maternal-newborn content; Saunders.
- B: Tempting because anxiety and newborn teaching are real needs, but they are lower priority than hemorrhage risk. The clue eliminating it is active excessive bleeding. Source: Saunders.
- C: Tempting because documentation is always required, but it is incorrect as a first action because it delays urgent care. The discriminating clue is signs of acute circulatory compromise. Source: ANA standards; NCSBN.
- D: Tempting because uterotonic therapy may be needed, but asking for a new order before focused action and escalation delays response; also the PN/LVN does not independently direct treatment changes. The clue eliminating it is the need for immediate bedside intervention first. Source: NCSBN; ANA standards.
5. Correct answer: B
- A: Tempting because diabetes teaching is important and the client asked for it, but probable hypoglycemia requires immediate assessment and action first. The discriminating clue is diaphoresis, shakiness, and irritability after insulin. Source: Saunders; Lewis.
- B: Tempting because it delays education, and it is correct because the practical nurse should address the active physiologic problem using the established protocol. The discriminating clue is symptomatic possible hypoglycemia. Source: NCSBN prioritization; medication safety guidance in Saunders.
- C: Tempting because the insulin was administered appropriately, but documentation alone does not treat a potential adverse effect. The clue eliminating it is the presence of symptoms now. Source: ANA standards; NCSBN.
- D: Tempting because the insulin regimen may later need adjustment, but requesting a prescription change is not the immediate nursing action and exceeds role expectations. The clue eliminating it is the current bedside instability. Source: ANA standards; NCSBN scope framing.
6. Correct answer: B
- A: Tempting because possible self-harm statements require seriousness, but independently initiating a new protocol based on personal judgment exceeds typical PN/LVN authority and bypasses the chain of communication. The discriminating clue is the scope-of-practice issue, not just the client statement. Source: ANA standards; NCSBN role expectations.
- B: Tempting because it sounds less decisive, and it is correct because it combines therapeutic communication, safety awareness, and appropriate reporting within PN/LVN scope. The discriminating clue is no explicit plan but a concerning statement that still requires exploration and reporting. Source: NCSBN psychosocial integrity and safety framework; Saunders.
- C: Tempting because reassurance feels kind and medication administration is routine, but false reassurance is nontherapeutic and ignores a concerning cue. The discriminating clue is the emotionally loaded statement. Source: Saunders therapeutic communication review; ANA standards.
- D: Tempting because family presence can be supportive, but monitoring a potentially at-risk client cannot be shifted informally to family while the nurse leaves. The discriminating clue is the nurse’s ongoing responsibility for safety and escalation. Source: NCSBN safety principles; ANA standards.
7. Correct answer: B
- A: Tempting because pain can raise pulse and treating pain is a valid nursing action, but it is the right intervention at the wrong priority. The discriminating clue is the downward blood pressure trend with declining urine output over hours. Source: NCSBN priority and trend recognition; Lewis.
- B: Tempting because the client is still alert and pain is present, and it is correct because the data suggest an evolving complication requiring focused reassessment and prompt RN report. The discriminating clue is the combined trend of falling blood pressure, rising pulse, and less urine. Source: Saunders; NCSBN.
- C: Tempting because fluids and reassessment are common postoperative measures, but delaying until end of shift ignores a meaningful deterioration pattern. The discriminating clue is progressive change rather than one isolated vital sign. Source: ANA standards; Lewis.
- D: Tempting because the data raise concern for hemorrhage, but independently diagnosing shock and preparing consent exceed the PN/LVN role. The discriminating clue is the out-of-scope action language. Source: NCSBN scope guardrails; ANA standards.
8. Correct answer: B
- A: Tempting because discharge paperwork is a real nursing responsibility, but it is lower priority than an active breathing problem. The discriminating clue is oxygen saturation 88% with accessory muscle use. Source: NCSBN ABCs; Saunders pediatric review.
- B: Tempting because it postpones the parent’s request, and it is correct because the child has acute respiratory compromise requiring immediate in-scope support and RN notification. The discriminating clue is audible wheezing plus low oxygen saturation. Source: NCSBN; Lewis.
- C: Tempting because anxiety can worsen asthma symptoms, but coaching alone is insufficient when objective respiratory distress is present. The discriminating clue is the objective hypoxemia. Source: Saunders.
- D: Tempting because medication escalation may be needed later, but the practical nurse should first carry out ordered interventions and report the change rather than request a new prescription independently. The discriminating clue is the need for immediate bedside action within scope. Source: ANA standards; NCSBN scope framing.