Stable Angina Patterns
What you’ll learn
- Recognize the illness script for stable angina and separate it from acute coronary syndrome and nonischemic chest pain.
- Choose the most appropriate initial outpatient workup for suspected chronic coronary syndrome.
- Select first-line symptom control and secondary prevention strategies for stable angina.
- Identify red flags that convert a “stable” chest pain history into urgent escalation.
- Use exercise tolerance, timing, triggers, and relief pattern to eliminate close distractors on exam stems.
Blueprint mapping
- Cardiovascular: Diagnosis -> Chest pain pattern recognition
- Cardiovascular: Interpretation -> Ischemic symptom probability
- Cardiovascular: Management -> Initial antianginal therapy and risk reduction
- Cardiovascular: Disposition -> Stable outpatient workup vs urgent escalation
- Preventive Care: Management -> ASCVD risk reduction in known CAD
Why it matters
- Stable angina is common, highly testable, and often appears in stems designed to tempt you into overcalling MI or undercalling ischemia.
- The exam frequently separates predictable exertional symptoms relieved by rest from new, worsening, or rest pain that needs ACS-level urgency.
- Correct answers often hinge on choosing the right next test for a stable patient rather than jumping directly to invasive care.
- Management questions blend symptom relief with prevention: antianginal therapy, aspirin when appropriate, statin therapy, and risk-factor control.
Exam takeaway: Predictable exertional pain relieved by rest points toward stable angina, while rest pain or progression should trigger ACS thinking.
flowchart TD
A[Chest pain history] --> B{Predictable with exertion?}
B -->|Yes| C{Relieved in minutes by rest or nitroglycerin?}
C -->|Yes| D[Stable angina pattern likely]
C -->|No| E[Reassess for other causes or unstable ischemia]
B -->|No| F{Occurs at rest, new, or worsening?}
F -->|Yes| G[Think ACS and escalate]
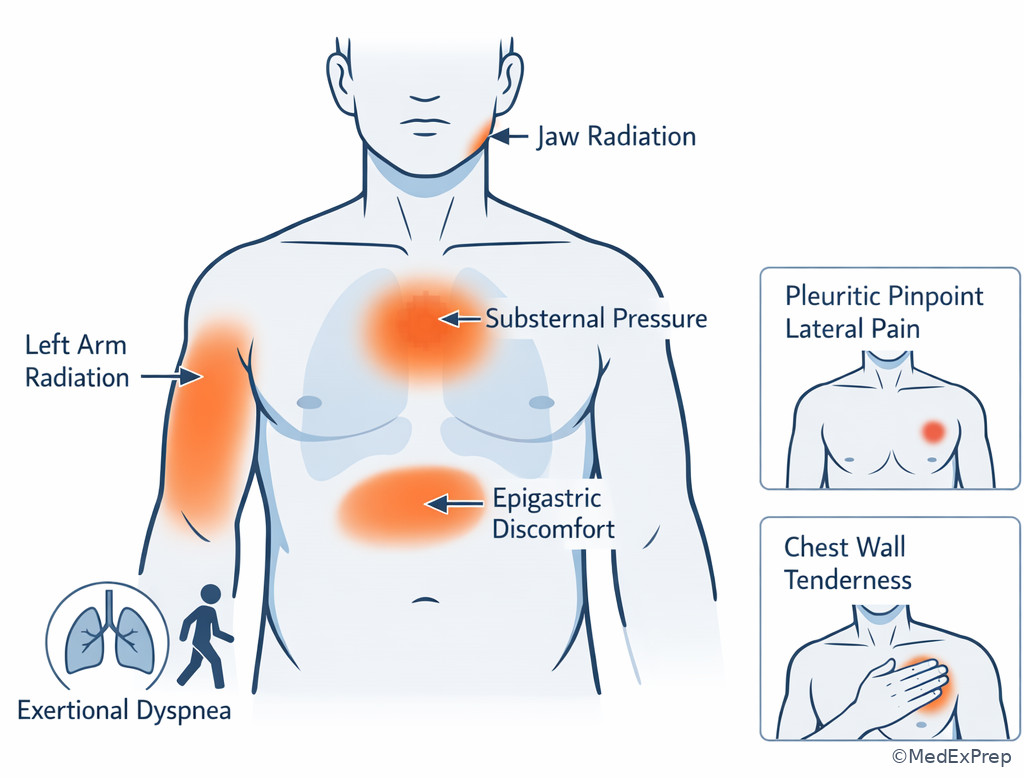
F -->|No| H[Consider noncardiac or atypical causes] When you see a board-style stem with “walking uphill,” “climbing stairs,” or “after meals in cold weather” followed by symptom relief within minutes of rest, think chronic myocardial oxygen supply-demand mismatch rather than plaque rupture. See Fig 1.
Key Terms & Must-Know Facts
1.1.1.1 Key terms
- Stable angina: Predictable chest discomfort with exertion or emotional stress, relieved by rest or nitroglycerin.
- Chronic coronary syndrome: Broad modern term for stable ischemic heart disease patterns.
- Demand ischemia: Myocardial oxygen demand exceeds supply without acute plaque rupture.
- Typical angina: Substernal discomfort, provoked by exertion/emotion, relieved by rest or nitroglycerin.
- Atypical angina: Meets 2 of the 3 classic angina features.
- Nonanginal chest pain: Meets 0-1 classic features.
- Functional capacity: Exercise tolerance that helps determine testing choice.
- Pretest probability: Estimated chance of obstructive CAD before testing.
- Antianginal therapy: Medications used to reduce ischemic symptoms, such as beta blockers, calcium channel blockers, or nitrates.
- Sublingual nitroglycerin: Short-acting nitrate for acute symptom relief.
- Secondary prevention: Measures that reduce future ASCVD events in known or suspected CAD.
- Exercise stress testing: Provocative testing for inducible ischemia when the patient can exercise and ECG is interpretable.
- Unstable angina: Ischemic symptoms at rest, new severe symptoms, or crescendo symptoms without troponin elevation.
1.1.1.2 Must-know facts
- Stable angina is predictable; ACS is unpredictable or progressive.
- Symptoms usually last minutes, not seconds, and are often triggered by exertion.
- Relief with nitroglycerin is helpful but not perfectly specific for CAD.
- A normal resting ECG does not exclude stable angina.
- Initial testing depends on ability to exercise and baseline ECG interpretability.
- Beta blockers are a common first-line antianginal choice unless contraindicated.
- Short-acting nitrates are used for symptom episodes and pre-exertional prophylaxis.
- High-intensity statin therapy is central when CAD is established or strongly suspected.
- Pain at rest, increasing frequency, or prolonged episodes should push you toward ACS evaluation.
| Feature | Stable angina clue | Why it matters on exam |
|---|---|---|
| Trigger | Exertion, emotional stress, cold exposure, heavy meals | Supports demand-related ischemia |
| Pattern over time | Same threshold, same quality, reproducible | Separates from crescendo symptoms |
| Relief | Rest or nitroglycerin within minutes | Classic stable ischemic script |
| Duration | Usually brief, often under 10-15 minutes | Very prolonged pain raises concern for ACS |
| Rest pain | Absent | If present, do not call it stable |
| Baseline ECG | May be normal | Do not be falsely reassured |
| Biomarkers | Not elevated in routine stable disease | Troponin testing is for acute concern, not every chronic exertional symptom |
Core content
1.1.1.3 Foundational pattern recognition: when exertional chest pain fits stable angina
A Explanation
The core decision conflict is whether the patient has a predictable fixed-obstruction pattern or a dynamic acute ischemic process. Choose stable angina when the story is reproducible: the same amount of walking, the same hill, or the same emotional stress reliably causes pressure-like chest discomfort that stops with rest after a few minutes. Reject stable angina when the pain is new at rest, more severe than usual, or happening with much less exertion than before.
WHY THIS IS TESTED: exam writers know many learners anchor too heavily on the word “chest pain” and forget that timing plus provocation plus relief is the single most useful first-pass rule.
Classic angina has 3 features: substernal discomfort, provoked by exertion or emotional stress, relieved by rest or nitroglycerin. Three of three supports typical angina; two of three is atypical angina; zero to one favors nonanginal pain. This classification does not replace judgment, but it sharply changes pretest probability and testing strategy. Stable angina comes from flow-limiting atherosclerotic plaque that cannot meet increased oxygen demand during exertion. There is ischemia, but not the acute plaque rupture-thrombus process seen in ACS.
Exam takeaway: The reproducible threshold and prompt relief pattern are the fastest way to identify stable angina in vignette stems.
See Fig 2. Also remember the forward link: if the story shifts to prolonged pain at rest or rising frequency, the next topic is ACS, not “worse stable angina.”
B Worked example
A 62-year-old man presents for 3 months of chest “tightness” when he walks two blocks uphill. He has type 2 diabetes, hypertension, and hyperlipidemia. He says the discomfort sometimes radiates to the left arm and lasts about 5 minutes, resolving when he sits down. He also mentions reproducible chest wall tenderness after moving furniture last week. Vitals are normal; resting ECG shows no acute changes; LDL is 148 mg/dL. The task is to identify the most likely chest pain pattern.
Reasoning chain: Identify task: classify the pain. Extract key facts: exertional trigger, same threshold, short duration, relief with rest, multiple CAD risk factors. Apply rule: that is a stable angina script. Eliminate distractors: musculoskeletal pain is tempting because of chest wall tenderness, but that finding is noise because the exertional arm-radiating pressure is the dominant pattern. ACS is less likely because symptoms are not new at rest and are unchanged over months. Verify safety: he still needs formal evaluation and preventive therapy, not simple reassurance.
C Exam trap
D Checkpoint
Question: A 58-year-old woman with hypertension and smoking history reports substernal pressure when climbing two flights of stairs. It resolves within 4 minutes of rest and has been unchanged for 4 months. Which diagnosis is most likely?
- Stable angina — Tempting because the exertional, reproducible pattern fits classic ischemia; this is correct because predictable activity-related pain relieved by rest defines stable angina.
- Unstable angina — Tempting because coronary ischemia is present; wrong because there is no rest pain, new severity, or crescendo pattern.
- Acute pericarditis — Tempting because chest pain can occur in middle-aged adults; wrong because pericarditis is pleuritic and positional rather than exertional and reproducible.
- Aortic dissection — Tempting because chest pain plus hypertension can raise concern; wrong because dissection causes sudden severe tearing pain, not months of brief exertional episodes.
1.1.1.4 Foundational testing logic: choosing the right initial evaluation
A Explanation
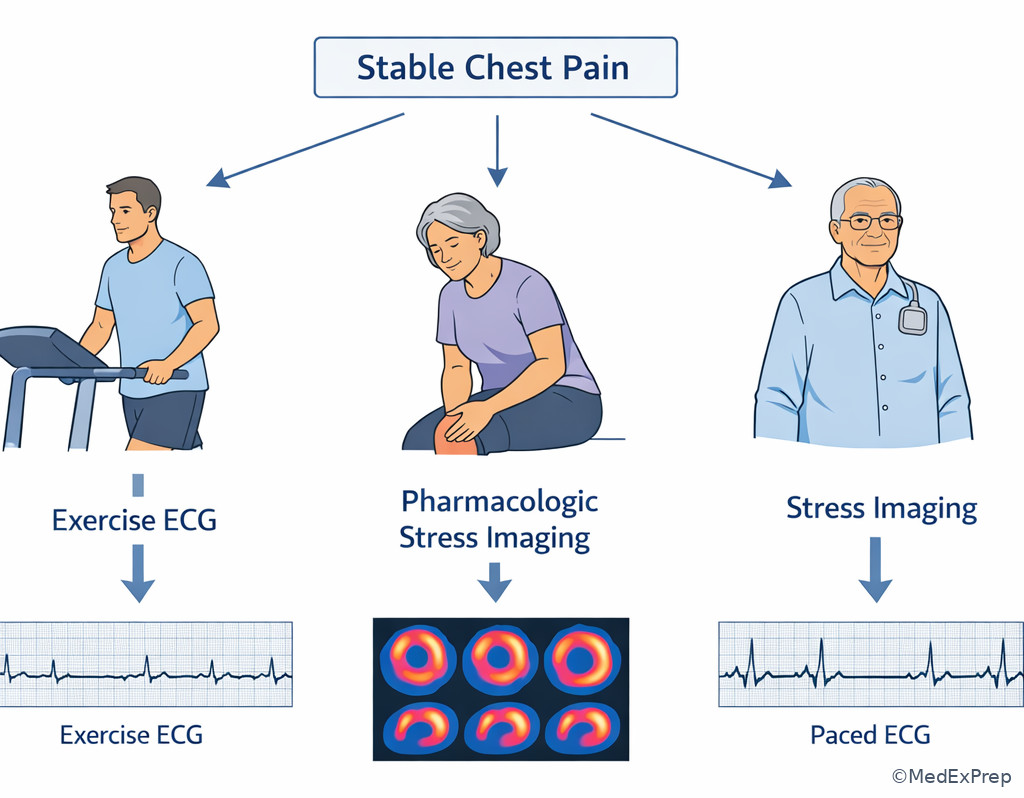
The decision conflict here is not “test or no test” but which stable-patient test matches the clinical setting. Choose a noninvasive ischemia evaluation when the patient is stable and symptoms are compatible with CAD. The single rule that resolves many exam questions is: if the patient can exercise and the resting ECG is interpretable, an exercise ECG stress test is often the best initial test. Reject plain exercise ECG when baseline ECG abnormalities limit interpretation; then choose an imaging-based stress test or coronary CT angiography depending on the stem.
WHY THIS IS TESTED: learners often memorize “stress test” without learning the branching logic based on exercise capacity and ECG interpretability.
Start with history, exam, risk profile, and resting ECG. A normal ECG does not exclude stable angina. If the patient is currently having concerning active symptoms or has unstable features, the question is no longer stable outpatient workup. For stable chest pain, the exam often rewards the simplest correct next step rather than the most technologically advanced test. Exercise ECG is useful when the patient can reach adequate workload and there is no left bundle branch block, paced rhythm, marked ST baseline abnormality, or other factor making ST changes hard to read. If the patient cannot exercise because of arthritis, severe COPD, stroke deficits, or deconditioning, choose pharmacologic stress imaging. If the stem emphasizes anatomic clarification in a lower-intermediate risk stable patient, coronary CT angiography may appear as an option.
Exam takeaway: Start with exercise ability and ECG interpretability before choosing a stress modality.
Exam takeaway: Exercise ECG is best only when the patient can exercise and the baseline ECG can be interpreted.
flowchart TD
A[Suspected stable angina] --> B{Unstable features?}
B -->|Yes| C[ACS pathway and urgent evaluation]
B -->|No| D{Can exercise?}
D -->|Yes| E{Baseline ECG interpretable?}
E -->|Yes| F[Exercise ECG stress test]
E -->|No| G[Exercise stress imaging]
D -->|No| H[Pharmacologic stress imaging]
H --> I[Risk-guided treatment]
F --> I
G --> I See Fig 3. The exam is usually asking for the most appropriate next step, not the most definitive test in all circumstances.
B Worked example
A 67-year-old woman with diabetes, obesity, osteoarthritis of both knees, and chronic stable exertional chest pressure is seen in clinic. Symptoms occur after walking across a parking lot and resolve in 3-4 minutes with rest. She has a paced rhythm on ECG from prior sick sinus syndrome. Troponin is not indicated because she is asymptomatic in clinic and has no acute change. The question asks for the most appropriate next diagnostic test.
Reasoning chain: Identify task: choose a stable ischemia test. Extract key facts: cannot exercise well because of knee disease; paced ECG is not interpretable for simple ST-segment treadmill testing. Apply rule: plain exercise ECG should be rejected. Eliminate distractors: exercise treadmill testing is tempting because it is common and inexpensive, but the ECG cannot be read for ischemia and she cannot exercise adequately. Verify: pharmacologic stress imaging is the best next step in a stable outpatient setting.
C Exam trap
D Checkpoint
Question: A 60-year-old man with exertional substernal pressure can jog on a treadmill and has a normal baseline ECG without conduction abnormalities. He is currently pain-free and stable. What is the most appropriate initial diagnostic test?
- Exercise ECG stress test — Tempting and correct because he can exercise and the baseline ECG is interpretable, making this the simplest appropriate first test.
- Immediate coronary angiography — Tempting because it directly visualizes anatomy; wrong because a stable outpatient without high-risk instability usually begins with noninvasive evaluation.
- Troponin trend every 3 hours — Tempting because ischemic chest pain raises ACS concern; wrong because there is no acute evolving syndrome in this stable clinic presentation.
- D-dimer testing — Tempting because chest symptoms can trigger broad workups; wrong because the story specifically fits exertional myocardial ischemia, not pulmonary embolism risk stratification.
- The best first stress modality when a stable patient can exercise and the ECG is readable is exercise ECG.
- True or False: A normal resting ECG excludes stable angina. False.
- Name the 2 branch points before picking a stress test: exercise capacity and ECG interpretability.
1.1.1.5 Applied symptom interpretation: typical vs atypical vs nonanginal chest pain
A Explanation
The decision conflict is whether the symptom description is cardiac enough to pursue ischemia-focused evaluation or whether another diagnosis is more likely. Choose an anginal category by using the 3-feature framework rather than guessing from vague descriptors. The single rule: count the classic features. Substernal pressure-like discomfort, brought on by exertion or emotional stress, and relieved by rest or nitroglycerin equals typical angina if all 3 are present. Two features suggest atypical angina. Zero to one supports nonanginal pain.
WHY THIS IS TESTED: many stems hide the diagnosis inside language like “indigestion,” “tightness,” “heaviness,” or “burning.” The exam wants you to translate patient wording into ischemic probability.
Older adults, women, and patients with diabetes may present less classically, with exertional dyspnea, fatigue, epigastric pressure, or decreased exercise tolerance rather than textbook crushing pain. That does not make the symptoms noncardiac. On the other hand, pain lasting a few seconds, pain that is purely pleuritic, pain that is sharply localized with one finger, or pain unrelated to exertion is less supportive of stable angina. Still, no single descriptor ends the evaluation; the full pattern matters.
Exam takeaway: Count the 3 classic features before deciding whether chest pain is typical, atypical, or nonanginal.
Exam takeaway: Use symptom location, radiation, and exertional context together rather than relying on one descriptor alone.
B Worked example
A 55-year-old woman with diabetes and CKD stage 3 reports “indigestion” and shortness of breath whenever she carries groceries from the car. She denies sharp pain. The sensation is central, lasts 6 minutes, and improves after sitting. She also has chronic GERD and notes occasional sour taste after large meals. The task is to decide whether this is more likely anginal or gastrointestinal.
Reasoning chain: Identify task: classify symptoms. Extract key facts: exertional, central discomfort, dyspnea equivalent, short-lived, relieved by rest, multiple CAD risks. Apply rule: despite the word “indigestion,” she effectively meets the anginal framework. Eliminate distractors: GERD is tempting because of reflux history and epigastric language, but GERD is not reliably triggered by carrying groceries and relieved within minutes by rest. Verify: ischemic evaluation is appropriate.
C Exam trap
D Checkpoint
Question: Which history most strongly supports typical stable angina?
- Sharp left-sided pain lasting 10 seconds, worse with deep breathing — Tempting because chest pain can still worry exam takers; wrong because pleuritic, brief pain does not fit the classic 3-feature angina model.
- Burning epigastric discomfort after spicy meals, worse lying down — Tempting because ischemia can be described as burning; wrong because meal- and position-related symptoms point away from exertional ischemia.
- Substernal pressure while climbing stairs, relieved after resting for 3 minutes — Tempting and correct because it directly matches substernal, exertional, rest-relieved angina.
- Localized tenderness over the costochondral junction after lifting boxes — Tempting because activity precedes pain; wrong because musculoskeletal chest wall pain is positional or reproducible to palpation, not demand ischemia.
1.1.1.6 Integration of treatment: symptom control plus secondary prevention
A Explanation
The decision conflict is whether treatment should only reduce symptoms or also reduce future events. The correct exam answer often includes both. Choose beta blockers as common first-line antianginal therapy, especially when there is a need to reduce heart rate and myocardial oxygen demand. Choose sublingual nitroglycerin for immediate symptom relief or before exertion. Add aspirin and high-intensity statin therapy when CAD is established or strongly suspected unless contraindications exist. Reject therapies that sound cardiac but do not address the right goal in the scenario.
WHY THIS IS TESTED: many students treat stable angina as if symptom relief alone were enough. Board questions often reward the answer that adds risk reduction.
Beta blockers lower heart rate and contractility, thereby decreasing oxygen demand. Calcium channel blockers are options when beta blockers are contraindicated or inadequate; nondihydropyridines also slow heart rate, while dihydropyridines mainly vasodilate. Long-acting nitrates help symptom prevention but require nitrate-free intervals to avoid tolerance. Ranolazine may appear as add-on therapy in persistent symptoms, but it is not usually the first answer in foundational stems. Beyond antianginals, smoking cessation, blood pressure control, diabetes management, and exercise counseling are all testable. Revascularization may be considered for refractory symptoms or high-risk anatomy, but exam stems at this level usually emphasize medical therapy first in stable disease.
Exam takeaway: The best answer often combines short-term symptom relief with long-term event reduction.
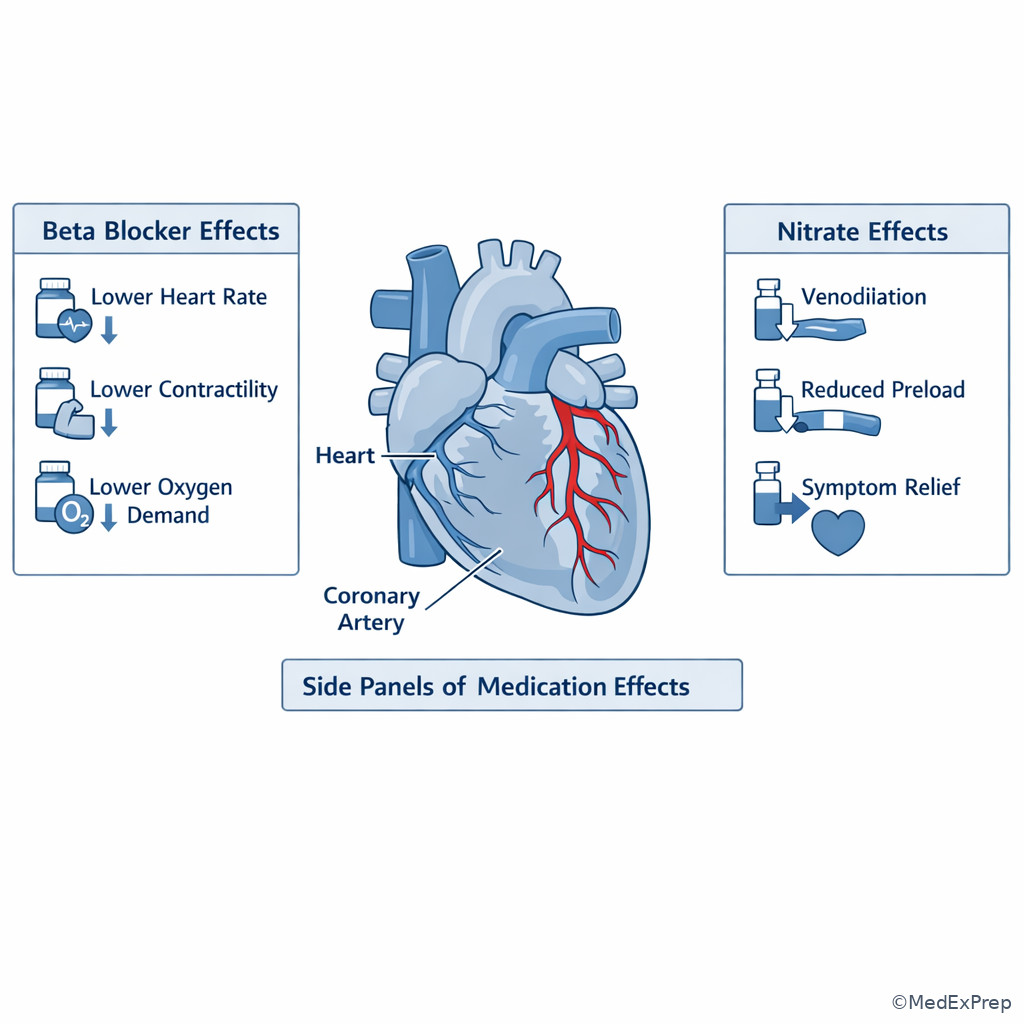
See Fig 4. On a “best initial therapy” question, ask whether the exam is testing immediate relief, chronic control, or risk reduction.
Exam takeaway: Link beta blockers to lower demand and nitrates to rapid venodilation-based symptom relief.
B Worked example
A 64-year-old man with prior smoking, hypertension, and known CAD reports chest pressure when shoveling snow. Symptoms stop within minutes of rest. He takes no current antianginal medication. He also has benign prostatic hyperplasia and asks whether a friend’s erectile dysfunction medication would interact with heart pills. BP is 148/88 mm Hg, HR 84/min, LDL 132 mg/dL. The task is to choose appropriate initial management.
Reasoning chain: Identify task: chronic stable management. Extract key facts: predictable exertional angina, hemodynamically stable, untreated risk factors. Apply rule: give short-acting nitroglycerin for episodes, start beta blocker if no contraindication, and intensify secondary prevention with statin therapy. Eliminate distractors: immediate catheterization is tempting because he has known CAD, but symptoms are stable and the stem asks initial management. Verify safety: counsel him not to combine nitrates with PDE-5 inhibitors.
C Exam trap
D Checkpoint
Question: A stable outpatient with known exertional angina has recurrent symptoms while climbing stairs. Which option best addresses both symptom control and future cardiovascular risk?
- Sublingual nitroglycerin only — Tempting because it quickly relieves chest discomfort; wrong because it does not provide chronic demand reduction or event prevention by itself.
- Beta blocker plus sublingual nitroglycerin and high-intensity statin therapy — Tempting and correct because it combines chronic antianginal control, rescue therapy, and secondary prevention.
- Opioid analgesic as needed — Tempting because it addresses pain; wrong because it does not treat ischemia or risk reduction and is not standard outpatient angina therapy.
- Empiric proton pump inhibitor alone — Tempting because chest discomfort may mimic reflux; wrong because the exertional reproducible pattern points to ischemia, not primary acid-related disease.
- The common first-line chronic antianginal class is beta blockers.
- True or False: Short-acting nitroglycerin replaces the need for statin-based prevention. False.
- Name 3 stable angina management goals: relieve episodes, reduce demand, prevent future ASCVD events.
1.1.1.7 Integration and safety: distinguishing stable angina from urgent chest pain mimics and progression
A Explanation
The final decision conflict is safety: when should you stop the outpatient stable-angina pathway and pivot to urgent evaluation? The single rule is this: stable angina should not occur at rest, should not be rapidly worsening, and should not be prolonged or hemodynamically unstable. If any of those are present, reject the stable label until proven otherwise.
WHY THIS IS TESTED: many exam questions are really triage questions hidden inside a diagnosis stem.
Unstable angina or NSTEMI can resemble stable angina but differ by timing and evolution. Pericarditis usually causes pleuritic pain that improves when leaning forward and may show diffuse ST elevation with PR depression. Aortic dissection causes abrupt, severe, tearing pain with pulse or blood pressure asymmetry. Pulmonary embolism often adds dyspnea, pleuritic pain, tachycardia, or risk factors for venous thromboembolism. Musculoskeletal pain may be reproducible with palpation; GERD often links to meals or recumbency. The exam frequently places one clue from these mimics into an otherwise angina-looking stem. Your job is to identify the clue that overrules the rest of the story.
Exam takeaway: Rest pain, progression, prolonged episodes, or instability should move you off the stable outpatient pathway.
Exam takeaway: The safest answer changes once pain becomes rest-related, progressive, or accompanied by high-risk features.
flowchart TD
A[Chest pain compatible with ischemia] --> B{Predictable only with exertion?}
B -->|Yes| C{Unchanged for weeks to months?}
C -->|Yes| D[Stable angina pathway]
C -->|No| E[Escalate for possible ACS]
B -->|No| F{Rest pain or prolonged episode?}
F -->|Yes| E
F -->|No| G{Pleuritic or positional?}
G -->|Yes| H[Consider pericarditis or PE]
G -->|No| I{Tearing pain or pulse asymmetry?}
I -->|Yes| J[Consider aortic dissection]
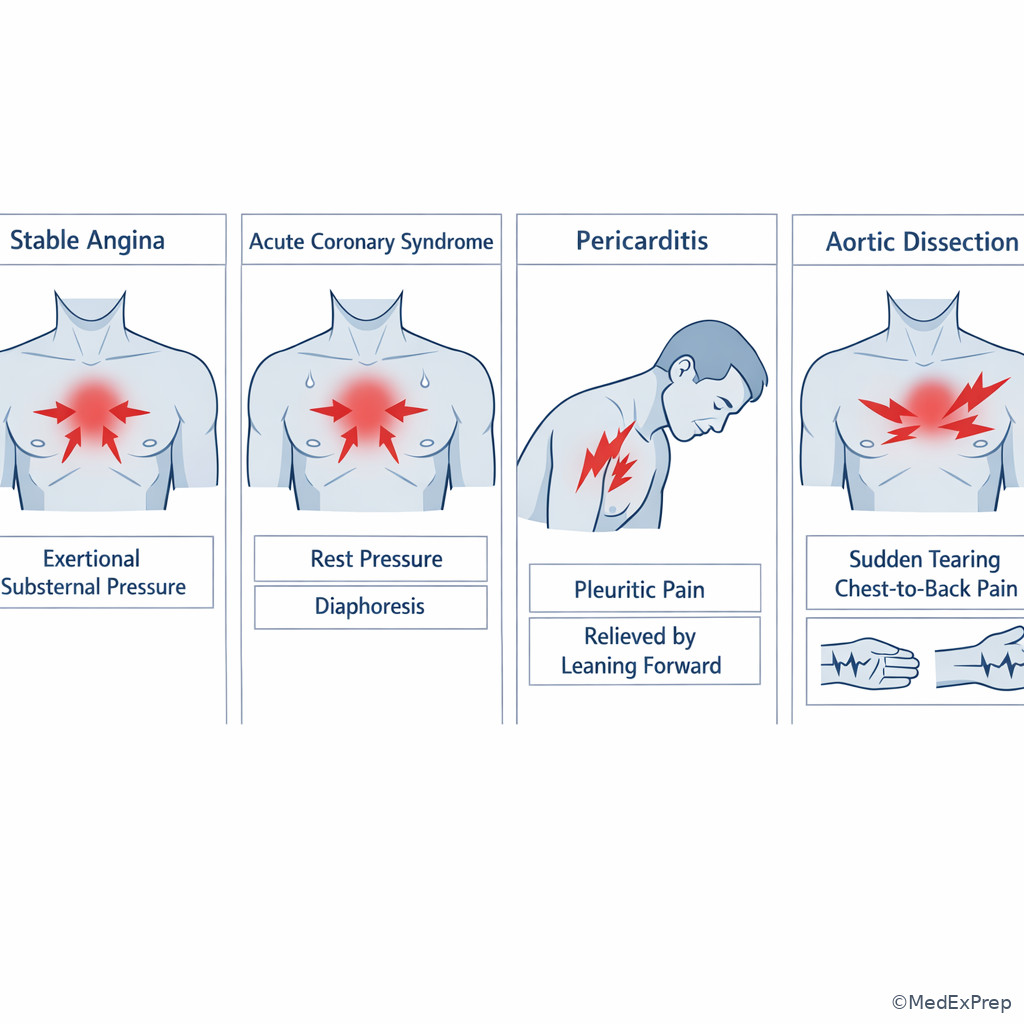
I -->|No| K[Reassess differential] See Fig 5. This topic also sets up the next two lessons: ACS is the progression pathway; pericarditis and aortic emergencies are the chest pain look-alikes with different discriminators.
Exam takeaway: One discriminating visual clue can separate stable angina from pericarditis, dissection, or pulmonary embolism.
B Worked example
A 70-year-old woman with diabetes, prior smoking, and peripheral arterial disease reports a month of exertional chest pressure when walking uphill. Over the last 2 days, she has had two episodes while watching television, each lasting 20 minutes, with diaphoresis. She also notes mild reproducible trapezius tenderness after gardening. The question asks for the most appropriate next step.
Reasoning chain: Identify task: determine disposition, not just diagnosis. Extract key facts: prior exertional pattern has changed, now occurring at rest and lasting longer, with autonomic symptoms. Apply rule: this is no longer stable angina. Eliminate distractors: outpatient stress testing is tempting because of the long prior history of exertional pain, and the muscle tenderness is distracting noise. Verify: urgent ACS evaluation is required.
C Exam trap
D Checkpoint
Question: Which stem detail most strongly requires abandoning the stable angina pathway?
- Symptoms reliably occur after climbing stairs and stop after 3 minutes of rest — Tempting because it confirms ischemia; wrong because this still fits a stable exertional pattern.
- Pain has the same intensity for 6 months with heavy exertion only — Tempting because chronicity can still feel concerning; wrong because unchanged exertional threshold supports stability.
- Pain now occurs at rest and episodes are lasting 20 minutes — Tempting and correct because rest pain with prolonged duration indicates possible ACS rather than stable angina.
- There is mild chest wall tenderness on palpation after exercise — Tempting because tenderness suggests a benign cause; wrong because this finding alone does not override the broader ischemic pattern.
Exam Traps & Differentiators
Most common wrong answer and why: The most common wrong answer is GERD or musculoskeletal chest pain when the stem includes one misleading clue like reflux history or chest wall tenderness. That is tempting because those clues are concrete and familiar. The discriminator is still predictable exertional provocation with relief after stopping activity.
| Looks similar | Why it fools learners | Single clue that separates it from stable angina | Best exam move |
|---|---|---|---|
| Unstable angina / NSTEMI | Both can have pressure and radiation | Rest pain, crescendo pattern, longer episodes, or acute change | Urgent ECG/troponin pathway, not routine outpatient testing |
| GERD | Burning epigastric discomfort may sound similar | Meal/recumbent trigger rather than reproducible exertion | Do not dismiss ischemia if exertional pattern dominates |
| Costochondritis | Pain may be localized and activity-related | Palpation reproducibility without demand-threshold pattern | Chest wall tenderness does not rule out CAD |
| Pericarditis | Chest pain with ECG changes can confuse | Pleuritic, positional pain improved by leaning forward | Think upcoming pericarditis topic |
| Aortic dissection | Chest pain plus hypertension is alarming | Abrupt tearing pain with pulse/BP asymmetry | Emergency imaging/escalation |
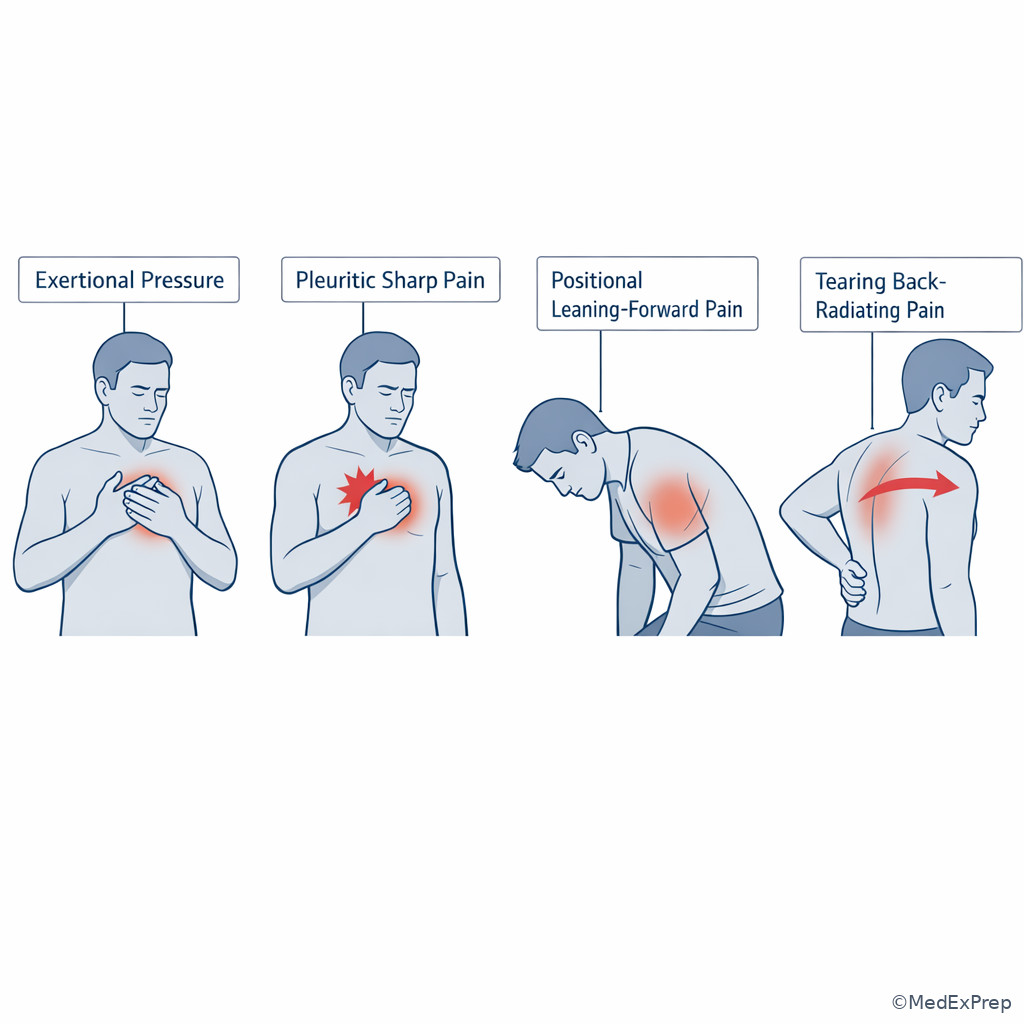
If the stem says...
- “Same pain every time he walks uphill” → think stable angina.
- “Now occurring while resting on the couch” → think ACS until proven otherwise.
- “Improves leaning forward” → think pericarditis.
- “Sudden tearing pain to the back with unequal arm pressures” → think aortic dissection.
- “Baseline ECG has paced rhythm/LBBB” → think do not choose plain exercise ECG.
- “Can exercise and ECG is interpretable” → think exercise ECG stress test.
Exam takeaway: The board answer often turns on one history phrase such as exertional, pleuritic, positional, or tearing.
Tables
| Medication/strategy | Main role | High-yield caution | Exam use case |
|---|---|---|---|
| Short-acting nitroglycerin | Rapid relief of episodes; pre-exertional use | Avoid with recent PDE-5 inhibitor use | Best for immediate symptom relief |
| Beta blocker | First-line chronic symptom control | Use caution with bradycardia, severe reactive airway disease, decompensated HF | Best first chronic antianginal in many stems |
| Calcium channel blocker | Alternative or add-on symptom control | Nondihydropyridines also slow rate | Use if beta blocker not tolerated or insufficient |
| Long-acting nitrate | Symptom prevention | Needs nitrate-free interval | Add when symptoms persist |
| High-intensity statin | Event reduction | Check for intolerance or interactions | Secondary prevention in CAD |
| Aspirin | Antiplatelet prevention when indicated | Balance bleeding risk and contraindications | Often paired with statin in known CAD |
| Testing scenario | Best next test | Why that test wins |
|---|---|---|
| Stable symptoms, can exercise, interpretable ECG | Exercise ECG stress test | Simple first-line physiologic evaluation |
| Stable symptoms, cannot exercise | Pharmacologic stress imaging | Provides ischemia assessment without exercise |
| Stable symptoms, can exercise, but paced rhythm/LBBB/baseline ST changes | Exercise stress imaging | Baseline ECG prevents reliable treadmill-only interpretation |
| Rest pain or crescendo symptoms | Urgent ACS evaluation | No longer a stable outpatient workup |
| Low-to-intermediate risk stable anatomy-focused question | Coronary CT angiography | Defines coronary anatomy in selected stable patients |
| Differential | Shared feature with stable angina | Discriminator | Common trap wording |
|---|---|---|---|
| Stable angina | Chest pressure | Predictable exertion, short duration, relief with rest | “Occurs after 2 blocks every time” |
| Unstable angina | Chest pressure | New/worsening or rest pain | “Now happening while watching TV” |
| Pericarditis | Chest discomfort | Pleuritic, positional, improved by leaning forward | “Worse supine, better sitting up” |
| Aortic dissection | Severe chest pain | Abrupt tearing pain, pulse deficit, BP asymmetry | “Sudden pain radiating to the back” |
| GERD | Burning chest/epigastric discomfort | Meal/position trigger, acid symptoms | “After late meal, sour taste” |
| Costochondritis | Chest pain | Localized tenderness reproducible by palpation | “Pain at left costochondral joint” |
Algorithm / Approach
Exam takeaway: Decide stability first, then select testing based on exercise ability and ECG readability, and always add prevention.
See Fig 6. This is the repeatable exam workflow: pattern -> stability -> test selection -> treatment -> safety reassessment.
Exam takeaway: Matching the stress test to exercise ability and baseline ECG prevents the classic testing error.
Rapid Review
- Stable angina → predictable exertional threshold with prompt relief after rest.
- Unstable angina → same ischemic quality but now at rest or crescendo.
- Typical angina → 3 of 3 classic features: substernal, exertional, rest-relieved.
- Atypical angina → 2 of 3 classic features, not automatically noncardiac.
- Normal resting ECG → does not exclude stable ischemia.
- Exercise treadmill ECG → only if can exercise and ECG is interpretable.
- Paced rhythm/LBBB → avoid plain treadmill ECG; choose imaging-based testing.
- Sublingual nitroglycerin → rescue relief, not sufficient long-term strategy alone.
- Beta blocker → common first-line chronic antianginal.
- Statin therapy → event reduction, not just lipid-number improvement.
- Chest wall tenderness → can coexist as noise; does not rule out CAD.
- GERD confounder → meal/recumbent trigger favors GI source over exertional ischemia.
- Pericarditis confounder → pleuritic and positional, better leaning forward.
- Aortic emergency confounder → abrupt tearing pain with asymmetry, not reproducible exertional threshold.
Self-check quiz
1. A 59-year-old man with hypertension and hyperlipidemia reports substernal pressure every time he climbs three flights of stairs. It resolves within 5 minutes of rest and has been unchanged for 5 months. Which is the most likely diagnosis?
- Stable angina
- Unstable angina
- Acute pericarditis
- Aortic dissection
2. A 63-year-old woman with diabetes has exertional chest pressure and is currently asymptomatic in clinic. She can exercise adequately, and her resting ECG is normal without conduction abnormalities. What is the most appropriate initial diagnostic test?
- Exercise ECG stress test
- Immediate coronary angiography
- Serial troponin testing
- Ventilation-perfusion scan
3. A 68-year-old woman with diabetes, obesity, bilateral knee osteoarthritis, and chronic exertional chest pressure presents for outpatient evaluation. Symptoms occur with brisk walking and resolve after 4 minutes of rest. Her ECG shows a paced rhythm. Which is the most appropriate next diagnostic step?
- Standard exercise treadmill ECG
- Pharmacologic stress imaging
- Empiric proton pump inhibitor trial only
- Reassurance without further evaluation
4. A 61-year-old man with known CAD, smoking history, and uncontrolled LDL has predictable chest pressure while shoveling snow. It resolves within minutes of rest. He takes no antianginal medications. Which is the best initial outpatient management plan?
- Sublingual nitroglycerin only
- Beta blocker, sublingual nitroglycerin, and high-intensity statin therapy
- Opioid analgesic as needed
- Immediate fibrinolytic therapy
5. A 56-year-old woman with diabetes and GERD reports “indigestion” and dyspnea every time she carries groceries upstairs. Symptoms last 6 minutes and improve with sitting. She also notes sour taste after large meals. Which detail most strongly supports an anginal source rather than GERD?
- Associated sour taste after meals
- Reproducible onset with exertion
- Epigastric location
- Burning quality
6. A 72-year-old man with diabetes, CKD, and prior smoking has 4 months of exertional chest pressure while walking uphill. Over the last 48 hours, he has had two 20-minute episodes at rest with diaphoresis. Mild left chest wall tenderness is present after lifting boxes. What is the most appropriate next step?
- Schedule outpatient exercise stress testing
- Begin NSAIDs for musculoskeletal chest pain
- Urgent ACS evaluation with ECG and troponin testing
- Increase exercise gradually and follow up in 1 month
7. A 65-year-old man with hypertension and exertional angina asks for treatment of recurrent episodes while walking uphill. He also used sildenafil last night. Which medication requires immediate clarification before prescribing because of a serious interaction risk?
- Sublingual nitroglycerin
- Metoprolol
- Atorvastatin
- Aspirin
8. A 58-year-old woman with hypertension, diabetes, and tobacco use reports chest discomfort. Which presentation most strongly supports stable angina rather than pericarditis, aortic dissection, or unstable angina?
- Sudden severe chest pain radiating to the back with asymmetric arm blood pressures
- Substernal pressure when climbing stairs that resolves after 3 minutes of rest, unchanged for months
- Pleuritic chest pain that improves when leaning forward
- Chest pressure at rest that is more frequent this week than last month
Answer key
1.1.1.8 1. Correct answer: A. Stable angina
A. Stable angina: Tempting because the story is classic for exertional myocardial oxygen supply-demand mismatch; correct because the pain is predictable, triggered by exertion, relieved by rest, and unchanged for months. The single stem clue is same exertional threshold with relief in minutes. Source: AHA/ACC chronic coronary disease guidance; Harrison’s Principles of Internal Medicine.
B. Unstable angina: Tempting because it is also ischemic chest pain; incorrect because unstable angina requires new, worsening, or rest symptoms rather than a fixed pattern. The single discriminator is unchanged pattern over 5 months. Source: AHA/ACC chest pain and chronic coronary disease guidance.
C. Acute pericarditis: Tempting because it can cause chest pain in adults; incorrect because pericarditis is usually pleuritic and positional, often improved by leaning forward. The single discriminator is exertion-triggered relief-with-rest pattern. Source: Harrison’s; ESC/AHA pericardial disease references.
D. Aortic dissection: Tempting because hypertension is present and chest pain can be catastrophic; incorrect because dissection causes abrupt severe tearing pain, often with neurologic symptoms or pulse asymmetry. The single discriminator is brief predictable exertional episodes over months. Source: AHA aortic disease guidance; Harrison’s.
1.1.1.9 2. Correct answer: A. Exercise ECG stress test
A. Exercise ECG stress test: Tempting because it is the standard stable-workup answer in the right patient; correct because she is stable, can exercise, and has an interpretable resting ECG. The single stem clue is exercise capacity plus normal baseline ECG. Source: AHA/ACC chronic coronary disease/chest pain guidance; UpToDate review of stable ischemic heart disease testing.
B. Immediate coronary angiography: Tempting because it is definitive anatomy testing; incorrect because stable patients without high-risk instability usually start with noninvasive evaluation. The discriminator is currently asymptomatic stable clinic presentation. Source: AHA/ACC guidance.
C. Serial troponin testing: Tempting because chest pain raises concern for ACS; incorrect because there is no acute evolving syndrome here. The discriminator is chronic exertional pattern without active acute episode. Source: AHA/ACC chest pain guideline.
D. Ventilation-perfusion scan: Tempting because dyspnea/chest symptoms can overlap with PE; incorrect because the presentation is classic exertional ischemia, not embolic disease. The discriminator is reproducible exertional substernal pressure. Source: Harrison’s; PE diagnostic guidance.
1.1.1.10 3. Correct answer: B. Pharmacologic stress imaging
A. Standard exercise treadmill ECG: Tempting because stable angina often leads to “treadmill” in memory; incorrect because her paced rhythm makes ECG ischemia interpretation unreliable and knee osteoarthritis limits exercise capacity. The discriminator is paced rhythm plus poor exercise ability. Source: AHA/ACC testing guidance.
B. Pharmacologic stress imaging: Tempting because it bypasses both exercise limitation and ECG interpretability issues; correct because she cannot reliably do an exercise test and the ECG is not readable for ST changes. The discriminator is cannot exercise adequately with uninterpretable ECG. Source: AHA/ACC chronic coronary disease guidance; UpToDate testing algorithms.
C. Empiric proton pump inhibitor trial only: Tempting because chest symptoms can be reflux-related; incorrect because the history is strongly exertional and consistent with ischemia. The discriminator is symptoms with brisk walking relieved by rest. Source: Harrison’s chest pain evaluation.
D. Reassurance without further evaluation: Tempting because symptoms are brief and self-limited; incorrect because multiple CAD risks and classic exertional pattern still warrant evaluation. The discriminator is high-probability ischemic pattern. Source: AHA/ACC chest pain guidance.
1.1.1.11 4. Correct answer: B. Beta blocker, sublingual nitroglycerin, and high-intensity statin therapy
A. Sublingual nitroglycerin only: Tempting because it gives immediate relief for exertional episodes; incorrect because it does not provide chronic antianginal control or reduce future ASCVD risk by itself. The discriminator is known CAD with uncontrolled LDL and recurrent exertional symptoms. Source: AHA/ACC chronic coronary disease guideline.
B. Beta blocker, sublingual nitroglycerin, and high-intensity statin therapy: Tempting because it addresses multiple goals; correct because it combines rescue symptom treatment, chronic demand reduction, and event prevention. The discriminator is question asks for best initial outpatient management, not just symptom rescue. Source: AHA/ACC chronic coronary disease guidance; Harrison’s.
C. Opioid analgesic as needed: Tempting because chest pain may prompt symptom-based treatment; incorrect because opioids do not treat ischemic mechanism and are not routine stable angina management. The discriminator is ischemic pathophysiology needing oxygen-demand reduction and prevention. Source: guideline-based CAD management.
D. Immediate fibrinolytic therapy: Tempting because coronary disease can progress to MI; incorrect because fibrinolysis is for STEMI scenarios, not stable outpatient angina. The discriminator is predictable exertional symptoms relieved by rest. Source: AHA/ACC ACS/STEMI guidance.
1.1.1.12 5. Correct answer: B. Reproducible onset with exertion
A. Associated sour taste after meals: Tempting because it supports reflux; incorrect because it points away from a cardiac source. The discriminator is GI-associated rather than demand-associated pattern. Source: Harrison’s differential diagnosis of chest pain.
B. Reproducible onset with exertion: Tempting because it is the classic ischemic trigger; correct because exertional reproducibility is the strongest feature favoring angina over GERD in this stem. The discriminator is carrying groceries triggers the symptoms consistently. Source: AHA/ACC chest pain guidance.
C. Epigastric location: Tempting because angina can present atypically; incorrect because location alone does not outperform exertional provocation as a discriminator. The single clue is location is less specific than trigger. Source: Harrison’s; AHA chest pain guidance.
D. Burning quality: Tempting because both reflux and atypical angina can burn; incorrect because quality alone is not the best separator. The discriminator is provocation pattern matters more than adjective choice. Source: AHA/ACC chest pain guidance.
1.1.1.13 6. Correct answer: C. Urgent ACS evaluation with ECG and troponin testing
A. Schedule outpatient exercise stress testing: Tempting because he has a long-standing exertional history that sounds like stable angina; incorrect because the pattern has changed to rest pain with longer episodes and diaphoresis. The discriminator is two 20-minute rest episodes in the last 48 hours. Source: AHA/ACC chest pain and ACS guidance.
B. Begin NSAIDs for musculoskeletal chest pain: Tempting because chest wall tenderness can suggest musculoskeletal pain; incorrect because the tenderness is distracting noise and does not explain the new rest diaphoresis episodes. The discriminator is progression to rest pain. Source: Harrison’s chest pain approach.
C. Urgent ACS evaluation with ECG and troponin testing: Tempting because the story is now unstable; correct because a change from chronic exertional symptoms to prolonged rest pain with diaphoresis requires urgent assessment for unstable angina/NSTEMI. The discriminator is crescendo/rest symptoms. Source: AHA/ACC ACS guidance.
D. Increase exercise gradually and follow up in 1 month: Tempting because exercise helps chronic CAD risk reduction; incorrect because this would dangerously delay evaluation of possible ACS. The discriminator is active instability, not chronic conditioning need. Source: AHA/ACC safety guidance.
1.1.1.14 7. Correct answer: A. Sublingual nitroglycerin
A. Sublingual nitroglycerin: Tempting because it is the standard rescue drug for angina; correct because nitrates combined with recent sildenafil can cause profound hypotension. The discriminator is sildenafil used last night. Source: AHA/ACC chronic coronary disease guidance; standard pharmacology references.
B. Metoprolol: Tempting because beta blockers affect blood pressure and heart rate; incorrect because the serious named interaction in this stem is not with sildenafil. The discriminator is PDE-5 interaction specifically implicates nitrates. Source: Harrison’s; pharmacology guidance.
C. Atorvastatin: Tempting because statins have many interaction questions; incorrect because sildenafil does not create the classic dangerous hypotension issue with statins. The discriminator is interaction risk type is hemodynamic collapse, not statin toxicity. Source: guideline-based CAD pharmacotherapy.
D. Aspirin: Tempting because bleeding risk often prompts medication clarification; incorrect because sildenafil does not create the hallmark contraindication here. The discriminator is nitrate-PDE-5 combination. Source: AHA/ACC guidance.
1.1.1.15 8. Correct answer: B. Substernal pressure when climbing stairs that resolves after 3 minutes of rest, unchanged for months
A. Sudden severe chest pain radiating to the back with asymmetric arm blood pressures: Tempting because it is very serious and chest-centered; incorrect because this is classic for aortic dissection. The discriminator is abrupt tearing back-radiating pain with asymmetry. Source: AHA aortic disease guidance.
B. Substernal pressure when climbing stairs that resolves after 3 minutes of rest, unchanged for months: Tempting because it is textbook stable ischemia; correct because it combines exertional trigger, short duration, relief with rest, and chronic reproducibility. The discriminator is unchanged exertional threshold over months. Source: AHA/ACC chronic coronary disease guidance; Harrison’s.
C. Pleuritic chest pain that improves when leaning forward: Tempting because pericarditis also causes chest pain; incorrect because positional pleuritic pain relieved by leaning forward points to pericarditis. The discriminator is positional improvement. Source: pericarditis references.
D. Chest pressure at rest that is more frequent this week than last month: Tempting because ischemic pressure is present; incorrect because increasing rest symptoms suggest unstable angina or ACS. The discriminator is rest pain with increasing frequency. Source: AHA/ACC ACS guidance.