Why it matters
- NAPLEX questions often hide the real task inside extra details; the medication-related problem framework tells you what the pharmacist must solve first.
- The same drug can create different problems in different patients: one stem tests missing indication, another tests underdosing, another tests safety, and another tests adherence.
- This framework prevents out-of-scope thinking by keeping your focus on pharmacist actions: review, clarify, recommend, hold, monitor, counsel, and escalate when needed.
- It is the foundation for upcoming topics on best next pharmacist action and order verification priorities.
Key Terms & Must-Know Facts
1.1.1.1 Key terms
- Medication-related problem (MRP): Any issue preventing a medication from being indicated, effective, safe, or usable.
- Indication: Whether a medication is needed and appropriate for a recognized treatment goal.
- Untreated indication: A condition needing drug therapy but no appropriate medication is present.
- Unnecessary therapy: A medication exists without a current valid reason, or duplicates another therapy.
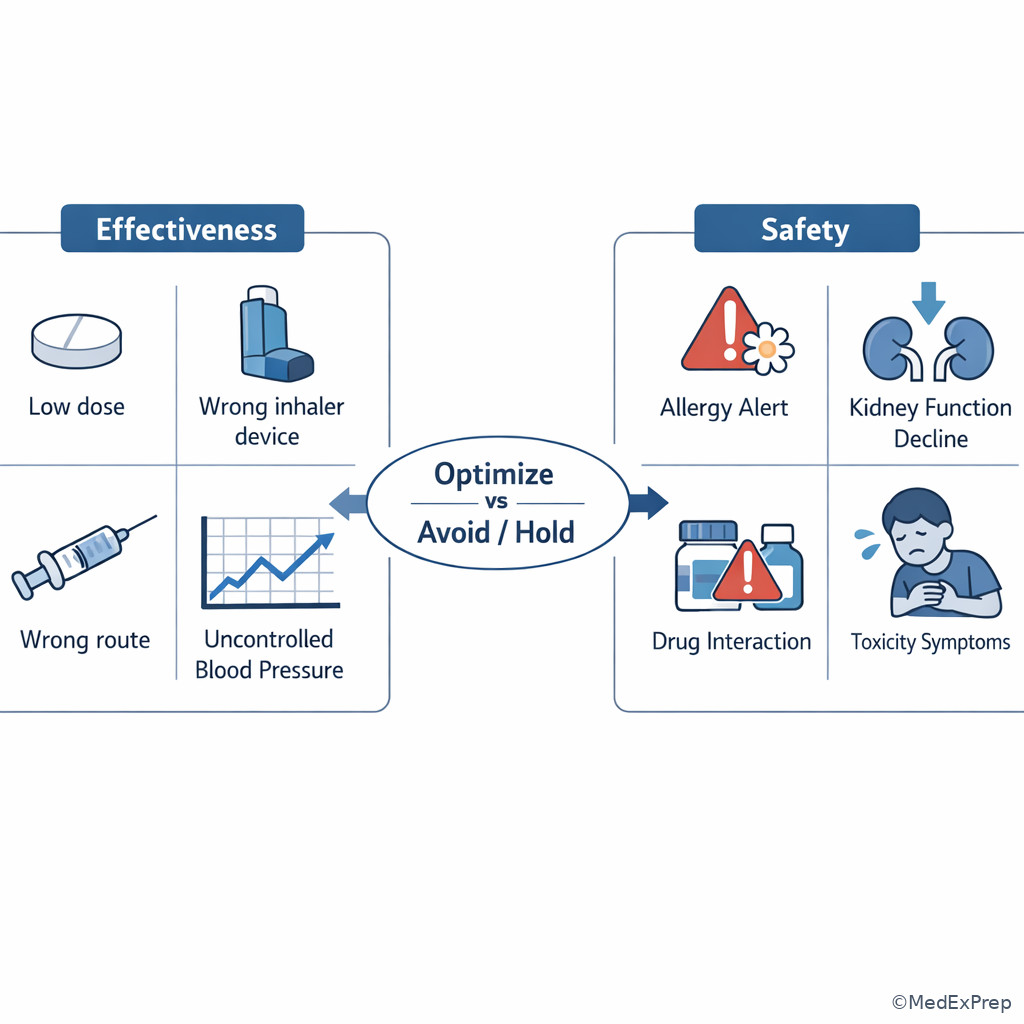
- Effectiveness: Whether the therapy can achieve the desired outcome for this patient.
- Subtherapeutic dose: Dose, route, interval, formulation, or duration is insufficient.
- Wrong drug for condition: A medication is used, but it is not the best therapeutic choice for the patient’s problem.
- Safety: Whether risks outweigh benefits for this patient at this dose and under these circumstances.
- Adverse drug reaction: Harmful or intolerable effect at usual doses.
- Dose too high: Toxicity risk from dose, accumulation, interaction, organ dysfunction, or duplicate exposure.
- Adherence/nonadherence: Failure to take or obtain therapy as intended.
- Administration barrier: Patient cannot use dosage form, device, timing, or technique correctly.
- Monitoring failure: Needed labs, vitals, symptoms, or follow-up are missing.
- Clarification threshold: The point at which the pharmacist should stop verification and obtain missing or conflicting information.
1.1.1.2 Must-know facts
- The four high-yield buckets are indication, effectiveness, safety, and adherence/practical use.
- Ask first: Does the patient need this drug? before asking whether the dose is correct.
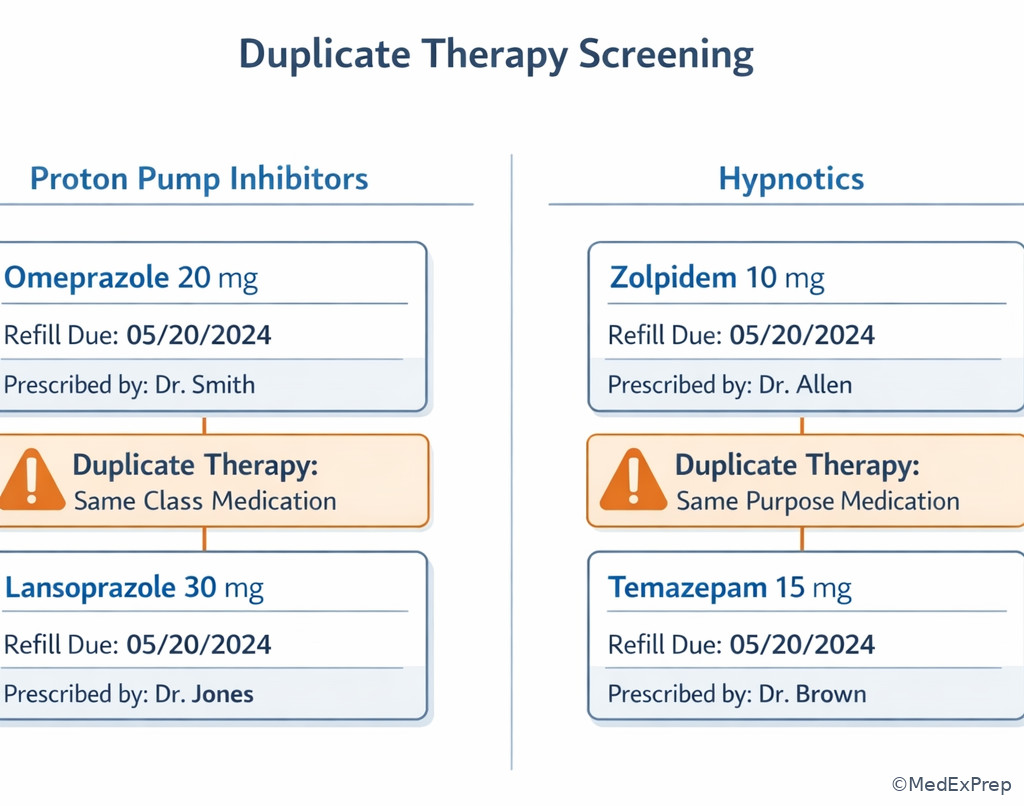
- Two drugs for the same purpose may signal duplicate/unnecessary therapy, not stronger treatment.
- Normal dose does not mean safe dose in renal impairment, hepatic impairment, older age, pregnancy, or major interactions.
- A drug can be ineffective even when “on board” if the dose, formulation, route, interval, or device technique is wrong.
- Adherence problems are medication-related problems even when the prescription itself is technically correct.
- When the order is incomplete or unsafe, the pharmacist action is hold and clarify, not guess.
- Urgent toxicity, anaphylaxis, severe bleeding, or major interaction risk shifts the action from routine verification to escalation.
| MRP category | Core question | Typical stem clue | Likely pharmacist action |
|---|---|---|---|
| Indication | Should a drug be started, stopped, or de-duplicated? | No therapy for a clear need, or duplicate therapy without justification | Recommend initiation, discontinuation, or clarification |
| Effectiveness | Can this regimen work as written? | Poor control, wrong drug, low dose, wrong formulation, wrong route | Recommend alternative, titration, or formulation change |
| Safety | Is harm likely in this patient? | Allergy, contraindication, interaction, organ dysfunction, high dose, toxicity | Hold, clarify, recommend safer option, monitor, escalate if urgent |
| Adherence/practical use | Can the patient actually use it correctly? | Missed doses, cost, technique errors, confusion, refill gaps | Counsel, simplify, troubleshoot access, reinforce monitoring |
Exam takeaway: Sort the stem into indication, effectiveness, safety, or adherence before choosing a pharmacist action.
flowchart TD
A[Medication order or patient case] --> B{First question}
B -->|Drug needed?| C[Indication]
B -->|Will it work?| D[Effectiveness]
B -->|Could it harm?| E[Safety]
B -->|Can patient use it?| F[Adherence or practical use]
C --> C1[Untreated indication]
C --> C2[Unnecessary or duplicate therapy]
D --> D1[Wrong drug]
D --> D2[Dose too low or wrong formulation]
E --> E1[Adverse effect or contraindication]
E --> E2[Dose too high or interaction]
F --> F1[Nonadherence]
F --> F2[Technique or access barrier] Use this as your first sorting tool. See Fig 1.
Core content
1.1.1.3 Foundational sorting: identify the primary medication-related problem
A Explanation
The main decision conflict is whether the stem is really about starting/stopping a therapy or about fixing an existing therapy. The single rule that resolves it is this: if the patient lacks an appropriate therapy or has therapy without need, classify it as indication first. Only after indication is settled should you move to effectiveness, safety, or adherence. WHY THIS IS TESTED: NAPLEX stems often include a distracting abnormal lab or side effect, but the most urgent or primary pharmacist task is recognizing that the patient either needs therapy that is missing or is receiving a therapy that should not be there.
Choose untreated indication when there is a clear therapeutic need and no appropriate medication exists. Choose unnecessary therapy when the drug has no current indication, duplicates another drug for the same purpose, or is treating an avoidable side effect of another medication instead of the root cause. Reject “dose too low” when the more basic problem is that the chosen drug is not needed at all. Reject “adherence” when the patient is perfectly adherent to a medication that should never have been continued.
Exam takeaway: When multiple issues appear, choose the first problem that changes whether therapy should exist at all.
flowchart TD
A[Case stem] --> B{Is there a clear untreated condition?}
B -->|Yes| C[Untreated indication]
B -->|No| D{Is there a duplicate or no-current-need drug?}
D -->|Yes| E[Unnecessary therapy]
D -->|No| F{Therapy present but not meeting goal?}
F -->|Yes| G[Effectiveness problem]
F -->|No| H{Risk outweighs benefit?}
H -->|Yes| I[Safety problem]
H -->|No| J[Adherence or use barrier] When several answer choices look plausible, return to the sequence in See Fig 2.
B Worked example
A 67-year-old man presents to the pharmacy for refill synchronization. His profile includes metformin 1000 mg by mouth twice daily, insulin glargine 24 units nightly, lisinopril 20 mg daily, atorvastatin 40 mg nightly, and duplicate acid suppression with omeprazole 20 mg daily plus pantoprazole 40 mg daily from a recent discharge. He has type 2 diabetes, hypertension, and GERD. His wife reports excellent adherence. A recent fasting glucose of 168 mg/dL is listed, which tempts you to focus on diabetes intensification. The board-style task asks for the most likely medication-related problem requiring clarification before routine refill.
Reasoning chain: Identify task: name the primary MRP. Extract key facts: duplicate PPIs, no evidence of two different indications, strong adherence, elevated glucose but already on active therapy. Apply rule: ask first whether any drug is unnecessary. Omeprazole and pantoprazole are therapeutic duplicates for the same purpose. Eliminate distractors: “dose too low” for diabetes is tempting because glucose is above goal, but that is not the most basic problem requiring refill clarification. “Nonadherence” is contradicted by refill sync and spouse report. Verify: the clearest immediate category is unnecessary/duplicate therapy under indication.
C Exam trap
D Checkpoint
Question: A 58-year-old woman with atrial fibrillation, osteoarthritis, and chronic insomnia brings a profile containing apixaban 5 mg by mouth twice daily, ibuprofen 600 mg three times daily as needed, and two active sleep agents: trazodone 50 mg nightly and zolpidem 10 mg nightly from different prescribers. She reports taking all medications exactly as labeled. Which medication-related problem is the best primary classification for the two sleep agents?
- A. Untreated indication — Tempting because insomnia is present, but incorrect because therapy is already present; the issue is not absence of treatment.
- B. Unnecessary therapy — Correct because two hypnotic therapies for the same symptom raise duplicate-therapy concern unless a clear rationale exists.
- C. Dose too low — Tempting because insomnia persists in many patients, but incorrect because the discriminating clue is duplication, not underdosing.
- D. Nonadherence — Tempting because sleep medications are often taken inconsistently, but incorrect because she reports taking them exactly as directed and the profile itself shows the problem.
1.1.1.4 Foundational refinement: distinguish effectiveness problems from safety problems
A Explanation
The central conflict here is choosing between “this therapy is not enough” and “this therapy may cause harm”. The single rule that resolves it is this: if the regimen could plausibly work but patient-specific risk makes it dangerous, choose safety; if the regimen is too weak, wrong, or poorly matched to the condition, choose effectiveness. WHY THIS IS TESTED: Many NAPLEX stems give an abnormal value and a risky comorbidity at the same time. The exam wants to know whether you prioritize better control or harm prevention.
Choose effectiveness when the drug is the wrong agent, the dose is too low, the interval is too long, the route is inappropriate, or the dosage form prevents adequate exposure. Choose safety when the same regimen creates toxicity risk through renal accumulation, drug interaction, contraindication, allergy, excessive dose, duplicate exposure, or adverse effect pattern. A key discriminator is whether you would increase/change therapy versus hold/reduce/avoid therapy. See Fig 3 for the compare-and-choose framework.
| Feature | Effectiveness problem | Safety problem |
|---|---|---|
| Main question | Why is the regimen not achieving the goal? | Why might the regimen harm this patient? |
| Usual next step | Increase, switch, optimize, or change formulation | Hold, reduce, avoid, monitor, or escalate |
| Typical clues | Persistent symptoms, poor control, underdose, wrong route | Allergy, interaction, organ dysfunction, toxicity signs |
| Common distractor | Mild side effects that do not outweigh benefit | Single uncontrolled value that tempts dose increase |
| Best framing | Therapy exists but cannot do the job | Therapy exists but may be dangerous |
Exam takeaway: The best answer often hinges on whether the pharmacist should intensify therapy or prevent harm first.
B Worked example
A 74-year-old woman with heart failure, chronic kidney disease, and atrial fibrillation is discharged on digoxin 0.25 mg by mouth daily, furosemide 40 mg daily, and amiodarone 200 mg daily. Her serum creatinine increased from 0.9 to 1.6 mg/dL over two months, and she now reports nausea and yellow vision changes. A BNP value remains elevated, which tempts you to focus on heart failure effectiveness. The task asks for the most likely medication-related problem requiring immediate pharmacist intervention.
Reasoning chain: Identify task: classify the dominant problem. Extract key facts: older age, worsening renal function, digoxin dose, amiodarone interaction, classic digoxin toxicity symptoms. Apply rule: when a regimen could cause harm and the fix is reduction/hold rather than intensification, choose safety. Eliminate distractors: “effectiveness problem” is tempting because heart failure is not fully controlled, but elevated BNP is noise compared with toxicity clues. “Adherence” is not supported. Verify: the primary problem is safety: dose too high / interaction-related toxicity risk.
C Exam trap
D Checkpoint
Question: A 63-year-old man with type 2 diabetes, CKD stage 4, and neuropathy presents with a refill request for gabapentin 900 mg by mouth three times daily. He reports new excessive sedation and unsteady gait but says his foot pain is still bothersome. Which is the best primary medication-related problem category?
- A. Untreated indication — Tempting because neuropathy remains symptomatic, but incorrect because the patient already has therapy for the indication.
- B. Dose too low — Tempting because pain persists, but incorrect because CKD plus sedation and gait instability point to accumulation and harm.
- C. Safety problem — Correct because renal impairment and toxicity symptoms make the dominant issue dose-related harm.
- D. Nonadherence — Tempting because variable pain control can reflect inconsistent use, but incorrect because the discriminating clues are adverse effects with organ dysfunction.
- The first category to consider when a drug is missing or duplicated is indication.
- True or False: A normal labeled dose can still be a safety problem in renal impairment. True.
- Name the two broad questions that separate effectiveness from safety: Will it work? and Could it harm?
1.1.1.5 Applied patient review: find the clue that reclassifies the problem
A Explanation
This section moves from category names to pattern recognition in real profiles. The decision conflict is whether the patient data are merely background or the single discriminating clue that changes the MRP category. The rule: when a patient factor changes appropriateness of the regimen—renal function, allergy, age, pregnancy, comorbidity, or interacting medication—that factor can reclassify a problem from routine dosing to safety or from apparent failure to practical-use failure. WHY THIS IS TESTED: board-style cases frequently add one line of data that flips the answer from simple dose adjustment to hold-and-clarify.
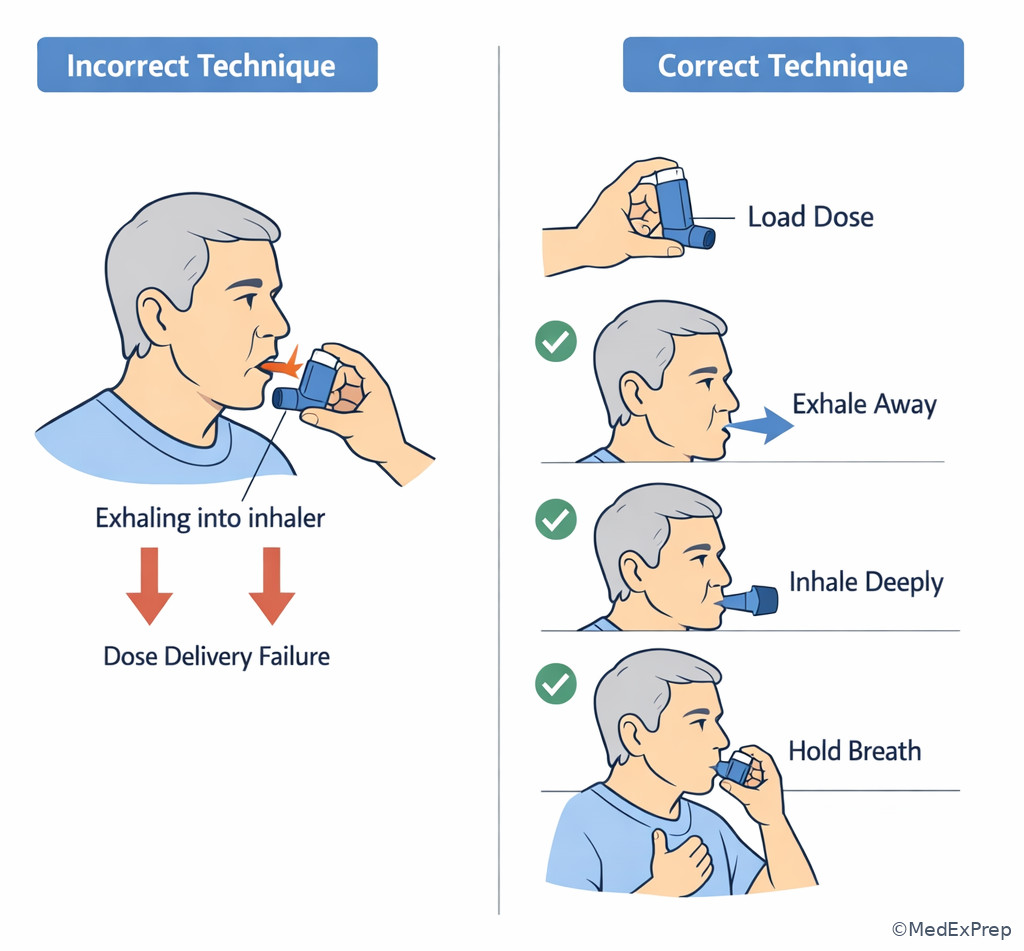
Examples: uncontrolled asthma on albuterol may look like undertreatment, but if the patient never uses the inhaler correctly, the core MRP is adherence/practical use. A PPI with poor symptom control may look ineffective, but if the patient is taking it after meals only intermittently, the problem is administration/adherence. A standard antibiotic dose may look fine, but if the patient has an immediate penicillin anaphylaxis history and cross-reactivity concern in the stem, safety becomes primary. In pharmacy practice, the best pharmacist action depends on the dominant driver, not every issue present.
Exam takeaway: One patient-specific fact can move the answer from simple optimization to hold, clarify, or counseling-focused intervention.
flowchart LR
A[Regimen looks straightforward] --> B{Key patient clue}
B -->|Poor technique or missed doses| C[Adherence or practical use]
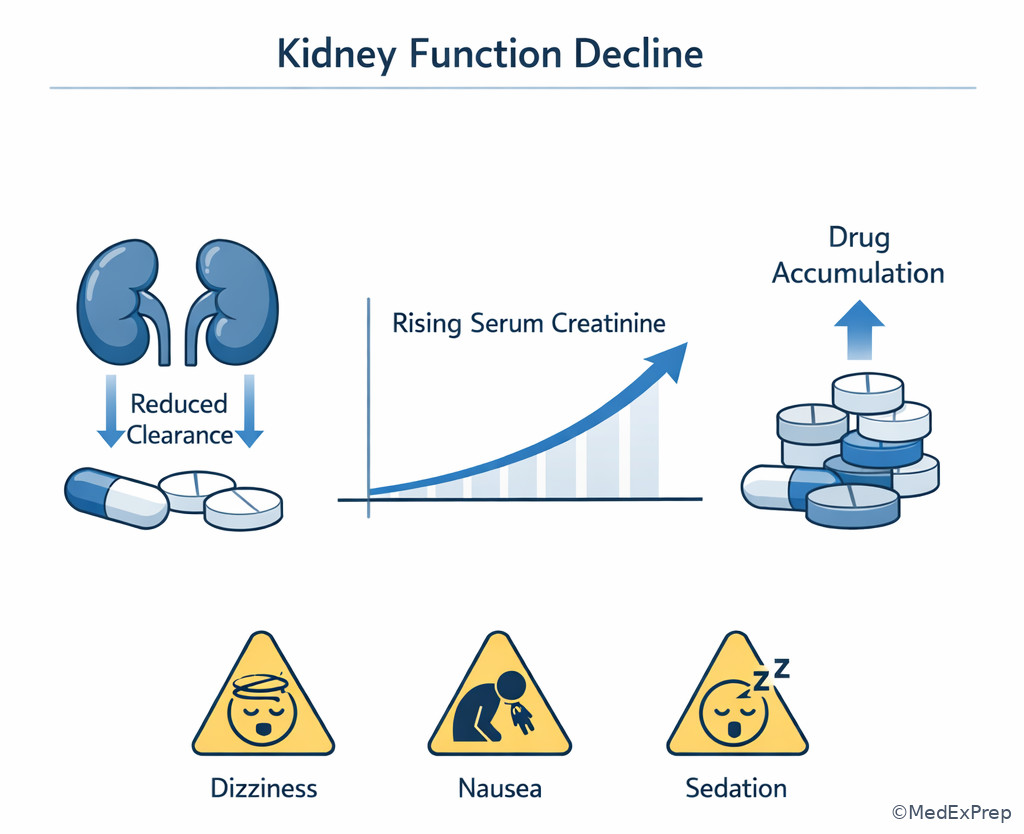
B -->|Kidney or liver decline| D[Safety: accumulation risk]
B -->|Duplicate agent from transition of care| E[Indication: unnecessary therapy]
B -->|No contraindication, but poor control| F[Effectiveness]
C --> G[Counsel or simplify]
D --> H[Hold, reduce, clarify]
E --> I[De-duplicate]
F --> J[Optimize or switch] When you feel two options are equally plausible, ask which single patient clue does the sorting. See Fig 4.
B Worked example
A 49-year-old man with asthma, obesity, and GERD requests an early refill for fluticasone/salmeterol 250/50 one inhalation twice daily and albuterol HFA two puffs every 4 hours as needed. He reports “the steroid inhaler never works,” has nighttime symptoms three times weekly, and also takes omeprazole 20 mg daily. His peak flow log is inconsistent. During counseling, he demonstrates activating the dry powder inhaler after exhaling directly into the device. The distracting clue is that he uses albuterol several times daily, which makes dose escalation look attractive.
Reasoning chain: Identify task: classify the most likely current MRP. Extract key facts: controller present, symptoms uncontrolled, technique error with dry powder inhaler, inconsistent peak flow log. Apply rule: if the regimen could work but the patient cannot use it correctly, the primary problem is adherence/practical use rather than pure ineffectiveness. Eliminate distractors: “dose too low” is tempting because symptoms persist; “untreated indication” is wrong because therapy exists. Verify: the best classification is adherence/practical-use problem due to device technique.
C Exam trap
D Checkpoint
Question: A 31-year-old woman with epilepsy, hypothyroidism, and iron deficiency takes levothyroxine 100 mcg by mouth every morning, ferrous sulfate 325 mg with breakfast, and calcium carbonate 500 mg three times daily. Her TSH remains elevated despite timely refills and she denies missed doses. Which medication-related problem best fits the levothyroxine issue?
- A. Untreated indication — Tempting because TSH is elevated, but incorrect because hypothyroidism is already being treated.
- B. Effectiveness problem — Correct because interacting administration with iron and calcium reduces absorption, making the regimen ineffective as used.
- C. Safety problem — Tempting because drug interactions are involved, but incorrect because the interaction here mainly causes subtherapeutic effect rather than toxicity.
- D. Unnecessary therapy — Tempting if one focuses on supplement duplication, but incorrect because the question asks specifically about levothyroxine not reaching goal.
1.1.1.6 Integration: convert the framework into the safest pharmacist action
A Explanation
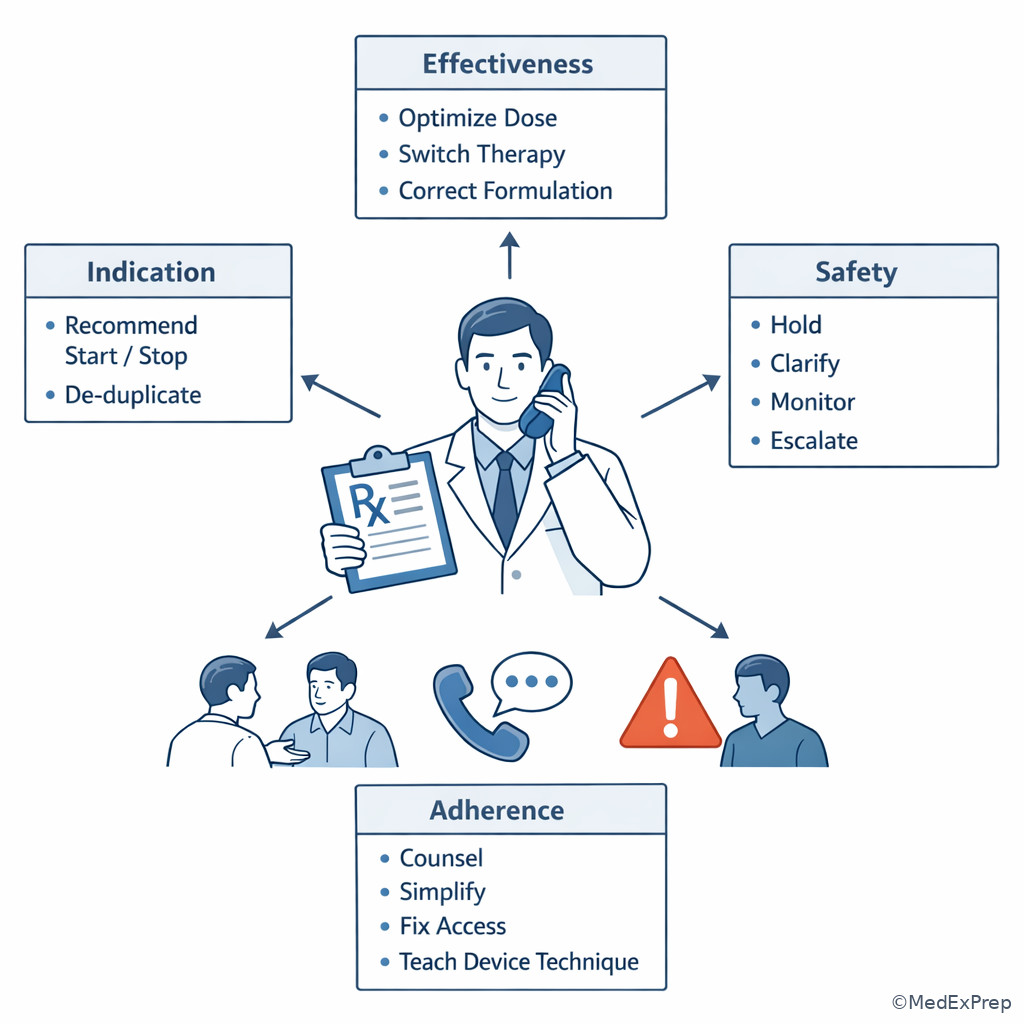
The final decision conflict is not just naming the category but choosing the right pharmacist move within scope. The rule is simple: the category predicts the action. Indication problems often lead to recommendation or clarification. Effectiveness problems usually lead to optimization, formulation correction, counseling, or monitoring recommendations. Safety problems most often lead to hold, urgent clarification, dose reduction recommendations, or escalation. Adherence/practical-use problems lead to counseling, simplification, refill coordination, affordability troubleshooting, or technique correction. WHY THIS IS TESTED: on NAPLEX, the best answer is often not the disease-management ideal but the safest pharmacist action supported by the data in the stem.
Choose hold and clarify when critical information is missing, the order is internally inconsistent, there is significant contraindication risk, or urgent harm is possible. Choose recommend when the problem is clear but implementation requires prescriber involvement. Choose counsel and verify understanding when the prescription is otherwise appropriate and the barrier is use-related. Reject out-of-role options such as independently diagnosing a new condition or unilaterally prescribing changes without authority. See Fig 5 for the action ladder.
Exam takeaway: The correct answer is usually the safest in-scope action predicted by the problem category.
B Worked example
A 72-year-old woman with osteoarthritis, hypertension, and CKD stage 3 presents with a new prescription for trimethoprim/sulfamethoxazole DS 1 tablet by mouth twice daily for 10 days while taking warfarin 5 mg nightly and lisinopril 20 mg daily. She has a documented sulfonamide antibiotic rash history listed as “hives,” but the prescriber note is not attached. Her INR last week was 2.4. The tempting but wrong clue is that the dose itself looks standard and the infection has already been diagnosed. The question asks for the best pharmacist action before dispensing.
Reasoning chain: Identify task: choose action, not diagnosis. Extract key facts: possible antibiotic allergy, major warfarin interaction, renal impairment, standard dose but high safety concern. Apply rule: safety problem with significant missing clarification and interaction risk predicts hold and contact prescriber. Eliminate distractors: counseling only is insufficient; changing therapy independently is out of role; dispensing with extra monitoring ignores the unresolved allergy and interaction concern. Verify: the safest action is hold dispensing and clarify with the prescriber.
C Exam trap
D Checkpoint
Question: A 66-year-old man with COPD, diabetes, and limited vision has correct refills on tiotropium inhalation daily and metformin 1000 mg twice daily. He says he “cannot tell which inhaler cap goes where,” and his wife reports frequent confusion about administration times. The prescription directions are accurate and no urgent contraindication is present. What is the best next pharmacist action category linkage?
- A. Safety → hold dispensing immediately — Tempting because misuse can cause harm, but incorrect because no urgent toxicity or contraindication is present; the dominant issue is practical use.
- B. Adherence/practical use → counsel and simplify the regimen — Correct because the primary problem is the patient’s ability to use the medications accurately.
- C. Indication → recommend adding another inhaler — Tempting because COPD symptoms may persist, but incorrect because the stem emphasizes confusion, not missing therapy.
- D. Effectiveness → increase tiotropium dose — Tempting because poor disease control may result, but incorrect because device confusion must be addressed first.
- If the best fix is to hold, avoid, or reduce therapy, the category is usually safety.
- True or False: Adherence barriers count as medication-related problems even when the order is correctly written. True.
- Name one trigger to stop routine verification and clarify: allergy conflict, dangerous interaction, missing key information, or major duplicate therapy.
Exam takeaway: Match each patient-specific clue on the profile to indication, effectiveness, safety, or adherence before verifying the order.
Exam takeaway: Two active drugs from the same therapeutic purpose should prompt duplication screening before routine refill.
Exam takeaway: A standard labeled dose can still become unsafe when renal function declines or interacting drugs are added.
Exam takeaway: When the regimen is appropriate but the patient cannot use the device correctly, classify the problem as practical-use or adherence related.
Exam Traps & Differentiators
- Most common wrong answer and why: Choosing “dose too low” whenever disease control is imperfect. This is tempting because exams often show one value above goal. Reject it when there is a more basic clue such as duplication, contraindication, technique failure, or nonadherence.
- Looks similar but isn’t: Uncontrolled disease due to missed doses is not the same as wrong drug or low dose. The regimen may be correct on paper but ineffective in real life because it is not being used properly.
- Related future trap: In the upcoming Best Next Pharmacist Action topic, some options will all describe helpful things to do. The winning answer will be the safest action for the dominant MRP category, not the most comprehensive list.
- Related future trap: In Order Verification Priorities, learners may focus on product selection before asking whether the therapy itself is indicated and safe. The framework in this lesson should come first.
| Looks similar | Actually this | Discriminating clue | Why it matters |
|---|---|---|---|
| Uncontrolled symptoms on therapy | Adherence/practical-use problem | Missed doses, refill gaps, wrong timing, bad device technique | Needs counseling or simplification before dose escalation |
| Persistent abnormal value | Safety problem | Toxicity signs, renal decline, interaction, allergy, excessive dose | Harm prevention outranks intensification |
| Multiple active drugs | Indication problem | Same purpose with no rationale or transition-of-care duplication | Requires de-duplication or clarification |
| Drug interaction present | Effectiveness problem | Interaction lowers exposure rather than causing toxicity | Optimize administration or spacing, not necessarily hold |
| Drug “not working” | Wrong formulation or route | Crushed ER product, incorrect inhaler, unsuitable dosage form | Framework points to effectiveness, not adherence alone |
If the stem says renal decline + sedation + same dose, think safety from accumulation.
If the stem says two active agents for the same purpose after hospitalization, think unnecessary/duplicate therapy.
If the stem says refills are timely but administration timing conflicts with food or supplements, think effectiveness problem caused by use pattern.
If the stem says patient demonstrates poor device technique, think adherence/practical-use barrier before dose escalation.
If the stem says allergy history is unresolved and a risky order arrives, think hold and clarify before dispensing.
Algorithm / Approach
Exam takeaway: Use a repeatable sequence so the safest pharmacist action follows directly from the dominant medication-related problem.
flowchart TD
A[Read medication context: drug dose route frequency] --> B[Define treatment purpose]
B --> C{Indication problem?}
C -->|Yes| D[Start stop or de-duplicate recommendation]
C -->|No| E{Effectiveness problem?}
E -->|Yes| F[Optimize or switch]
E -->|No| G{Safety problem?}
G -->|Yes| H[Hold clarify reduce or escalate]
G -->|No| I[Adherence or practical-use intervention]
H --> J[Document and communicate]
F --> J
D --> J
I --> J Keep this sequence visible during practice sets. See Fig 6.
Rapid Review
- Untreated indication → clear need with no appropriate therapy present
- Unnecessary therapy → active drug without current purpose or duplicated purpose
- Wrong drug → therapy present but poor fit for the patient or condition
- Dose too low → more therapy would solve the problem
- Safety problem → less therapy, holding, or avoidance would solve the problem
- Adherence issue → profile may be correct while real-world use is not
- Technique failure → classify as practical-use barrier before assuming drug failure
- Interaction lowering exposure → effectiveness problem more than toxicity problem
- Interaction increasing exposure → safety problem more than underdosing problem
- Duplicate inpatient-to-outpatient carryover → indication problem first
- Renal decline with toxicity symptoms → safety even if the labeled dose looks standard
- Abnormal value alone → not enough; find the clue that tells you why
- Best pharmacist action → must fit category and stay within scope
Self-check quiz
1. A 61-year-old woman with hypertension and GERD requests refills for omeprazole 20 mg by mouth daily and pantoprazole 40 mg by mouth daily, both active on her profile from different prescribers. She reports taking both every morning and denies missed doses. What is the most likely medication-related problem?
- A. Untreated indication
- B. Unnecessary therapy
- C. Dose too low
- D. Nonadherence
2. A 46-year-old man with asthma and allergic rhinitis uses fluticasone/salmeterol 250/50 one inhalation twice daily and albuterol HFA two puffs as needed. His refills are on time, but he demonstrates exhaling directly into the dry powder inhaler before inhalation. Which medication-related problem category best fits the controller inhaler issue?
- A. Untreated indication
- B. Effectiveness problem due to practical-use barrier
- C. Safety problem
- D. Unnecessary therapy
3. A 78-year-old man with CKD stage 4, diabetes, and peripheral neuropathy presents with a refill request for gabapentin 900 mg by mouth three times daily. He reports increasing sedation and falls, and his spouse confirms perfect adherence. Which is the best pharmacist classification of this issue?
- A. Effectiveness problem requiring dose increase
- B. Safety problem from dose accumulation
- C. Untreated indication
- D. Nonadherence causing poor control
4. A 33-year-old woman with hypothyroidism, iron deficiency, and migraines takes levothyroxine 100 mcg by mouth every morning, ferrous sulfate 325 mg with breakfast, and calcium carbonate 500 mg three times daily. Refills are timely, but her TSH remains elevated. What is the most appropriate classification for the levothyroxine problem?
- A. Effectiveness problem due to administration interaction
- B. Safety problem due to excessive dose
- C. Untreated indication
- D. Unnecessary therapy
5. A 70-year-old woman with atrial fibrillation, CKD stage 3, and a documented history of hives with sulfamethoxazole/trimethoprim presents a new prescription for sulfamethoxazole/trimethoprim DS 1 tablet by mouth twice daily for 7 days while taking warfarin 5 mg nightly. Which is the best next pharmacist action?
- A. Dispense as written and counsel on bleeding signs
- B. Reduce the antibiotic to once daily and dispense
- C. Hold dispensing and clarify with the prescriber
- D. Tell the patient to skip warfarin during therapy
6. A 64-year-old man with heart failure, atrial fibrillation, and CKD stage 3 takes digoxin 0.25 mg by mouth daily and amiodarone 200 mg daily. He now reports nausea, decreased appetite, and yellow visual halos; his serum creatinine has risen since the last refill. What is the most likely dominant medication-related problem?
- A. Effectiveness problem because heart failure is inadequately controlled
- B. Safety problem because the regimen now increases digoxin toxicity risk
- C. Untreated indication because the regimen lacks a beta blocker
- D. Nonadherence because symptoms suggest inconsistent intake
7. A 59-year-old woman with COPD, osteoarthritis, and cataracts has active prescriptions for tiotropium inhalation daily, albuterol HFA as needed, and prednisone 10 mg by mouth daily that was originally intended for a 5-day exacerbation course one month ago. She says she kept taking prednisone because “it helps me breathe.” Which medication-related problem is most important to identify first?
- A. Unnecessary therapy
- B. Dose too low for maintenance COPD control
- C. Untreated indication
- D. Safety problem only
8. A 68-year-old man with type 2 diabetes, neuropathy, and mild cognitive impairment takes metformin 1000 mg by mouth twice daily, insulin glargine 24 units nightly, and lisinopril 20 mg daily. His A1c is above goal. During counseling, he reveals he often skips insulin because he cannot remember whether he already injected, and his wife is hospitalized. What is the best primary medication-related problem classification driving the next pharmacist intervention?
- A. Untreated indication
- B. Effectiveness problem from dose too low
- C. Safety problem because glargine is inappropriate in older adults
- D. Adherence/practical-use problem
Answer key
1.1.1.7 1. Correct answer: B. Unnecessary therapy
A. Untreated indication — Tempting because GERD is a real condition requiring treatment. Incorrect for this specific scenario because therapy is already present twice over; the stem clue is two PPIs with the same purpose. This classification framework is supported by standard pharmacotherapy problem-solving models described in DiPiro and pharmacist care process teaching resources.
B. Unnecessary therapy — Correct because duplicate acid suppression without a distinct rationale signals medication without added current need. The discriminating clue is concurrent omeprazole and pantoprazole used every morning for the same condition. This matches medication-related problem frameworks in DiPiro and patient care process texts.
C. Dose too low — Tempting because some learners equate continued symptoms with undertreatment. Incorrect because the stem does not show refractory GERD despite optimized single-agent use; it shows duplication. The single eliminating fact is therapeutic overlap, not inadequate strength. DiPiro supports first resolving unnecessary therapy before dose optimization.
D. Nonadherence — Tempting because multiple prescribers often create confusion. Incorrect because she reports taking both drugs consistently, and the profile itself creates the problem. The discriminating clue is accurate adherence to an inappropriate duplicate regimen.
1.1.1.8 2. Correct answer: B. Effectiveness problem due to practical-use barrier
A. Untreated indication — Tempting because asthma remains symptomatic. Incorrect because controller therapy is already prescribed. The discriminating clue is improper device use, not absent therapy. Inhaler technique principles are emphasized in AHFS and major asthma guidance.
B. Effectiveness problem due to practical-use barrier — Correct because the drug is appropriate, but technique prevents adequate delivery. The single stem clue is exhaling into the dry powder inhaler, which disrupts powder delivery and medication exposure. This mechanism-based explanation aligns with inhaler counseling standards in AHFS and guideline-based asthma care.
C. Safety problem — Tempting because poor inhaler use can worsen asthma control. Incorrect because the present issue is failure of drug delivery rather than direct toxicity or contraindication. The discriminating fact is absence of harm-specific clues such as adverse effects or overdose.
D. Unnecessary therapy — Tempting if one assumes the controller is ineffective and should be stopped. Incorrect because the inhaler remains indicated; the problem is how it is used. The single clue is persistent need for controller therapy.
1.1.1.9 3. Correct answer: B. Safety problem from dose accumulation
A. Effectiveness problem requiring dose increase — Tempting because neuropathic pain often persists and gabapentin is frequently titrated. Incorrect here because CKD stage 4 plus sedation and falls signal excess exposure, not underdosing. The single stem clue is toxicity symptoms in severe renal impairment. Renal dosing guidance in Lexicomp and AHFS supports dose reduction rather than escalation.
B. Safety problem from dose accumulation — Correct because gabapentin is renally eliminated, and reduced kidney function increases risk of sedation and neurotoxicity at standard higher doses. The discriminating clue is CKD stage 4 with falls and sedation despite adherence. Lexicomp renal dosing recommendations support this interpretation.
C. Untreated indication — Tempting because pain remains a clinical problem. Incorrect because the patient is already treated for neuropathy. The single eliminating clue is an active gabapentin regimen.
D. Nonadherence causing poor control — Tempting because poor pain control can result from irregular use. Incorrect because the spouse confirms adherence and the adverse effects strongly suggest accumulation. The discriminating clue is perfect adherence plus toxicity.
1.1.1.10 4. Correct answer: A. Effectiveness problem due to administration interaction
A. Effectiveness problem due to administration interaction — Correct because iron and calcium reduce levothyroxine absorption, leading to persistent hypothyroid labs despite appropriate refill history. The single discriminating clue is levothyroxine taken near interacting cations. This is supported by FDA labeling, Lexicomp, and AHFS counseling guidance.
B. Safety problem due to excessive dose — Tempting because thyroid replacement questions often test over- or undertreatment. Incorrect here because the problem is poor absorption with elevated TSH, not excess thyroid effect. The eliminating clue is concomitant iron and calcium rather than hyperthyroid symptoms.
C. Untreated indication — Tempting because TSH remains elevated. Incorrect because hypothyroidism is being treated. The discriminating clue is an active levothyroxine prescription.
D. Unnecessary therapy — Tempting if one focuses on supplement burden. Incorrect because the question asks about why levothyroxine is not working, and the best category is impaired effectiveness. The single clue is persistent elevated TSH despite adherence.
1.1.1.11 5. Correct answer: C. Hold dispensing and clarify with the prescriber
A. Dispense as written and counsel on bleeding signs — Tempting because warfarin interactions can sometimes be managed with INR monitoring and counseling. Incorrect because the stem adds a documented history of hives to the same antibiotic, making unresolved allergy risk the discriminating clue. FDA labeling and Lexicomp support avoiding or clarifying true antibiotic allergy concerns before dispensing.
B. Reduce the antibiotic to once daily and dispense — Tempting because CKD often triggers renal dose adjustments. Incorrect because dose adjustment does not resolve the allergy concern or the major interaction issue. The single clue that eliminates this option is documented hives with the same medication.
C. Hold dispensing and clarify with the prescriber — Correct because the pharmacist is facing a likely safety problem with both allergy and interaction risk, and independent substitution is out of role unless authority is provided. The discriminating clue is that routine dispensing would ignore a potentially unsafe order. This action is consistent with pharmacist-scope medication safety responsibilities and standard references such as Lexicomp, AHFS, and FDA labeling.
D. Tell the patient to skip warfarin during therapy — Tempting because it appears to manage the interaction. Incorrect because instructing unapproved anticoagulation interruption is not the safest in-scope response and still ignores allergy concerns. The single eliminating clue is that prescriber clarification is needed before any dispensing or self-directed regimen change.
1.1.1.12 6. Correct answer: B. Safety problem because the regimen now increases digoxin toxicity risk
A. Effectiveness problem because heart failure is inadequately controlled — Tempting because heart failure patients often have ongoing symptoms and medication optimization needs. Incorrect here because nausea, anorexia, visual halos, renal decline, and amiodarone coadministration are classic safety clues. The single discriminator is the toxicity pattern, not a lack of therapeutic options. Digoxin monitoring guidance in Lexicomp and AHFS supports immediate safety concern.
B. Safety problem because the regimen now increases digoxin toxicity risk — Correct because digoxin has a narrow therapeutic index, is affected by renal function, and exposure may rise with interacting drugs such as amiodarone. The stem clue is yellow visual halos with worsening renal function. Lexicomp, AHFS, and FDA labeling confirm toxicity risk and need for caution.
C. Untreated indication because the regimen lacks a beta blocker — Tempting because guideline-directed heart failure therapy often includes multiple foundational agents. Incorrect because the question asks for the dominant current medication-related problem, and acute toxicity outranks absent long-term optimization. The single eliminating clue is active toxicity symptoms.
D. Nonadherence because symptoms suggest inconsistent intake — Tempting because nausea can lead to erratic medication use. Incorrect because the symptom cluster and renal change specifically fit toxicity rather than nonadherence. The single clue is amiodarone plus declining renal function.
1.1.1.13 7. Correct answer: A. Unnecessary therapy
A. Unnecessary therapy — Correct because prednisone was intended for a short exacerbation course but has been continued beyond the original treatment need. The discriminating clue is that the active medication persists after its temporary indication ended. DiPiro and standard COPD pharmacotherapy references support limiting systemic corticosteroid bursts rather than chronic unsupervised continuation.
B. Dose too low for maintenance COPD control — Tempting because persistent breathing symptoms can suggest undertreatment. Incorrect because the dominant issue is continued systemic steroid use without current intended indication, not insufficient prednisone. The single clue is the original 5-day burst instruction.
C. Untreated indication — Tempting because COPD may still need better long-term control. Incorrect because the patient already has maintenance inhaled therapy. The single eliminating clue is active tiotropium and albuterol therapy already on the profile.
D. Safety problem only — Tempting because chronic prednisone clearly carries safety risks. Incorrect as the best primary classification because the first issue is that the drug is no longer needed as originally prescribed; the safety risk stems from that unnecessary continuation. The discriminating clue is expired intended duration. Medication-related problem frameworks place unnecessary therapy under indication first.
1.1.1.14 8. Correct answer: D. Adherence/practical-use problem
A. Untreated indication — Tempting because the A1c remains above goal and many patients eventually need more therapy. Incorrect because diabetes treatment is already present. The single eliminating clue is active metformin plus basal insulin.
B. Effectiveness problem from dose too low — Tempting because uncontrolled A1c can reflect inadequate basal insulin. Incorrect because the stem directly identifies skipped injections due to memory uncertainty; the regimen cannot be judged ineffective until use is corrected. The discriminating clue is missed insulin because he cannot remember prior doses. ADA standards and insulin counseling resources emphasize adherence and administration assessment before intensification.
C. Safety problem because glargine is inappropriate in older adults — Tempting because cognitive impairment increases hypoglycemia risk. Incorrect because glargine is not inherently inappropriate; the immediate issue is inability to administer consistently. The single clue is skipped rather than excessive injections.
D. Adherence/practical-use problem — Correct because the main barrier is medication use in the setting of cognitive limitation and loss of caregiver support. The best next intervention would center on counseling, simplification, or support systems rather than automatic dose escalation. This is consistent with pharmacist patient care process principles in DiPiro and ADA guidance.