Why it matters
- BCMTMS questions often test service structure before clinical detail; if you cannot identify the MTM element, you may choose the wrong next step even when the drug issue itself is obvious.
- MTM is not just “finding a problem.” It requires converting findings into patient-friendly outputs, pharmacist documentation, communication, and follow-up.
- Many distractors mix up what the patient receives versus what the pharmacist documents internally; knowing this split prevents easy point losses.
- These elements create the framework used repeatedly in later topics such as CMR versus TMR and PMR/MAP design.
Key Terms & Must-Know Facts
1.1.1.1 Key terms
- MTM: pharmacist-provided, patient-centered services to optimize therapeutic outcomes.
- APhA/NACDS Core Elements: the commonly taught five-part MTM service structure.
- Medication Therapy Review (MTR): structured review of medications to identify medication-related problems.
- Comprehensive Medication Review (CMR): complete, interactive review of the full regimen and medication experience.
- Targeted Medication Review (TMR): focused review of specific problems or gaps.
- Personal Medication Record (PMR): patient-facing medication list.
- Medication-Related Action Plan (MAP): patient-facing list of actions the patient should take.
- Intervention/Referral: communication to prescriber, caregiver, or other clinician when action beyond patient education is needed.
- Documentation: defensible record of assessment, findings, actions, and follow-up plan.
- Follow-up: planned reassessment after the MTM service.
- Medication-related problem: issue involving indication, effectiveness, safety, adherence, duplication, omission, or monitoring gap.
- Transitions of care: medication management during movement between settings.
1.1.1.2 Must-know facts
- The five core elements are MTR, PMR, MAP, intervention/referral, and documentation/follow-up.
- The PMR and MAP are patient-facing; documentation is primarily clinician/service-facing.
- An MTM encounter can identify a problem correctly yet still be incomplete if communication or follow-up is missing.
- The MAP is action-oriented; it tells the patient what to do, not the clinician what was assessed.
- The PMR should reflect what the patient is actually using, not just what is on file.
- Intervention/referral is required when the issue exceeds routine counseling or needs another clinician’s action.
- Documentation should support continuity, billing/workflow where applicable, and medicolegal defensibility.
- For BCMTMS, the pharmacist should choose clarify, recommend, communicate, monitor, refer, or escalate rather than act outside scope.
Exam takeaway: Use the five-element sequence to decide what output belongs to the patient, the prescriber, or the pharmacist record.
flowchart LR A[Medication Therapy Review] --> B[Personal Medication Record] A --> C[Medication-Related Action Plan] A --> D[Intervention or Referral] D --> E[Documentation and Follow-up] B --> E C --> E
See Fig 1 for the high-yield relationship among the five elements.
| Element | Primary audience | Main purpose | Common exam cue |
|---|---|---|---|
| MTR | Pharmacist and patient interaction | Identify medication-related problems | “Review the regimen and identify highest-priority problem” |
| PMR | Patient/caregiver | Current medication list for ongoing reference | “Provide an updated take-home medication list” |
| MAP | Patient/caregiver | Convert findings into patient action steps | “What should the patient do next?” |
| Intervention/Referral | Prescriber/care team/other clinician | Communicate recommended changes or need for evaluation | “Notify prescriber” or “refer urgently” |
| Documentation/Follow-up | Pharmacist/service record | Record what happened and plan reassessment | “Best documentation element” or “appropriate follow-up plan” |
Core content
1.1.1.3 Foundational structure: what the five MTM elements are and how they fit together
A Explanation
The first exam decision conflict is simple but heavily tested: is the stem asking about the review process, the patient handout, the clinician communication, or the service record? The single rule that resolves it is this: MTR is the assessment; PMR and MAP are patient-facing outputs; intervention/referral is the clinician-facing action; documentation/follow-up closes the loop. If you keep those buckets separate, most introductory MTM questions become straightforward.
WHY THIS IS TESTED: test writers often present one correct clinical idea but ask for the wrong deliverable. For example, a recommendation to obtain renal labs is not itself a MAP item unless written as a patient action; likewise, a medication list is not documentation just because the pharmacist created it.
In practical MTM workflow, the pharmacist begins with a medication therapy review, which may be comprehensive or focused. From that review come patient-facing tools: an accurate PMR and a prioritized MAP. If the pharmacist identifies a problem requiring action by another clinician, intervention or referral follows. The encounter is not complete until documentation captures the problem, recommendation, communication, and follow-up plan. See Fig 1.
B Worked example
A 71-year-old woman with type 2 diabetes, hypertension, and osteoarthritis brings metformin 1000 mg by mouth twice daily, lisinopril 20 mg daily, hydrochlorothiazide 25 mg daily, ibuprofen 400 mg three times daily as needed, and an outdated bottle of glyburide she says she “sometimes still takes.” She reports dizziness and missed meals, but her distracting laboratory value is a stable LDL of 82 mg/dL. During the pharmacist visit, the learner is asked which APhA/NACDS MTM element is best represented by “give the patient a current list of what she should and should not be taking.”
Reasoning chain: identify task → this is not asking for problem identification itself, but for a patient take-home tool. Extract key facts → multiple actual and outdated medications, so the patient needs an accurate medication list. Apply rule → the patient-facing current medication list is the PMR. Eliminate distractors → MAP would list actions such as “stop using old glyburide until clarified” or “call clinic about dizziness”; intervention/referral would be contact with the prescriber; documentation would be the pharmacist record. Verify → the request centers on a current list for patient reference, so PMR is best.
C Exam trap
WHY IT IS TEMPTING: The patient clearly needs to do something, and students often equate every patient handout with the MAP.
The SINGLE CLUE that eliminates it: The stem asks for a current list of medications, which is a PMR, not a task list.
D Checkpoint
Question: During an MTM visit, a pharmacist identifies duplicate NSAID use and gives the patient an updated list of all prescription and nonprescription products currently being taken. Which MTM element is most directly represented by that take-home list?
- A. Medication therapy review — Tempting because the list comes from the review, but the review is the assessment process, not the take-home document.
- B. Personal medication record — Correct because it is the patient-facing, updated medication list intended for ongoing reference.
- C. Medication-related action plan — Tempting because patient action is important, but this option would list tasks, not the regimen itself.
- D. Intervention/referral — Tempting because duplicate NSAID use may require prescriber contact, but the question asks about the list given to the patient.
1.1.1.4 MTR as the assessment engine: what the pharmacist is deciding during review
A Explanation
The second decision conflict is choosing between performing a review and acting on the review. The medication therapy review is the core analytic step. It is where the pharmacist collects, reconciles, and evaluates all available medication information to identify medication-related problems involving indication, effectiveness, safety, and adherence. The single finding that resolves many questions is whether the pharmacist is still analyzing the regimen or has already moved to output/action.
WHY THIS IS TESTED: MTM stems often include a clinically interesting issue—duplicate therapy, omitted statin, affordability barrier, or monitoring gap—but the actual question asks which MTM element is being performed. If the pharmacist is still identifying and prioritizing problems, that is MTR.
MTR is broad enough to include medication history verification, assessment of OTC and herbals, review of adherence and affordability, screening for high-risk use, and identification of preventive care gaps tied to medication management. It does not end with merely spotting a discrepancy; the pharmacist must prioritize issues based on urgency, safety, and feasibility. In later lessons, you will separate CMR versus TMR; for now, the key is that both are forms of review under the MTR umbrella. See Fig 2 for how assessment categories feed problem detection.
Exam takeaway: When the pharmacist is identifying indication, effectiveness, safety, or adherence problems, the service element is the medication therapy review.
flowchart TD
A[Medication list and patient interview] --> B{Assess domain}
B --> C[Indication]
B --> D[Effectiveness]
B --> E[Safety]
B --> F[Adherence]
C --> G[Need for therapy? Duplication?]
D --> H[Working? Right intensity?]
E --> I[Interactions? Contraindication? Monitoring?]
F --> J[Cost? Understanding? Access?]
G --> K[Prioritized problem list]
H --> K
I --> K
J --> K See Fig 2 for the four-domain lens used inside the MTR.
B Worked example
A 63-year-old man with heart failure, atrial fibrillation, and chronic kidney disease presents for an MTM visit after multiple refill gaps. His medications include apixaban 5 mg by mouth twice daily, furosemide 40 mg daily, metoprolol succinate 100 mg daily, and naproxen 220 mg twice daily purchased over the counter. He also reports taking “a water pill from years ago” but cannot identify it. A distracting clue is that he says his multivitamin is “heart healthy.” The pharmacist’s immediate task is to determine which MTM element best describes reviewing all current prescription, OTC, and leftover medications to identify duplicate diuretic use and NSAID-related safety risk.
Reasoning chain: identify task → the pharmacist is evaluating the regimen for problems. Extract key facts → unknown additional diuretic, OTC naproxen, CKD, heart failure, anticoagulant use. Apply rule → this is the medication therapy review. Eliminate distractors → PMR would be the final corrected list; MAP would tell the patient to stop self-adjusting or contact providers; intervention/referral would communicate findings to prescribers; documentation/follow-up would record the encounter. Verify → because the pharmacist is still in the analytic phase, MTR is best.
C Exam trap
WHY IT IS TEMPTING: The scenario contains a real safety issue, so learners jump immediately to prescriber communication.
The SINGLE CLUE that eliminates it: The stem asks about reviewing medications to identify the problems, which occurs during MTR before communication is executed.
D Checkpoint
Question: A pharmacist interviews a patient, reconciles pharmacy claims with pill bottles, and identifies nonadherence to rosuvastatin plus duplication between OTC ibuprofen and prescription meloxicam. Which MTM element is being performed at that moment?
- A. Medication therapy review — Correct because the pharmacist is actively gathering and assessing information to identify medication-related problems.
- B. Personal medication record — Tempting because the reconciled information may later populate the PMR, but the step described is assessment, not the handout.
- C. Medication-related action plan — Tempting because action steps will follow, but the stem has not yet shifted into a patient task list.
- D. Documentation/follow-up — Tempting because good MTM requires recording the findings, but the current activity is still the review itself.
- The MTM element that identifies medication-related problems is MTR.
- True or False: A PMR is primarily an internal documentation tool. False.
- Name the 4 core assessment domains used in review: indication, effectiveness, safety, adherence.
1.1.1.5 Patient-facing outputs: PMR and MAP are not interchangeable
A Explanation
The most common foundational confusion is mixing the personal medication record with the medication-related action plan. Both are patient-facing, but they solve different problems. The PMR answers: “What medicines am I using?” The MAP answers: “What should I do next?” That single rule resolves nearly every PMR-versus-MAP question.
WHY THIS IS TESTED: Exam stems often include a medication list and a task list in the same vignette. Distractors exploit learners who recognize that the patient needs both but cannot identify which document a given statement belongs in. The PMR should be accurate, current, and understandable to the patient. The MAP should be prioritized, actionable, and written in plain language.
Examples of PMR content include drug name, strength, directions, purpose if helpful, and special notes such as allergies or what the patient actually takes. Examples of MAP content include “Schedule your blood pressure check this week,” “Ask your doctor whether you should continue glyburide,” or “Use a pillbox and bring all medicines to the next visit.” MAP items should be framed as patient actions, not internal clinical commentary. See Fig 3.
Exam takeaway: If the content is “what you take,” choose PMR; if it is “what you should do,” choose MAP.
flowchart LR
A[Patient-facing item] --> B{Type of content}
B -->|Current medicine list| C[PMR]
B -->|Patient task or follow-up step| D[MAP]
C --> E[Drug name, dose, directions, notes]
D --> F[Call, schedule, bring, monitor, ask, avoid] See Fig 3 for the fastest test-day rule to separate PMR from MAP.
Exam takeaway: Visually separating the medication list from action steps reduces PMR-versus-MAP confusion on exam stems.

B Worked example
A 68-year-old man with COPD, coronary artery disease, and insomnia uses tiotropium daily, albuterol inhaler as needed, aspirin 81 mg daily, and diphenhydramine 50 mg nightly purchased over the counter. He reports “sometimes borrowing” his spouse’s omeprazole. The distracting clue is that his blood pressure today is controlled. The pharmacist completes an MTM visit and wants to provide two patient documents: one showing the actual current regimen, and one listing steps such as “stop using your spouse’s medicine,” “bring inhalers to the next visit,” and “ask your clinician about nighttime sleep options.”
Reasoning chain: identify task → two patient-facing outputs are needed. Extract key facts → one need is for an accurate regimen list; the other is for specific follow-up tasks. Apply rule → current regimen = PMR; next steps = MAP. Eliminate distractors → intervention/referral may still occur for anticholinergic burden or unsafe borrowing, but those are separate clinician communications. Verify → if the exam asks which element contains the stepwise patient tasks, the answer is MAP.
C Exam trap
WHY IT IS TEMPTING: Students see a patient-facing document and stop there.
The SINGLE CLUE that eliminates it: The statement is an action the patient should take, so it belongs in the MAP.
D Checkpoint
Question: Which statement best belongs in a patient’s medication-related action plan rather than the personal medication record?
- A. Metoprolol succinate 50 mg by mouth once daily for blood pressure — Tempting because it is patient-friendly, but it describes a medication entry and belongs in the PMR.
- B. Allergic reaction to sulfonamides: rash — Tempting because it is clinically important and may be listed with the PMR, but it is not a patient action step.
- C. Bring all prescription and over-the-counter medicines to your next visit — Correct because it is a plain-language action the patient should complete.
- D. Vitamin D 1000 units once daily — Tempting because supplements are often forgotten, but this is still a medication list item for the PMR.
1.1.1.6 Intervention, referral, documentation, and follow-up: closing the MTM loop
A Explanation
The final foundational decision conflict is choosing between educating the patient and taking the next professional action required to resolve the problem. Not every medication-related problem can be solved within the patient conversation alone. If the issue requires a prescriber’s order, diagnostic workup, urgent evaluation, or care-team coordination, the pharmacist must perform intervention/referral. After that, the pharmacist must document the encounter and establish follow-up.
WHY THIS IS TESTED: many stems reward candidates who can recognize when the pharmacist’s role is to recommend, clarify, refer, or escalate rather than independently change therapy. Just as important, many stems test whether follow-up is specific enough to ensure continuity.
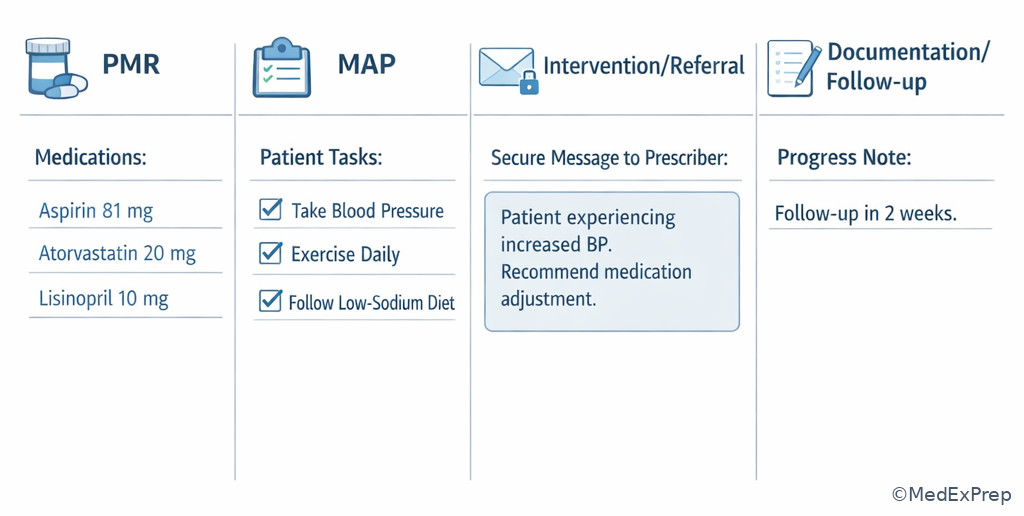
Intervention/referral includes communicating suggestions such as dose reassessment, need for lab monitoring, duplicate therapy resolution, refill-gap discussion, or urgent symptom evaluation. Documentation should capture the identified problem, the rationale, who was contacted, what was recommended, patient education provided, and planned follow-up. Follow-up must match risk: a life-threatening issue requires immediate escalation; a routine adherence aid can be reassessed later. See Fig 4 for the decision path. This section is where MTM most clearly intersects with professional scope: the pharmacist acts decisively, but within authority.
Exam takeaway: When a finding requires another clinician’s action or urgent evaluation, choose intervention/referral first, then document and arrange follow-up.
flowchart TD
A[Problem identified during MTR] --> B{Can patient self-act safely?}
B -->|Yes| C[Add to MAP and counsel]
B -->|No| D[Intervention or referral]
D --> E{Urgent risk?}
E -->|Yes| F[Immediate escalation]
E -->|No| G[Routine prescriber communication]
C --> H[Document]
F --> H
G --> H
H --> I[Follow-up plan] See Fig 4 for the choose-versus-escalate logic.
Exam takeaway: MTM is incomplete without a defensible note and clear communication plan when another clinician must act.

B Worked example
A 76-year-old woman with atrial fibrillation, heart failure, and recent hospital discharge is seen in community MTM. Her list includes warfarin 5 mg nightly, amiodarone 200 mg daily, furosemide 20 mg daily, and trimethoprim-sulfamethoxazole started yesterday at urgent care. She reports gum bleeding and dark stools but says she mainly came in to ask about a calcium supplement. The distracting clue is that she also forgot one warfarin dose last week. The pharmacist must choose the most appropriate MTM action.
Reasoning chain: identify task → urgent safety triage within pharmacist scope. Extract key facts → warfarin plus TMP-SMX interaction, bleeding symptoms, recent discharge, amiodarone interaction. Apply rule → this exceeds simple counseling; urgent evaluation/referral is needed, then documentation and communication. Eliminate distractors → updating the PMR is necessary but not sufficient; adding a MAP item alone delays urgent care; merely documenting without escalation is unsafe. Verify → the highest-priority MTM element now is intervention/referral with immediate escalation, followed by documentation/follow-up.
C Exam trap
WHY IT IS TEMPTING: MAP feels patient-centered and follow-up-oriented.
The SINGLE CLUE that eliminates it: Dark stools and bleeding signal urgent safety risk, so immediate referral/escalation is required.
D Checkpoint
Question: During an MTM encounter, a pharmacist finds that a patient recently started clarithromycin while taking simvastatin 40 mg nightly and is now reporting new severe muscle pain and weakness. What is the most appropriate MTM element to prioritize first?
- A. Personal medication record — Tempting because the list needs updating, but it does not address the immediate safety concern.
- B. Medication-related action plan — Tempting because the patient needs instructions, but clinician-level and urgent action come first.
- C. Intervention/referral — Correct because a serious interaction with concerning symptoms requires prompt communication and urgent evaluation.
- D. Documentation/follow-up — Tempting because every encounter must be documented, but documentation follows the urgent safety action.
- The most urgent MTM action when a dangerous interaction causes alarming symptoms is intervention/referral.
- True or False: Documentation can replace communication if the pharmacist note is detailed enough. False.
- Name the 3 core closure items after a clinician-facing recommendation: document, communicate, follow up.
1.1.1.7 Integration: using the MTM elements to choose the best next step in board-style cases
A Explanation
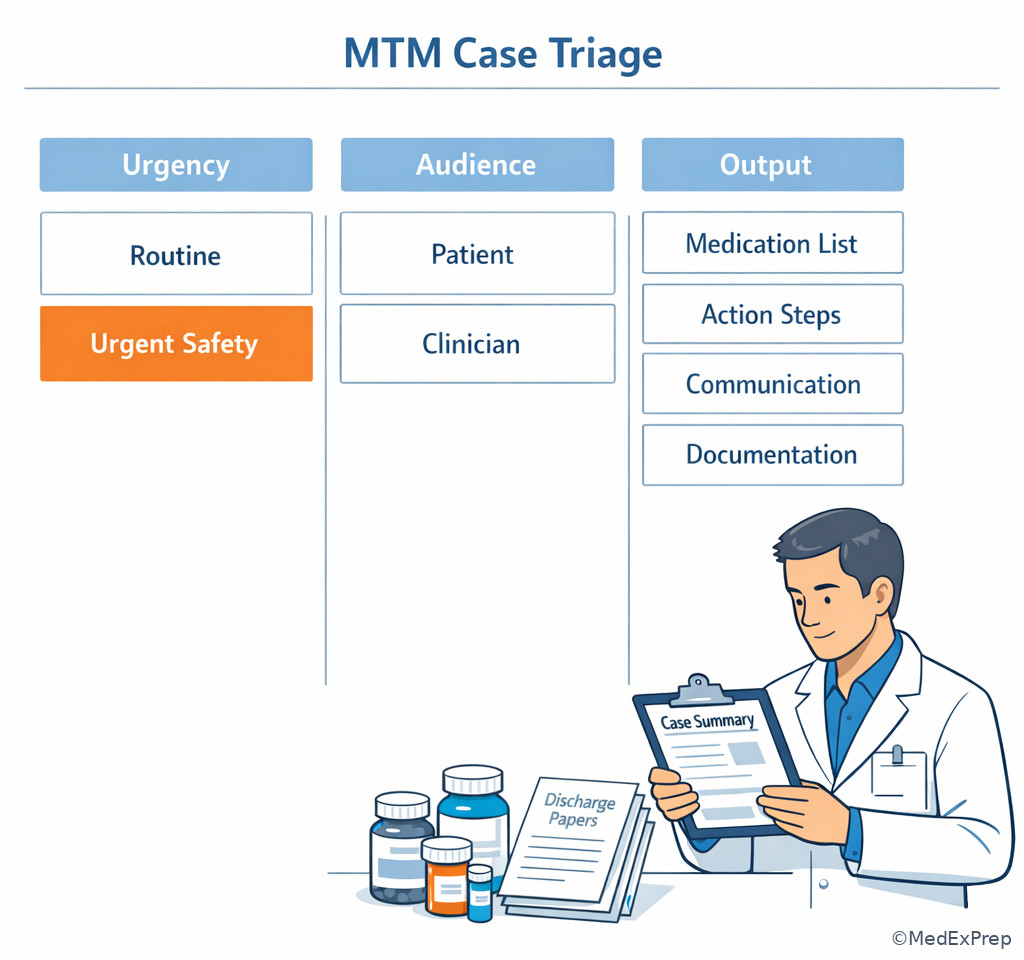
Once you know the five elements, the board-style challenge becomes integration: which element is the best answer for this exact moment in the case? The resolving rule is to identify the task the pharmacist must complete next, not every reasonable activity that could eventually happen. In most questions, multiple MTM elements are appropriate over the full encounter. The exam asks for the highest-priority next step.
WHY THIS IS TESTED: realistic MTM practice is sequential. A patient may need an MTR, PMR, MAP, prescriber communication, and follow-up—all in one episode. The test discriminates whether you can choose the first necessary action based on urgency, audience, and scope.
A reliable strategy is: identify urgency first; then identify audience; then identify output. If there is immediate danger, choose intervention/referral. If the pharmacist is still detecting problems, choose MTR. If the patient needs a current list, choose PMR. If the patient needs task-oriented instructions, choose MAP. If the question is about defensible recordkeeping or continuity, choose documentation/follow-up. See Fig 5.
Exam takeaway: In integrated cases, choose the MTM element that matches the immediate task, not every action that will eventually occur.
flowchart TD
A[Board-style MTM case] --> B{Urgent safety issue?}
B -->|Yes| C[Intervention or referral]
B -->|No| D{Still identifying problems?}
D -->|Yes| E[MTR]
D -->|No| F{Need patient output?}
F -->|Medication list| G[PMR]
F -->|Action steps| H[MAP]
C --> I[Document and follow-up]
E --> I
G --> I
H --> I See Fig 5 for a compact test-day algorithm.
Exam takeaway: Sorting the case by urgency, audience, and output quickly narrows the correct MTM element.
B Worked example
A 59-year-old woman with diabetes, depression, and recent hospitalization for pneumonia comes for an MTM visit with metformin 1000 mg twice daily, insulin glargine 20 units nightly, sertraline 100 mg daily, and prednisone 40 mg daily started 2 days ago. She forgot her hospital discharge papers and says she might still be taking her old glipizide. Her distracting clue is that she asks whether she should take vitamins with breakfast. The pharmacist identifies possible duplicate diabetes therapy, steroid-related hyperglycemia risk, and uncertainty about what was stopped at discharge.
Reasoning chain: identify task → if asked for the first structured MTM step, the pharmacist must clarify the active regimen and identify problems. Extract key facts → possible duplicate therapy and incomplete discharge information. Apply rule → the best next MTM element is MTR. Eliminate distractors → PMR cannot be accurate until the regimen is verified; MAP would be premature before clarification; intervention/referral may come later if unsafe overlap is confirmed; documentation follows the review. Verify → best answer is the review process first.
C Exam trap
WHY IT IS TEMPTING: The patient clearly needs a clean medication list after hospitalization.
The SINGLE CLUE that eliminates it: The current regimen is still uncertain; the pharmacist must perform MTR and reconciliation before the PMR can be accurate.
D Checkpoint
Question: A patient asks, “What exactly should I do before my next doctor’s visit?” The pharmacist has already completed medication review, updated the regimen list, and sent a recommendation to the prescriber. Which MTM element best addresses the patient’s question?
- A. Medication therapy review — Tempting because it generated the findings, but the review phase is already complete.
- B. Personal medication record — Tempting because the regimen list helps the patient, but the question asks for action steps rather than medication details.
- C. Medication-related action plan — Correct because it converts findings into specific patient tasks to complete before follow-up.
- D. Documentation/follow-up — Tempting because the encounter needs closure, but this answer does not directly give the patient next actions.
Exam Traps & Differentiators
Most common wrong answer and why: MAP instead of PMR. This is tempting because both are patient-facing and often delivered together. The discriminator is whether the content describes the current medication regimen or tells the patient what to do next.
| Looks similar | Why learners confuse it | Single clue that separates it | Correct MTM element |
|---|---|---|---|
| Updated medication list vs task list | Both are patient handouts | Medication details = list; action verbs = tasks | PMR vs MAP |
| Finding a discrepancy vs calling the prescriber | Both occur in the same encounter | Identifying the issue = review; communicating change = intervention | MTR vs intervention/referral |
| Note in chart vs message to clinician | Both are professional communications | Internal record = documentation; external action request = intervention | Documentation vs intervention/referral |
| Patient education vs urgent triage | Both involve advising the patient | Red-flag symptoms or toxic interaction require escalation | Intervention/referral |
| Creating PMR before reconciliation | Patient needs a list quickly | Uncertain regimen means review first | MTR first |
If the stem says ... think ...
- “Provide the patient with a current list” → think PMR.
- “Tell the patient what to do before the next visit” → think MAP.
- “Review all medications to identify problems” → think MTR.
- “Communicate recommendation to prescriber” → think intervention/referral.
- “Record the encounter and plan reassessment” → think documentation/follow-up.
- “New dangerous symptoms or severe interaction” → think urgent referral/escalation before routine documentation.
Exam takeaway: Side-by-side visual cues help separate patient handouts, clinician communication, and internal documentation.
Related confusable pairs from upcoming topics include CMR versus TMR and PMR versus MAP design. Those later lessons go deeper into review scope and document construction, but the trap here is more basic: know which element the stem is asking about before worrying about format details.
Tables
| Key fact/value table | High-yield point |
|---|---|
| Number of core APhA/NACDS MTM elements | 5 |
| Patient-facing elements | PMR and MAP |
| Assessment element | MTR |
| Clinician-facing action element | Intervention/referral |
| Closure element | Documentation/follow-up |
| Priority rule | Urgent safety issues outrank routine education and paperwork |
| Best PMR cue | Current medication list the patient can use |
| Best MAP cue | Plain-language patient action steps |
| Comparison item | PMR | MAP | Documentation/follow-up |
|---|---|---|---|
| Primary user | Patient/caregiver | Patient/caregiver | Pharmacist/care team record |
| Main question answered | What do I take? | What should I do? | What happened and what is next? |
| Typical content | Name, dose, directions, notes | Call, schedule, bring, avoid, monitor | Problem, recommendation, communication, follow-up |
| Exam distractor | Chosen for any patient handout | Chosen for any patient-friendly sentence | Chosen when clinician communication is actually needed |
| Best discriminator | Regimen list | Action verb | Record + reassessment plan |
| Case cue | Likely classification | Why |
|---|---|---|
| Pharmacist compares bottles, claims, and interview to identify duplicate therapy | MTR | Assessment and problem detection are occurring |
| Patient receives a corrected home medication list after discharge clarification | PMR | Current regimen is being presented to the patient |
| Patient receives instructions to bring inhalers and schedule A1c testing | MAP | Action steps are directed to the patient |
| Pharmacist contacts prescriber about ACE inhibitor omission | Intervention/referral | Another clinician must act on the recommendation |
| Pharmacist records problem list, recommendation, and 2-week reassessment | Documentation/follow-up | The service is being closed and tracked |
| Patient on warfarin reports melena after interacting antibiotic started | Urgent intervention/referral first | Safety escalation outranks routine handouts and note completion |
Algorithm / Approach
Exam takeaway: A simple urgency-audience-output checklist prevents choosing a technically correct but mistimed MTM element.
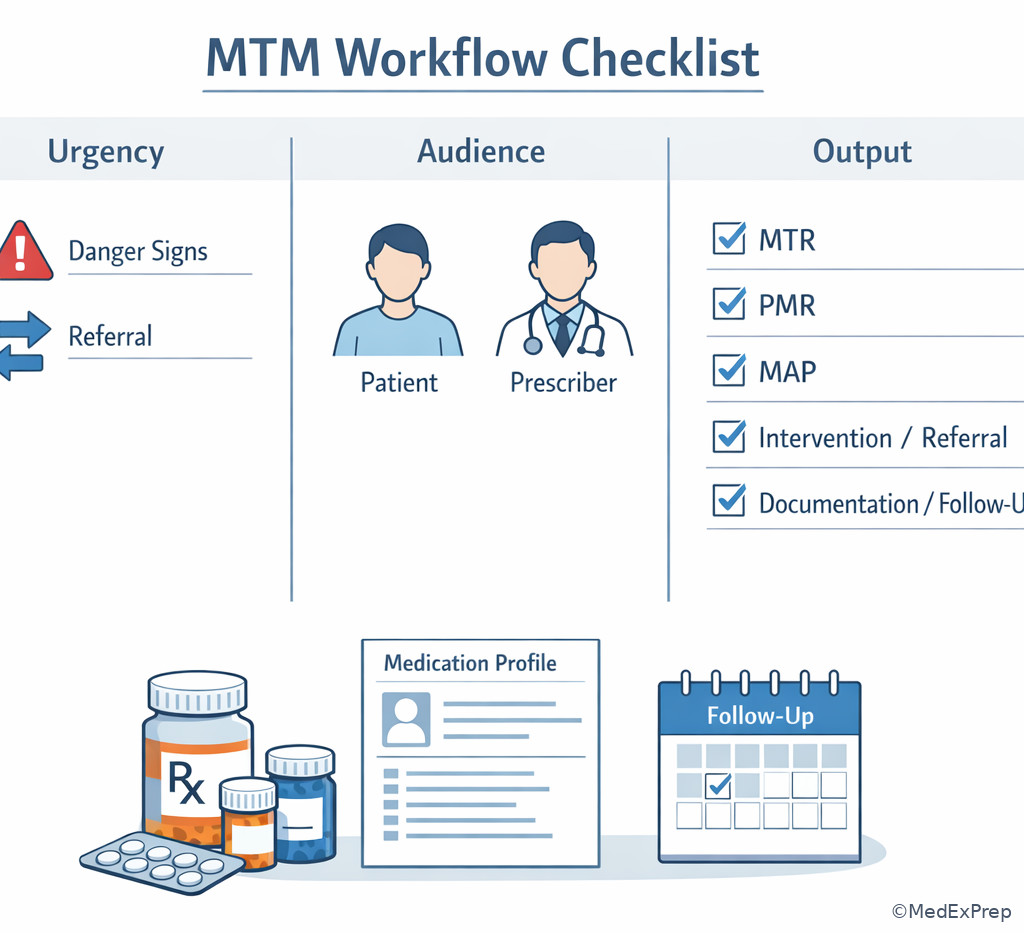
See Fig 6 as a compact exam-day mental checklist.
Rapid Review
- MTR → identifies problems; not the same as the final recommendation.
- PMR → current medication list; think “what I take.”
- MAP → patient task list; think action verbs.
- Intervention/referral → another clinician must act or patient needs urgent evaluation.
- Documentation/follow-up → closes the loop and supports continuity.
- Urgent symptom + interaction → escalate before routine paperwork.
- Unclear discharge regimen → reconcile and review before generating PMR.
- Patient handout with drug names and directions → PMR, not MAP.
- Patient handout with “call,” “bring,” or “schedule” → MAP, not PMR.
- Prescriber message recommending change → intervention/referral, not documentation alone.
- Found the issue but did not communicate it → MTM process incomplete.
- Good note but no follow-up for unresolved issue → closure gap.
Self-check quiz
1. A pharmacist completes an MTM visit for a 67-year-old man with hypertension and hyperlipidemia taking amlodipine 10 mg by mouth daily and atorvastatin 40 mg by mouth nightly. The patient asks for a take-home list of all medications, doses, and directions. Which is the most appropriate MTM element?
- A. Medication therapy review
- B. Personal medication record
- C. Medication-related action plan
- D. Documentation/follow-up
2. A pharmacist has already reviewed a patient’s regimen and updated the medication list. The patient taking lisinopril 20 mg by mouth daily and metformin 500 mg by mouth twice daily asks, “What should I do before my next appointment?” Which MTM element best answers that question?
- A. Medication therapy review
- B. Personal medication record
- C. Medication-related action plan
- D. Intervention/referral
3. A 74-year-old woman with CKD and osteoarthritis brings losartan 50 mg by mouth daily, meloxicam 15 mg by mouth daily, ibuprofen 400 mg by mouth three times daily as needed, and an old bottle of naproxen. Her serum creatinine from last month is mildly elevated, and the distracting detail is that she also asks about fish oil. The pharmacist compares all bottles with pharmacy fill history to identify duplicate NSAID use. Which MTM element is being performed?
- A. Medication therapy review
- B. Personal medication record
- C. Intervention/referral
- D. Documentation/follow-up
4. A 69-year-old man with diabetes and coronary disease takes metformin 1000 mg by mouth twice daily, insulin glargine 18 units subcutaneously nightly, and aspirin 81 mg daily. After the review, the pharmacist writes “Bring your glucose log, schedule your eye exam, and ask your clinician whether glipizide should remain discontinued.” Which MTM element is this?
- A. Personal medication record
- B. Medication-related action plan
- C. Intervention/referral
- D. Documentation/follow-up
5. A 72-year-old patient with atrial fibrillation and hypothyroidism takes warfarin 5 mg by mouth nightly and levothyroxine 75 mcg by mouth every morning. The patient was started on trimethoprim-sulfamethoxazole yesterday and now reports nosebleeds and dark stools; the distracting detail is that one warfarin dose was missed last week. What is the most appropriate next MTM action?
- A. Update the PMR first, then reassess in 1 month
- B. Add “watch for bleeding” to the MAP and follow up next week
- C. Perform intervention/referral for urgent evaluation, then document and follow up
- D. Complete routine documentation and wait for the prescriber to call back if concerned
6. A 61-year-old woman with heart failure, diabetes, and recent discharge takes carvedilol 12.5 mg by mouth twice daily, furosemide 40 mg by mouth daily, metformin 1000 mg by mouth twice daily, and prednisone 20 mg by mouth daily started in the hospital. She thinks she may also still be taking her old glyburide, and she did not bring discharge paperwork. The distracting detail is that she also asks whether magnesium supplements are safe. Which is the most appropriate MTM element to prioritize first?
- A. Personal medication record
- B. Medication-related action plan
- C. Medication therapy review
- D. Documentation/follow-up
7. A 78-year-old man with coronary artery disease, GERD, and chronic insomnia takes clopidogrel 75 mg by mouth daily, omeprazole 40 mg by mouth daily, and diphenhydramine 50 mg by mouth nightly. After the pharmacist identifies a potential interaction concern and inappropriate OTC use, which option best represents intervention/referral rather than MAP or documentation?
- A. “Bring all over-the-counter products to your next visit.”
- B. “I will send a recommendation to your clinician about the PPI and sedating OTC use.”
- C. “Current medications: clopidogrel 75 mg daily, omeprazole 40 mg daily, diphenhydramine 50 mg nightly.”
- D. “Problem identified, patient counseled, follow up in 2 weeks.”
8. A 70-year-old woman with hypertension, COPD, and depression uses tiotropium inhaled once daily, albuterol inhaled as needed, sertraline 100 mg by mouth daily, and leftover clonazepam 0.5 mg by mouth nightly from an old prescription. She reports increased falls and confusion, but the distracting detail is that her inhaler refill dates are on time. The pharmacist has already reviewed the regimen and updated the medication list. Which is the most appropriate next MTM element if the pharmacist wants the patient to stop using old sedatives and bring all bottles to the next appointment?
- A. Medication-related action plan
- B. Personal medication record
- C. Medication therapy review
- D. Documentation/follow-up
Answer key
1.1.1.8 1. Answer: B. Personal medication record
- A. Medication therapy review: Tempting because the list comes from the review. Incorrect for this scenario because the stem asks for the take-home list itself, not the assessment process. Single clue: “take-home list of all medications, doses, and directions.” Source support: APhA/NACDS Core Elements and DiPiro’s MTM framework emphasize PMR as the patient medication list.
- B. Personal medication record: Correct because the PMR is the patient-facing record of current medications, doses, and directions. The functional rationale is workflow-based rather than PK-based: it provides a reconciled regimen reference for safe use. Single clue: “list of all medications, doses, and directions.” Source support: APhA/NACDS MTM Core Elements; ASHP medication management documentation principles.
- C. Medication-related action plan: Tempting because patient counseling usually includes next steps. Incorrect because the MAP is task-oriented, not a regimen list. Single clue: no action verbs such as call, schedule, bring, monitor. Source support: APhA/NACDS Core Elements.
- D. Documentation/follow-up: Tempting because the pharmacist must record the service. Incorrect because documentation is the internal record and plan, not the patient’s medication list. Single clue: patient asks for a take-home list. Source support: ASHP and APhA MTM documentation standards.
1.1.1.9 2. Answer: C. Medication-related action plan
- A. Medication therapy review: Tempting because review precedes recommendations. Incorrect because the stem states the review is already done. Single clue: “has already reviewed a patient’s regimen.” Source support: APhA/NACDS sequencing of MTM elements.
- B. Personal medication record: Tempting because it is patient-facing. Incorrect because the question asks what the patient should do next, not what they take. Single clue: “What should I do before my next appointment?” Source support: APhA/NACDS Core Elements.
- C. Medication-related action plan: Correct because the MAP translates review findings into patient action steps. Operationally, it improves execution of care plan tasks and adherence behaviors. Single clue: asks for next actions. Source support: APhA/NACDS Core Elements; Lexicomp patient-care workflow references support task-oriented counseling tools.
- D. Intervention/referral: Tempting because some actions may involve another clinician. Incorrect because the question is specifically about what the patient should do. Single clue: patient-directed wording. Source support: APhA/NACDS MTM framework.
1.1.1.10 3. Answer: A. Medication therapy review
- A. Medication therapy review: Correct because the pharmacist is comparing medication sources to identify duplicate NSAID use and safety risk. Clinically, NSAID duplication increases toxicity risk, but the MTM element tested is the analytic review step. Single clue: “compares all bottles with pharmacy fill history to identify.” Source support: APhA/NACDS Core Elements; DiPiro on medication assessment workflow.
- B. Personal medication record: Tempting because a corrected list will eventually be needed. Incorrect because the pharmacist has not yet finished analyzing which agents are current and problematic. Single clue: still identifying the issue. Source support: APhA/NACDS.
- C. Intervention/referral: Tempting because CKD plus multiple NSAIDs may require clinician communication. Incorrect because the stem centers on the review activity before communication. Single clue: no communication has yet occurred. Source support: APhA/NACDS.
- D. Documentation/follow-up: Tempting because the findings should be recorded. Incorrect because the stem is not about recording or planning reassessment. Single clue: active medication comparison is underway. Source support: ASHP documentation guidance.
1.1.1.11 4. Answer: B. Medication-related action plan
- A. Personal medication record: Tempting because it is patient-facing and may include diabetes medicines. Incorrect because the listed statements are not drug entries but tasks. Single clue: all statements use action language. Source support: APhA/NACDS Core Elements.
- B. Medication-related action plan: Correct because the tasks are specific patient actions: bring logs, schedule exams, ask clinician about therapy status. These improve execution and continuity after the review. Single clue: “Bring,” “schedule,” and “ask.” Source support: APhA/NACDS; ASHP ambulatory care patient education frameworks.
- C. Intervention/referral: Tempting because one task mentions asking the clinician about glipizide. Incorrect because the document is still directed to the patient rather than being a pharmacist-to-prescriber communication. Single clue: patient-oriented wording. Source support: APhA/NACDS.
- D. Documentation/follow-up: Tempting because follow-up planning is implied. Incorrect because documentation would record the encounter internally; this is a patient task list. Single clue: intended for patient use. Source support: APhA/NACDS and ASHP documentation practices.
1.1.1.12 5. Answer: C. Perform intervention/referral for urgent evaluation, then document and follow up
- A. Update the PMR first, then reassess in 1 month: Tempting because an accurate list matters after a new antibiotic is added. Incorrect because the interaction between warfarin and trimethoprim-sulfamethoxazole can raise INR and bleeding risk quickly, and the patient already has bleeding symptoms. Single clue: “nosebleeds and dark stools.” Source support: Lexicomp interaction monograph; FDA warfarin labeling.
- B. Add “watch for bleeding” to the MAP and follow up next week: Tempting because MAP is patient-centered and addresses bleeding. Incorrect because symptomatic possible GI bleeding requires urgent evaluation, not delayed self-monitoring. Single clue: active bleeding symptoms. Source support: Lexicomp; Clinical Pharmacology; standard anticoagulation safety guidance.
- C. Perform intervention/referral for urgent evaluation, then document and follow up: Correct because the PD/clinical issue is a high-risk interaction plus alarming symptoms, requiring prompt escalation within pharmacist scope. Documentation and follow-up still matter but come after initiating urgent action. Single clue: warfarin + TMP-SMX with dark stools. Source support: FDA labeling, Lexicomp, and ACCP antithrombotic safety principles.
- D. Complete routine documentation and wait for the prescriber to call back if concerned: Tempting because thorough notes are expected. Incorrect because documentation cannot substitute for urgent triage. Single clue: time-sensitive bleeding risk. Source support: ASHP patient safety principles; Lexicomp interaction severity guidance.
1.1.1.13 6. Answer: C. Medication therapy review
- A. Personal medication record: Tempting because discharge confusion makes a medication list urgently useful. Incorrect because the regimen is not yet verified; a PMR built too early may perpetuate errors. Single clue: “she may also still be taking her old glyburide” and lacks discharge paperwork. Source support: APhA/NACDS; ASHP medication reconciliation principles.
- B. Medication-related action plan: Tempting because the patient will need instructions about diabetes monitoring and discharge follow-through. Incorrect because the pharmacist must first determine the true active regimen and safety issues. Single clue: uncertainty precedes action planning. Source support: APhA/NACDS.
- C. Medication therapy review: Correct because the immediate need is to reconcile and assess the regimen for possible duplicate sulfonylurea use and steroid-related hyperglycemia risk. From a medication-management standpoint, this is the foundational analytic step. Single clue: unclear active medication regimen after discharge. Source support: APhA/NACDS Core Elements; DiPiro and ASHP transitions-of-care medication review guidance.
- D. Documentation/follow-up: Tempting because a transition-of-care visit requires tracking. Incorrect because the pharmacist does not yet have enough clarified information for accurate closure. Single clue: unresolved uncertainty at the start of the encounter. Source support: ASHP documentation standards.
1.1.1.14 7. Answer: B. “I will send a recommendation to your clinician about the PPI and sedating OTC use.”
- A. “Bring all over-the-counter products to your next visit.” Tempting because it is good advice and supports future medication review. Incorrect because it is a patient task and therefore MAP content. Single clue: patient instruction phrased as a task. Source support: APhA/NACDS.
- B. “I will send a recommendation to your clinician about the PPI and sedating OTC use.” Correct because this is pharmacist-to-clinician communication about optimizing therapy and reducing risk. The clinical rationale is that clopidogrel/PPI selection and anticholinergic sedative burden may require prescriber review or regimen change. Single clue: direct recommendation to clinician. Source support: Lexicomp interaction resources; APhA/NACDS intervention/referral element.
- C. “Current medications: clopidogrel 75 mg daily, omeprazole 40 mg daily, diphenhydramine 50 mg nightly.” Tempting because it contains medication names and doses. Incorrect because it is a PMR-style entry, not clinician communication. Single clue: medication list format. Source support: APhA/NACDS PMR element.
- D. “Problem identified, patient counseled, follow up in 2 weeks.” Tempting because it sounds professional and complete. Incorrect because it is documentation/follow-up language, not the intervention itself. Single clue: internal note style. Source support: ASHP documentation guidance; APhA/NACDS.
1.1.1.15 8. Answer: A. Medication-related action plan
- A. Medication-related action plan: Correct because the review and PMR are already complete, and the pharmacist now wants the patient to take specific next steps: stop using old sedatives and bring all bottles. The management logic is task-oriented and patient-facing. Single clue: explicit patient actions after review completion. Source support: APhA/NACDS Core Elements.
- B. Personal medication record: Tempting because the medication list has been updated. Incorrect because the stem asks for patient tasks, not list content. Single clue: “stop using” and “bring all bottles.” Source support: APhA/NACDS PMR versus MAP distinction.
- C. Medication therapy review: Tempting because falls and confusion imply safety assessment. Incorrect because the stem states the pharmacist has already reviewed the regimen. Single clue: review already done. Source support: APhA/NACDS sequencing.
- D. Documentation/follow-up: Tempting because these actions should also be recorded and reassessed. Incorrect because the question asks for the element used to tell the patient what to do next. Single clue: patient instruction focus. Source support: ASHP documentation principles; APhA/NACDS.